IJCRR - 5(24), December, 2013
Pages: 10-15
Date of Publication: 31-Dec-2013
Print Article
Download XML Download PDF
PREVALENCE AND EXISTING QUITTING PATTERN OF CHEWING TOBACCO AMONG URBAN POPULATION
Author: Syed Arif Pasha, Muneeb Jehan, Abdullah Rehman, Umrana Mirza
Category: Healthcare
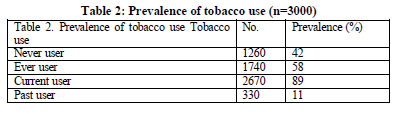
Abstract:Background: Awareness towards tobacco hazards has increased recently but its role alone towards cessation is still under debate. For effective formulation of quitting strategies, knowledge regarding quitting behavior is necessary to study and hence a cross-sectional study was carried out in Hyderabad city. Objectives: 1.To study prevalence of different forms of chewing tobacco and its quitting patterns in urban area. 2. To study quitting patterns in relation to various personal and family background factors. Materials and Methods: A cross sectional research involves 3000 individuals from randomly selected 30 clusters by two stage cluster sampling method for this research during June \?December 2009 from urban area of Hyderabad (India). Pretested, designed and self explained questionnaire was used for interview purpose after taking verbal, written and informed consent with approval from ethical committee. Statistical analysis was done using SPSS software. Information was collected on chewing forms, quitting pattern, quitting reasons and health hazards, age of tobacco initiation, duration of tobacco chewing, daily frequency, family exposure of tobacco and knowledge regarding health hazards of tobacco. Results: About 58% of study population was ever-tobacco-chewers; 89 % of them were current-chewers and 11 % were quitters. Approximately 18 % of current-consumers were willing to quit. Mawa-masala (73 %) and Gutka (62 %) were preferred forms of chewing tobacco and 60 % of the current-chewers chewed tobacco six to eight times a day. About 51 % smokers and 71 % chewers showing willingness to quit had not consumed tobacco for more than five years, 69 % of current-chewers had a family member consuming tobacco. With initiation of health problems, 62 % subjects quit while 38 % of them already knew about health hazards but not willing to quit. Conclusions: Every 7 out of 10 residents were found to be exposed to chewing tobacco. With Mawa-masala and Gutka as a primary source of consumption, early usage in late adolescence, continuous consumption for long time and family as well as friend circle exposure seem to be inhibiting quitting. Awareness of tobacco health hazards only does not produce successful quitting results.
Keywords: tobacco, chewing, health hazard, quitting
Full Text:
INTRODUCTION
Today it is known that tobacco use continues to be the leading global cause of preventable death. It kills nearly 6 million people and causes hundreds of billions of dollars of economic damage worldwide each year. Most of these deaths occur in Low and Middle-income countries, and this disparity is expected to widen further over the next several decades. If current trends continue, by 2030 tobacco will kill more than 8 million people worldwide each year, with 80% of these premature deaths among people living in Low and Middle- income countries. Over the course of the 21st century, tobacco use could kill a billion people or more unless urgent action is taken1.
Tobacco consumption is a global public health problem. Approximately one person dies every six seconds due to tobacco and this accounts for one in 10 adult deaths. Up to half of current users will eventually die of a tobacco-related disease. It kills nearly six million people a year of whom more than 5 million are users and ex users and more than 600 000 are non-smokers exposed to second-hand smoke. The burden of tobacco-related illness and death is heaviest in low- and middle-income countries. India has the second largest number of smokers in the world, after China2. According to GATS- India (2009-10), the prevalence of overall tobacco use among males is 48% and that among females is 20%3-5.
According to NFHS-III, in India, 55.8% male, 10.8% female in the age group of 12 to-60 years have been found to be consuming tobacco. Among males, 32.7% smokers while 36.5% tobacco chewers are reported, while among females; it is reported to be 1.4 and 8.4%, respectively6.
Awareness towards hazardous health effects of tobacco has increased with time but its role alone towards attainment of tobacco cessation is questionable. For effective formulation of quitting strategies, knowledge regarding quitting behavior is necessary to study and hence a cross-sectional study was carried out in Hyderabad city to find out the prevalence of chewing tobacco along with prevalence of quitters, their reasons for quitting, quitting behavior in existing consumers and associated factors.
MATERIALS AND METHODS
A cross-sectional study, based on the results of prior pilot study on prevalence of tobacco use was conducted in Hyderabad urban city. Almost 3000 individuals were selected from randomly selected 30-clusters from different political wards of Hyderabad city. The study was carried out between June-December 2009. Pre-designed and pre-tested questionnaire was used as a data tool after taking verbal and informed consent from participants. Tobacco chewing, different form, quitting pattern, age of tobacco initiation, its duration and frequency as well as knowledge regarding its health hazards, were used as study variables. Current-Tobacco-Chewers were those who had chewed tobacco regularly and chewed at least once on an average each day, during the previous 30 days at the time of study. Tobacco-Chewing-Quitters were those who chewed tobacco in the past but had quit and not chewing presently. The current-tobacco-chewers and past-tobacco-chewers together formed the term Ever-Tobacco-Chewers. Never-Tobacco-Chewers were the persons who never chewed tobacco in their lives.
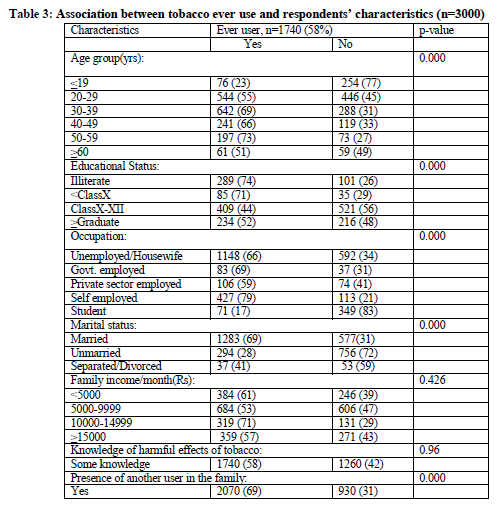
Descriptive statistics like mean, percentages and proportions were used. Chi- square test was used to see the association between tobacco use and selected variables like age, educational status, occupation, income, religion, knowledge of harmful effects of tobacco and presence of another tobacco user in the family. A p-value of <0.05 was taken as significant. Informed consent was taken from all the respondents and confidentiality was maintained. Approval for the study was granted by Institutional Review Board of Deccan College of Medical Science, Hyderabad, India.
RESULTS
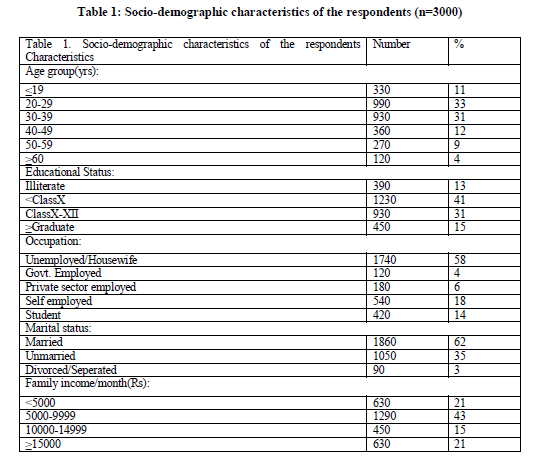
About 58 % of the total study population (1740) was found to be exposed to tobacco chewing either in past or present. A total of 366 out of total 3000 subjects (8.2%) were found to be tobacco smokers, while 1549 were reported to be tobacco chewers (52 %). Almost 17 % individuals were found to be consuming both smoking and smokeless forms of tobacco.
Mawa-masala was the preferred form of chewing found in 73% chewers followed by Gutka in 62%. Approximately 24.5% of current-consumers used tobacco in pan. Mean age of tobacco initiation was found to be 29 years in case of smokers, while it was 22 years in case of tobacco chewers. Among all study subjects, smoking prevalence was found to be 2 % in late adolescence, which rose sharply to 11% in the age group of 17 to 19 years and was found highest between 25 and 35 years (27%).
Tobacco chewing prevalence was almost 9 % in the age group of 13 to 17 years, which rose to 45 % among 17 to 19 years. It was found highest in 45-55 years of age group (75 %), followed by 56 % in 35 to 45 years of age. About 71 % of the current-consumers showed willingness to quit their habit.
Approximately 51 % of smokers and 71 % of current-chewers who showed willingness to quit had not consumed tobacco for more than five years. Among those who were not willing to quit tobacco, 82 % had chewed tobacco for more than five years.
About 69 % of current-tobacco-chewers had a family member consuming tobacco in any form, while 23 % of quitters had a history of any family member consuming tobacco in any form. Among the successful quitters, major reasons for quitting were found to be initiation of health problems (62 %), which included respiratory problems like coughing, breathlessness, short breathing and wheezing; reduced widening of mouth, weight loss and decreased working capacity cumulatively. Positive preaching from the local religious leaders towards quitting of tobacco played a role in 59 % of cases, while the reason was familial pressure either by spouse or by other family member(s) in 41% of the cases.
Approximately 20 % of quitters did not have a specific reason to quit, while among the current-tobacco-chewers, who were willing to quit, had social pressure (52 %) and religious vows (30 %) as the major reasons behind their willingness to quit.
Out of those who quit after initiation of health problems, 58 % already knew about health hazards of tobacco but did not bother until any health disturbance occurred to them.
DISCUSSION
The study results suggest a wide prevalence of tobacco chewing in the study population. Almost three-fourth of the residents were found to be exposed towards the habit of chewing tobacco. More than 89 % of the individuals were chewing tobacco at the time of study, which is not in association with Sen et al. (2000) who found the prevalence rate of tobacco chewing to be 36% in males and 19% in females7.
In the present study, the mean age of tobacco initiation was found to be 29 years in case of smokers, while it was 22 years in case of tobacco chewers. No national level data were available for the same but several studies by Kapoor et al. (1995), Babu et al. (1978), Sen et al. (2002), Singhi et al. (1987) etc. accord with the findings of early age of initiation of the habit8-11.
In current study, smoking prevalence was almost nil among 13 to 15 years but significantly highest between 25 to 35 years (27%). Similarly, tobacco chewing prevalence was almost 9% in the age group of 13-17 years, while almost 45 % among the age group of 17 to 19 years. It was highest in 45-55 years of age group (75%), followed by 56 % in 35 to 45 years of age. Sen U and Basu A (2000) reported that increased tobacco use was associated with older age groups7.
Mawa-masala and Gutka were the predominant forms of chewing tobacco, prevalence being much higher than what Gupta et al. (1996) found about betel quid with tobacco (27.1%)12. Harmful effects of tobacco were found to be widely known concurring the finding of Basu et al. (1992) that three out of four persons knew the problems of smoking13.
More than half of those who quit chewing tobacco after appearance of unfavorable health events knew earlier about the harmful effects of tobacco but did not pay much attention till it started showing.
CONCLUSION
People know much about the health hazards of tobacco and that merely is not sufficient to stop them from taking up or from continuing the habit as s and lake of knowledge as well as family and friend circle impact played a major role in its prevalence. Different strategies focusing on multiple background factors are needed for early age tobacco consumption intervention.
ACKNOWLEDGEMENT
Author acknowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript. The author is also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- WHO. WHO Report on The Global Tobacco Epidemic, 2011:Warning about the angers of tobacco. Italy: WHO; 2011. p 8. Available
from:http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf Accessed on Oct 15th, 2011.
- World Health Organization. Tobacco Fact Sheet No.339. 2012. Available from:
URL:http://www.who.int/mediacentre/factsheets/fs339/en/index.html . Accessed 18 June 2012.
- Global Adult Tobacco Survey (GATS): India. World Health Organisation; 2009-2010. Available from:
http://www.searo.who.int/LinkFiles/Regional_Tobacco_Surveillance_System_GATS_India.pdf . Accessed 6 July 2011.
- Reddy KS, Gupta PC, editors. Report on tobacco control in India. Ministry of Health and Family Welfare, Government of India, New Delhi, India 2004;57-61.
Rani M, Bonu S, Jha P, Nguyen SN, Jamjourm L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob
- Control, 12,2003,341. Available from: URL: http://www.tobaccocontrol.com/cgi/content/full/12/4/e4 . Accessed 28 June, 2011.
- National Family Health Survey 2005-06, Ministry of Health and Family Welfare, Govt. of India. Available from:
http://www.measuredhs.com/pubs/pdf/SR128/SR128.pdf. Accessed 1st Dec 2009.
- Sen U, Basu A. Factors influencing smoking behavior among adolescents. Asian
Pac J Cancer Prev. 2000;1:305–9.
- Kapoor SK, Anand K, Kumar G. Prevalence of tobacco use among school and college going adolescents of Haryana. Indian J Paediatrics. 1995;62:461–6.
- Babu DS, Chuttani CS, Murthy NS. Some epidemiological factors related to smoking among secondary school children of Delhi. Int J Epidemiol. 1978;7:183–4.
- Sen U. Tobacco Use in Kolkata. Lifeline. New Delhi, India: WHO SEARO; 2002. pp. 7–9. Vol 8.
- Singhi S, Brica JS, Mathur GM. Smoking behavior of rural school boys. Indian Paediatr. 1987;24:655–9.
- Gupta PC. Survey of sociodemographic characteristics of tobacco use among 99598 individuals in Bombay, India, using hand-held computers. Tob Control. 1996;5:114–20.
- Basu A, Ganguly SK, Datta S. Demographic survey of opinions towards smoking: A pilot study. J Indian Med Assoc. 1992;90:292–4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





