IJCRR - 5(24), December, 2013
Pages: 27-33
Date of Publication: 31-Dec-2013
Print Article
Download XML Download PDF
COMPARATIVE STUDY OF TREATMENT OF UNSTABLE INTERTROCHANTERIC FRACTURE WITH SIMPLE DYNAMIC HIP SCREW AND LOCKING DYNAMIC HIP SCREW IN ELDERLY PATIENTS
Author: Nitin Sanadhya, Abhinav Likhyani
Category: Healthcare
Abstract:Aim: Is to evaluate the outcome of locking dynamic hip screw in comparison to standard dynamic hip screw in terms of fracture union, implant failure, range of movement of hip joint in unstable intertrochanteric fractures in elderly patients (age > 65 years), and to assess the hip function using modified Harris hip score. Methodology: This is a prospective randomized comparative study comprises of unstable intertrochanteric fracture of femur treated with dynamic hip screw and locking dynamic hip screw. The cases were selected randomly for fixation with Dynamic Hip Screw (DHS) and Locking Dynamic Hip Screw. The series consist of 50 cases divided in 2 groups. The group 1 consist of 25 cases treated by DHS and group 2 consist of another 25 cases treated by Locking DHS. The cases were followed up for minimum of 6 month duration Result and Observations: Most common mode of trauma in both groups of patients was slip (60%).Mean of Singh Index in group 1st cases was 3.64 \? 0.68 while mean of Singh Index in group 2nd was 3.56 \? 0.57.There were 5 cases (22.73%) of varus deformity in group 1st patients and 4 cases (19.05%) of varus deformity in group 2nd patients, although there were no significant varus deformity > 10º in both groups.2 cases of nonunion was seen in group 1st patients. In DHS group there was one case each of side plate pull out and screw cut out. No implant failure was seen in locking DHS. This study showed that functional outcome deteriorated when patients were more osteoporotic. Final outcome assessed using Modified Harris Hip Score. In group 1st there were 4.76% excellent, 86.37% good to fair and 9.09 % poor results, whereas in group 2nd cases 9.52% excellent, 85.71% good to fair and 4.77% was poor. Mean of Modified Harris Hip Score in group 1st was 68.33 \? 8.66 while 70.83 \? 8.35 in group 2nd cases. Conclusion: Keeping in mind of osteoporosis in geriatric population Locking DHS have some advantage in term of less chance of implant failure and functional outcome of the cases based on Harris hip score were slightly better, however they not statistically significant.
Keywords: unstable intertrochanteric fracture, simple dynamic hip screw, elderly patients
Full Text:
INTRODUCTION
Intertrochanteric fractures account for nearly 50% of all the proximal femoral fractures. Generally patients age group lies in 6th to 8th decade. The factors associated with intertrochanteric fractures include advancing age, increased number of comorbidties and history of other osteoporosis related fractures.
Sliding hip screw which is used commonly for fixation of these fractures has different biomechanical principles of fixation based on their fracture patterns. In stable fracture pattern the hip screw acts only as a lateral tension band, hence less chance of fixation failure. In unstable fracture pattern it allows controlled collapse and impaction of fragments, with shortening of lever arm acting on implant, it decreases the bending moment and thus decreasing the risk of mechanical failure. But while treating unstable intertrochanteric fracture with sliding hip screw in older patients, when sliding occurs in great amount, there is increased risk of fixation failure.
Fixation failure in unstable intertrochanteric fracture can occur in different modes like screw cutout, fatigue failure of lag screw, implant disassembly and rarely pullout or breakage of side plate. Surgical fixation of intertrochanteric femur fracture remain the standard of care, however, the best method of fixation is debatable. Fracture fixation with a compression hip screw and side plate has been gold standard but certain new implant designs have challenged it. Recent design of compression hip screw also evolves continuously like plate construct that provides biaxial dynamic compression, lag screw with improved purchase are among the many recent innovations of compression hip screw design.
The fixed angled construct allow for dynamic fracture compression for most intertrochanteric fracture pattern. Acting in load sharing capacity hip screw allows compression through a fixed angled construct in intertrochanteric fracture perpendicular to the axis of femoral neck.
However, there has been a concerted effort to increase, rigidity and fixation of dynamic hip screw in osteoporotic bone. Current consensus is that locked plating is beneficial in situations that require support to end segment fracture that are prone to varus / valgus collapse and in diaphyseal and metadiaphyseal fracture in osteoporotic patients. It is thought that non locked plating acts as a single beam scenario in healthy bone. Osteoporotic bone condition where unsatisfactory compression causes premature loosening of screw that render them ineffective.
Advantage of Locked Plating
- Locking plates stability does not depend on the plate bone interface, rather stability is maintained at the angular-stable screw plate interface. As a result of this stable monoblock of the locking internal fixator, the pull out strength of locking head screw is substantially higher than that of conventional screws.
- The design of locked plate construct permits reduced need for bone friction which minimizes biological insult.
In spite all dynamic hip screw remains the gold standard standing the test of time. Osteoporosis which is seen, in more than half of the patients with trochanteric fracture is associated with higher incidence of implant failure due to poor purchase it provides.
Based on these advantages dynamic hip screw was introduced with locking side plate concept. These new implant designs have increased the pull out strength of side plate in osteoporotic bone and unstable fracture configurations particularly. So this study is intended to study the advantage of applying locking side plate principle to the dynamic hip screw in the treatment of unstable intertrochanteric fractures (as classified by Boyd and Griffin).
AIMS AND OBEJECTIVES
- To evaluate the outcome of locking dynamic hip screw in comparison to standard dynamic hip screw in terms of fracture union, implant failure, range of movement of hip joint in unstable intertrochanteric fractures in elderly patients (age > 65 years).
- To assess the hip function using modified Harris hip score.
MATERIAL AND METHODS
The prospective comparative randomized study comprises of unstable intertrochanteric fracture of
femur treated with dynamic hip screw and locking dynamic hip screw. The cases were selected randomly for fixation with DHS and Locking DHS. The series consist of 50 cases divided in 2 groups. The group 1 consist of 25 cases treated by DHS and group 2 consist of another 25 cases treated by Locking DHS. The cases were followed up for minimum of 6 month duration. In group 1 22 cases were available for follow 1case died while 2 lost in follow up while in group 2, 21 cases turned up for follow up 2 case died and another 2 lost in follow up. The study conducted in Department of Orthopaedics, Dhanwantri Hospital and Research Center, Jaipur during the period July, 2011 to September, 2012.
Inclusion Criteria
- Patients giving informed consent to take part in the study.
- Unstable intertrochanteric fracture
- Age > 65 years.
- Radiological evidence of osteoporosis
Criteria for evaluation of results
The end results assessment of patients has been done by point system of rating including aspect of patient’s daily routine. It is mainly based upon the rating scale for hip disabilities by Harris Hip score (1963).
Based on the above scores 4 grades are given:
≥ 80 : Excellent
79-70 : Good
69-60 : Fair
< 60 : Poor
Radiological Evaluation
Radiologically anteroposterior and lateral x-rays of hip joint with thigh were taken and evaluated for
- Progress of union
- Non-union
Varus / valgus deformity
OBSERVATION AND RESULTS

- The mean value ± standard deviation of Singh Index in group 1st was 3.64 ± 0.68.
- The mean value ± standard deviation of Singh Index in group 2nd was 3.56 ± 0.57.
Mean value of Singh’s Index in both groups was comparable.
 There was no pull out of side plate in LDHS group while there was pull out of side plate in one case in DHS group which has the Singh’s index 3.
There was no pull out of side plate in LDHS group while there was pull out of side plate in one case in DHS group which has the Singh’s index 3.
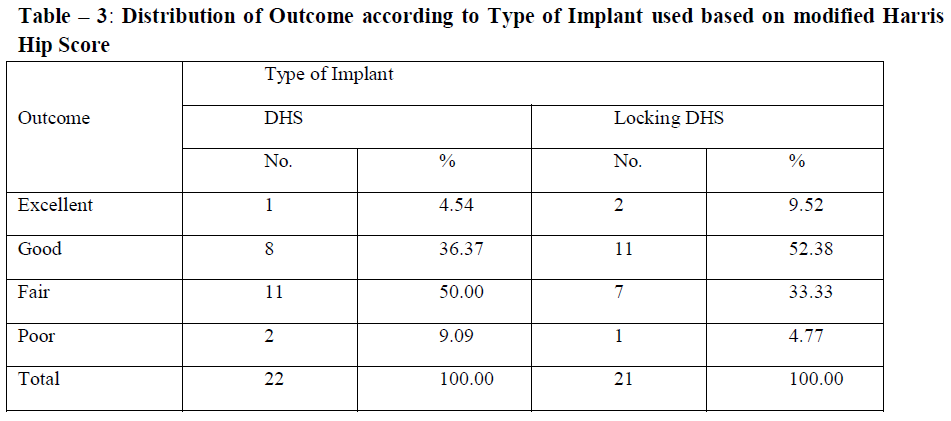
Excellent to good results were seen in 61.91% cases (13 out of 21 cases ) in LDHS group as compare to 40.91% cases ( 9 out of 22 cases) in DHS group. There was one case of poor result in LDHS as compare of 2 cases in DHS group.
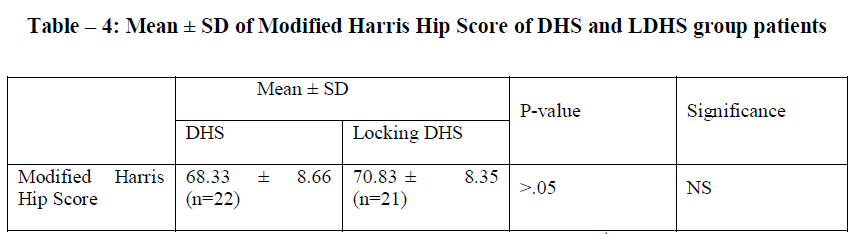
Mean ± standard deviation of modified Harris Hip Score in group 1st patients was 68.33 ± 8.66, as compare to 70.83± 8.35 in 2nd group patients. Although patient of group 2nd had more improved functional outcome as compare to group 1st patient but it was not statistical significant.
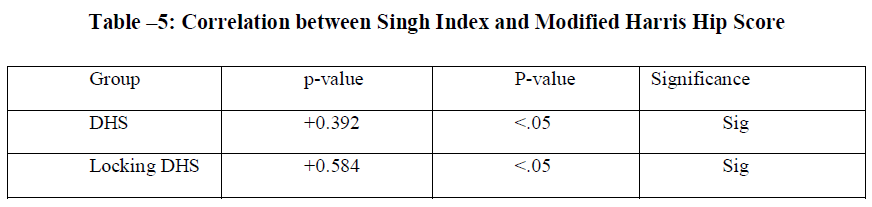
There was significant correlation between Singh Index and Modified Harris Hip Score in both groups. Functional outcome of intertrochanteric fractures in both groups either fixed with dynamic hip screw or locking dynamic hip screw both decreased as amount of bone osteoporosis increased as determined by Singh Index.
DISCUSSION
Intertrochanteric fractures are most commonly encountered fracture in geriatric age group. The most common underlying pathology is senile/postmenopausal osteoporosis.
This series includes randomly selected prospective study 50 cases of intertrochanteric fracture in osteoporotic patients. In our study 25 patients were treated by D.H.S (group 1st) and another 25 patients were treated by Locking D.H.S (group 2nd). Four cases out of fifty lost in follow up and three cases died during follow up, hence final assessment was done in 43 cases. All patients were admitted in the Department of Orthopaedics of Dhanwantri Hospital and Research Centre, Jaipur.
Since our study consisted of fixation of unstable intertrochanteric fractures in osteoporotic patients minimum age of the patient was 65 years and maximum age was 96 years. Mean age for group 1st was 72.84 years and in group 2nd it was 74.12 years. 64% of the patient in group 1st and 60% of patient in group 2nd were between the age group of 65-74 years. Only one patient in each group was above the age of 85 year.
Available literature suggests that osteoporosis of bone increases with age. In our study mean of Singh Index (1970) was 3.64 ± 0.68 group 1st and was 3.56 ± 0.57 in group 2nd.C.kayali et al (2006)(11) and Knobe et al (2008) in their studies treated by D.H.S had mean Singh index 2.5 and 2.9 respectively. In our study 48% patients in group 1st and 40% patients in group 2nd was in definite osteoporosis stage (Singh Index ≤ 3) which was similar to the series of K Akan et al (2011) and Yih-Shiunn Lee et al (2007) who mentioned the osteoporosis in 42.5% and 41.7% patients.
Coxa vara deformity is most common deformity in intertrochanteric fractures with reported incidence varying from 1.61% by Malcom L. Ecker et al (1975) to 9.02% by Laros and Moore (1974). Valgus deformity has also been reported at 10.24% by Laros and Moore (1974). K.S. Leung et al (1992) in his comparative study for intertrochanteric fracture fixation by D.H.S and Gamma nail in elderly patients found 2.15% Coxa Vara deformity in each group. Coxa Vara further exaggerates the limp by causing shortening and by reducing the efficiency of abductor lever arm.
In contrast to above studies we have mean higher rate of varus deformity. In the present series varus deformity was present in 22.73 cases in D.H.S group and 19.05% in L.D.H.S group. We have considered varus deformity if the neck shaft angle is less than 5º as compare to opposite side. Although higher numbers of patients were having varus deformity but the mean value of in group 1st patients was 0.89 ± 2.62º while mean value in group 2nd patients was 0.91 ± 2.67º. This is probably because of delayed weight bearing in our series.
In our study there was no case of nonunion in group 2nd treated by L.D.H.S but in group 1st treated by D.H.S there were 2 case of nonunion, out of which screw cut through occurred in one case (case no. 4) and pull of side plate in another case (case no. 5). In both these cases Singh index was 3
Simpson A.H., Varty K et al (1989) showed that side pull plate out was seen 4% cases in intertrochanteric fractures operated with dynamic hip screw. Based on their Biochemical study Dylan P.A. Jevell et al (2008) concluded that locking plate increases the pull-out strength of dynamic hip screw in osteoporotic bone. CAI Bing et al (2011) also had no side plate pull out in cases treated by L.D.H.S.
In our study side plate pull out was seen in 4.54% cases in group 1st and no side plate pull out was seen in group 2nd patients. This is explained due to better axial and torsional strength of locking DHS in patient age >65 years with osteoporotic bone.
C. Kayali et al (2006) in his study evaluated the result of patients treated by D.H.S through Modified Hariss Hip Score. He had 68.4% excellent to good results while 23.7%were fair and 7.9% had poor results. Similarly CAI Bing et al (2011) had better results in intertrochanteric
fractures treated by L.D.H.S . He had 89.5% excellent to good, 10.5% fair and no poor results in group treated by D.H.S. In our study 40.9% patients had excellent to good results in D.H.S and 61.9% in L.D.H.S group. 9.09% (2 cases) in D.H.S and 4.77% (1 case) in L.D.H.S group had poor results. High percentage of patients had fair results. The overall clinical results as evaluated by Modified Harris Hip Score were excellent to good in 51.16% cases, fair in 41.86% and poor 6.9% cases.
There were excellent to good results in 22 cases in our series out of which 19 cases had Singh index 4 or more while 3 cases had Singh index ≤3, two cases in D.H.S and one case in L.D.H.S group. There were 18 cases of fair results out of which 10 cases had Singh index ≤ 3. All 3 cases of poor results had Singh index 3. Thus our study shows significant correlation between Singh index and functional outcome. The functional outcome in both the group decreased as osteoporosis increased. K Akan et al (2011) had similar observations; in their study of intertrochanteric fractures treated by Gamma nail he had mean Harris Hip score 70 in patients of Singh Index grade I-II while mean Harris Hip score of 78.5 in patient had Singh Index III-IV. He observed that this difference to be statistically significant. Kim WY et al (2001) also had 39% implant failure in patients with osteoporotic intertrochanteric fracture treated by D.H.S had Singh Index I-II.
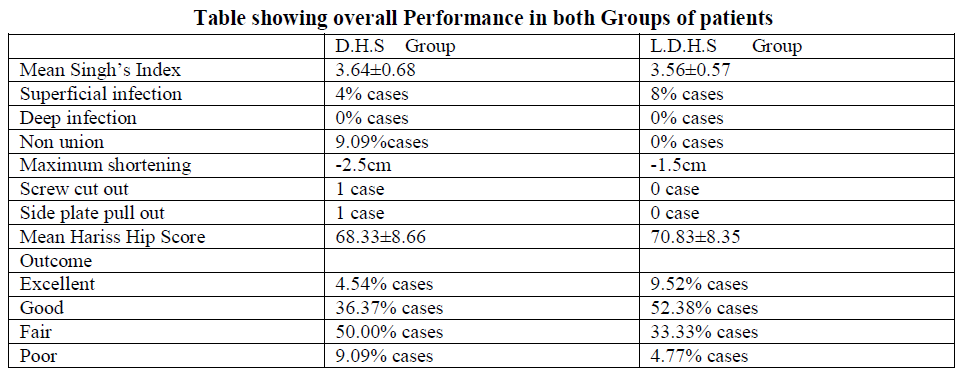 The above table showed the comparative outcome of intertrochanteric fracture treated by D.H.S and Locking D.H.S. Our study shows that patients had slightly better outcome with Locking D.H.S as compare to D.H.S. There was no non union and implant failure in patients treated by Locking D.H.S. The average Modified Harris Hip Score in patient treated by D.H.S was 68.33±8.66 as compare to Locking D.H.S 70.83±8.35. The osteoporosis had significant correlation with the functional outcome.
The above table showed the comparative outcome of intertrochanteric fracture treated by D.H.S and Locking D.H.S. Our study shows that patients had slightly better outcome with Locking D.H.S as compare to D.H.S. There was no non union and implant failure in patients treated by Locking D.H.S. The average Modified Harris Hip Score in patient treated by D.H.S was 68.33±8.66 as compare to Locking D.H.S 70.83±8.35. The osteoporosis had significant correlation with the functional outcome.
SUMMARY AND CONCLUSIONS
The series consisted of 50 patients treated by D.H.S (group 1st) and L.D.H.S. each group consisted of 25 cases.
- Most common mode of trauma in both groups of patients was slip (60%).
- Mean of Singh Index in group 1st cases was 3.64 ± 0.68 while mean of Singh Index in group 2nd was 3.56 ± 0.57.
- There were 5 cases (22.73%) of varus deformity in group 1st patients and 4 cases (19.05%) of varus deformity in group 2nd patients, although there were no significant varus deformity > 10º in both groups.
- Two case of nonunion was seen in group 1st patients.
- In DHS group there was one case each of side plate pull out and screw cut out. No implant failure was seen in locking DHS.
- This study showed that functional outcome deteriorated when patients was more osteoporotic.
- Final outcome assessed using Modified Harris Hip Score. In group 1st there were 4.54% excellent, 86.37% good to fair and 9.09 poor results, whereas in group 2nd cases 9.52% excellent, 85.71% good to fair and 4.77 was poor.
- Mean of Modified Harris Hip Score in group 1st was 68.33 ± 8.66 while 70.83 ± 8.35 in group 2nd cases.
In conclusion in patient age >65 years functional outcome after fixation of unstable intertrochanteric fractures with locking dynamic hip screw was slightly better than dynamic hip screw but it is not statistically significant.
In no cases of unstable intertrochanteric fractures fixed with locking dynamic hip screw, side plate pull out was seen. Its advantages over dynamic hip screw in osteoporotic bone (as proven by biomechanical studies).
References:
- Apel D.M. et al: Axial loading of unstable studies of unstable interochantric fractures of the femur:Clin Ortop No. 246,Dec,1989: 156-163.
- Audige L, Henson B, Swientkowski MF: Implant related complications in the treatment of unstable intertrochanteric fractures: meta-analysis of dynamic hip screw plate v/s dynamic screw – intramedullary nail devices. Int. Orthop. 2004, Feb; 28(1): 61 author reply 62-63.
- Baumgaertner MR,Curtin SL. Lindskog DM, et al. : The value of the tip-apex distance in predicting failure of fixation of pertrochanteric fractures of the hip. J. Bone joint Surg Am 1995:77:1058-1064.
- CAI Bing et al: treatment of femoral intertrochanteric fractures in the elderly with locking plate-dynamic hip screw and proximal femoral nail antirotation; journal of clinical orthopaedics;2011-12
- Cummings SR, Nevitt MC, Browner WS et al: Risk factors for hip fracture in white women: study of osteoporotic fractures Research group: New Eng. Jr of Med. 1995;332:767-73.
- Dylan, P.A. Jewell, Sabina Gheduzzi et al.: Locking plates increases the strength of dynamic hip screw, Injury, Int. J. Care Injured; 39:209-212, 2008.
- Gundle R, Gordan MF, and Simpson AH: How to minimize failures of fixation of unstable interochantric fractures. Injury 1995; Nov,:26(9): 611-614.
- Kim WY, Han CH, Park JI, Kim JY: Failure of intertrochanteric fractures fixation with a DHS in relation to preoperative fracture stability and osteoporosis: International Orthopaedics, 2001; 25(6): 360-362.
- Pervez H: Prediction of fixation failure after sliding hip screw fixation: Injury (Eng.) Oct. 2004; 35(10) pg. 994-8.
- Soloman, Warwik, Nayagam : Apley’s system of orthopadics and fractures 8th edn, 2001.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





