IJCRR - 5(24), December, 2013
Pages: 23-26
Date of Publication: 31-Dec-2013
Print Article
Download XML Download PDF
SYNOSTOSED COSTOCHONDRAL AND CHONDROSTERNAL JOINTS- A REVIEW
Author: Sayee Rajangam, Flossie Jayakaran, Sivacharan P. V.
Category: Healthcare
Abstract:Ossified costochondral and chondrosternal joints are often seen in radiological pictures and may be associated with some syndromes. Five such bony specimens available in our lab was studied and literature reviewed to see its prevalence, the process of ossification and if possible to evaluate the consequences of such a rigid thoracic inlet. A quick review showed that there is more to ossification than that given in standard textbooks and that it may have a role to play in sex dimorphism and age determination. This subject may definitely be of academic interest for research by postgraduate students in Anatomy.
Keywords: Ossified costochondral and chondrosternal joints, thoracic inlet
Full Text:
INTRODUCTION
The 1st rib’s costochondral and chondrosternal joints and the processes of ossification of the same are generally well known. Costochondral junctions are those between the anterior ends of the ribs and their costal cartilages which, with their rounded ends fit reciprocally into the depressions in the ribs. They are held in position by the continuity of the periosteum of the ribs and the perichondrium of the cartilages. These junctions are immobile and very strong. It may be noted that the adjacent bone may fracture but the bone and cartilage interface will not separate. Primary cartilaginous joints occur where bone and cartilage meet. Non-articular hyaline cartilage has the capacity to ossify with age and then a synchondrosis tends to become a synostosis upon the completion of growth. Chondrosternal articulations are found between the costal cartilages of the first 7 ribs and the articular facets on the lateral borders of the sternum. Among them, the 1ststernochondral joint between the manubrium and the first costal cartilage is an unusual form of synarthrosis and is often also called as synchondrosis. Slight gliding movements, sufficient for ventilation, may occur at this sternocostal joint. The manubrium is ossified from one to 3 centers appearing in the 5th month of fetal life and by the age of 25 years the centers in the sternum are united. The 1st rib has a primary center for the shaft that appears around the 2nd month of intrauterine life. Secondary centers for the head of the rib and tubercle appear around puberty. Fusion is completed by 20 years. The costal cartilages are the persistent un-ossified anterior parts of the cartilaginous elements from the transverse processes of the thoracic vertebrae in which the ribs develop. The 1st costal cartilage is continuous with the 1st rib and the manubrium, to form a primary cartilaginous joint that is usually replaced by bone after 25 years. (Sinnatamby 2006, Datta 2008, Standring 2008, Singh 2011) The present article is a short note and a review on the synostosed first costochondral and chondrosternal joints of the 1st rib.
MATERIAL AND METHOD
Among the teaching materials for Osteology of the thorax at the Department of Anatomy, International Medical School, Bangalore, there were five 1st ribs with intact synostosed costochondral and chondromanubrial (sternal) joints. The Method used here is subjective description of the observed features.
RESULTS
The 1st rib’s synostosed costochondral and chondrosternal joints were noted in 5 specimens and they were bilateral. From the muscular markings and the thickness of the specimens, they were subjectively sexed as male bones. The total number of manubria and 1st ribs available in the Department were 25 and 30 respectively. Hence, in the present study, the occurrence of the synostosed first ribs with their cartilages was 16.6% (5/30) and those with the manubria 20% (5/25).
Figure 1 shows the 5 specimens with complete and or incomplete forms of the synostosed costochondral and chondrosternal joints of the 1strib. Figure 1a is a complete sternum with remnants of the synostosed 1st rib on each side of the manubrium; Figure 1b shows manubrium with synostosed 1st rib, which is broken on the left side and as a stump on the right side; Figure 1c shows synostosed 1st rib, which is complete on the left side and stumped on the right side; Figures 1d and 1e are the two 1st ribs with synostosis in their anterior ends. Figure 1e had an additional feature of the presence of an oblique foramen passing medially from the superior to the inferior surface of the rib, near its inner border, between the scalene tubercle and the synostosis with the costal cartilage.
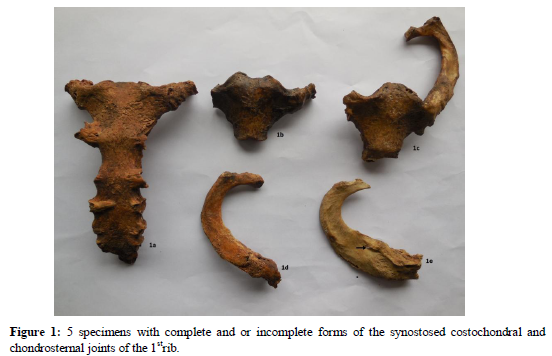
1:1a: Sternum with bilateral synostosis of the 1st rib. The right side shows a short segment of the 1st rib and on the left side is the broken 1st rib.
1:1b: Manubrium with synostosis. On the right side, a very small stump representing the 1st rib and on the left a short segment of the 1st rib is seen.
1:1c: Manubrium with bilateral synostosis. The right side shows a stump of the 1st rib and on the left side is the complete 1st rib.
1:1d: Complete right 1st rib showing synostosis with a small segment of the manubrium.
1:1e: Complete right 1st rib showing synostosis with a small segment of the manubrium. In addition, note the presence of an oblique foramen (indicated by an arrow) passing medially from the superior to the inferior surface located close to the inner border of the rib and the scalene tubercle.
DISCUSSION
A review of literature indicated the clinical importance of osteogenesis in the 1st rib in Radiology.
In 1989, a case of Teitze’s syndrome was reported in a female. Her CT scan showed the sclerosis of the manubrium, partial calcification of the costal cartilage and soft tissue swelling. A biopsy of the right 1st cartilage showed chronic inflammation with fibrosis and ossification. (Honda et al 1989)
In a radiological study by normal and polarized light microscopy on mineralization and osteogenesis of the 1st rib cartilage, the following were the findings in the words of the authors: (Kampen et al 1995)
i) Onset of mineralization occurred at the end of puberty and was located directly beneath the perichondrium.
ii) Bone was formed in a typical spur like manner medially from the upper edge of manubrium and laterally from the caudal rim of the bony part of 1st rib
iii) In the middle of the 2nd decade, large cartilage canals with several blood vessels and loose perivascular connective tissue were seen in the central areas of the 1st costal cartilage and these parts became the last to be mineralized and ossified in old age
iv) The type of osteogenesis can’t be classified according to the common patterns of the ossification. In spite of the subperichondreal localization, it can’t be intramembranous, because the new bone was separated from the perichondrium by a layer of mineralized cartilage and it can’t be called endochondral (comparable with the epiphyseal plate osteogenesis) because hypertrophied chondrocytes were absent. Moreover, immune reactivity for the collagen type ‘X’ was missing and areas where bone was formed, it was laid directly on hyaline cartilage
v) Vascularization and onset of osteogenesis could be separated in time and localization
vi) Mineralization and osteogenesis in the 1st costal cartilage being physiological age-related changes; hence, can’t be regarded as degenerative processes.
The authors concluded that the ossification could neither be directly correlated with the invasion of the blood vessels nor classified under the classical concepts of intramembranous or endochondral osteogenesis. However, the time of commencement of ossification was in accordance with that given in standard textbooks of Anatomy.
In an another study from radiographs, on the factors affecting the rate and pattern of the first costal cartilage’s ossification, the extent of the costochondral ossification of the 1st rib was determined in 13 healthy male soldiers out of 78 who were subjected to periodic follow up. (Barchilon et al 1996) The study has provided information on the process of ossification:
i) ossification of the 1stcostal cartilage may start early in adult life and progress at individual rates
ii) the process of ossification proceeds from the costal to the sternal end of the cartilage
iii) morphological age related changes range from the formation of small osseous islands in the cartilage to complete ossification between 1st rib and sternum.
The study concluded that the degree of ossification of the 1st costal cartilage as an indicator of age does not provide the precision necessary for forensic or anthropological studies.
Age and sexually dimorphic changes in costal cartilages, that appear at the microscopic level throughout life, especially during the ossification process, was also reported. (Rejtarova et al 2009).The particular research work was built on their previous study, which confirmed the presence of the two sexually dimorphic ossification patterns. The study was carried out on autopsies of 17 corpses, whose age varied greatly from newborn to 91 years. The method consisted of getting sections of costal cartilages, processed and stained. Alkaline phosphatase activity was detected with histochemistry and collagen fiber types ‘II’ and ‘X’ detected with immunohistochemistry by monoclonal antibodies. Their observations were:
i) ossification of costal cartilages could take place in the form of 2 independent processes such as localization and time.
ii) endochondral ossification in the region of the costochondral zone appears in the 1st decade, which correspond to ossifications detected by X-ray in the 2nd decade.
iii) location of sex-specific ossification is determined by the penetration of cartilage canals into the metaphyseal part of the rib.
iv) endochondral and intramembranous ossification in reserve zone appears after the 3rd decade.
v) these types of ossifications corresponded to central globular ossifications detected by X-rays and are not sexually dimorphic.
The study was concluded that it could serve for an accurate estimation of age.
Among the observations in the present study, the foramen in the rib (Figure 1e) could have been formed by the passage of a vein draining into the right subclavian vein.
CONCLUSION
The present study has reported the normal occurrence of the synostosed 1stcostochondral and chondrosternal joints. It has also reported a review from reports on their ossification processes and their importance in sex dimorphism and in age determination. The article could be considered as an academic source for postgraduate students in Anatomy for presentations in scientific programs (seminars, conferences) or dissertation topics or for research projects.
References:
- Barchilon V, Hershkovitz I, Rothschild BM, Wish-Baratz S, Latimer B, Jellema LM, Hallel T, Arensburg B. 1996. Factors affecting the rate and patterns of the first costal cartilage ossification.Am J Forensic Med Pathol. 17(3): 239-247.
- Datta AK 2008. Essentials of Human Anatomy (Thorax, Abdomen and Pelvis) Part 1.8th ed. Current Books International, Calcutta, India.
- Kampen WU, Classen H, Kirsch T 1995. Mineralization and osteogenesis in the human 1st rib cartilage. Ann Anat 177(2): 171-7.
- RejtarovaO, Hejna P, Soukup T, Kuchar M 2009. Age and sexually dimorphic changes in costal cartilages. A preliminary microscopic study . Forensic Sci Int. 193(1-3): 72-8.
- Singh IB 2011. Textbook of Anatomy.Volume 2, Thorax, Abdomen and Pelvis.5th edition.Jaypee Brothers Medical Publishers (P) Ltd, Delhi, India.
- Sinnatamby CS 2006. Last’s Anatomy: Regional and Applied. 11th edition. Churchill Livingstone / Elsevier, Edinburgh.
- Snell RS 2008. Clinical Anatomy by Regions. 8thed, Wolters Kluwer/ Lippincott Williams and Wilkins. Philadelphia, USA.
- Standring S 2008. Grey’s Anatomy. The Anatomical Basis of Clinical Practice.40th edition. Churchill Livingstone Elsevier, UK.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





