IJCRR - 6(1), January, 2014
Pages: 39-43
Print Article
Download XML Download PDF
FINE NEEDLE ASPIRATION (FNAC) AS A DIAGNOSTIC TOOL IN PAEDIATRIC LYMPHADENOPATHY.
Author: Heming Agrawal, R.N. Gonsai, Shilpa Singal, H.M. Goswami
Category: Healthcare
Abstract:Aim - This Study has been undertaken to evaluate the diagnostic role of Fine Needle Aspiration Cytology (FNAC) in paediatric lymphadenopathy. Materials and Method - 102 paediatric patients (upto 14 years of age) with Lymphadenopathy were subjected to FNAC over a period of 6 months (January 2013 to June 2013). FNAC was done as a routine procedure using 22 gauge needle with standard precautions. Smears obtained were stained with May-Grunwald-Giemsa (MGG), Papanicolaou (PAP) and Hematoxylinand Eosin (Hand E). Special stain used was Ziehl-Neelsen (ZN) for Acid Fast Bacilli (AFB). Result - In this study, out of 102 cases 56(54.9%) patients were males and 46(45.0%) patients were females. The male and female ratio was 1.22:1. Inflammatory lymphadenopathy comprised 97.05% of the total lesions of the lymph nodes. It included 66.66% cases of chronic non specific lymphedenitis, 27.45% cases of granulomatous lymphadenitis, 1.96% cases of acute suppurative lymphadenitis and 0.96% cases of Kikuchi's diseases. Malignant lesions were seen in 3(2.94%) patients. Conclusion - FNAC is a very simple and expeditious procedure which can be carried out with ease in children. The diagnostic accuracy of the cytosmears was 98.89% and the overall sensitivity and specificity were 91.3% and 99.1%, respectively so, FNAC is fairly accurate in the diagnosis of lymphadenopathy.
Keywords: Fine needle aspiration cytology, FNAC, paediatric, children, lymphadenopathy.
Full Text:
NTRODUCTION
Lymphadenopathy is one of the commonest clinical presentations in paediatric patients. It is necessary to arrive at a definitive diagnosis in order to administer proper treatment in a easy, fast way. It has several aetiologies ranging from an inflammatory process to a malignant condition, thus posing diagnostic dilemma to a paediatrician. Therefore, it is necessary to arrive at a definitive diagnosis in order to administer proper treatment. The objective of this study was to evaluate the diagnostic role of fine needle aspiration cytology in lymphadenopathy in the paediatric age group. It has been shown in several studies like ours, that FNA is fairly accurate in the diagnosis of lymphadenopathy.1,2 In the last few years, FNAC has emerged as a reliable diagnostic procedure in the paediatric age group, thus obviating the need for excision biopsy3,4 .
MATERIALS AND METHODS
The study was carried out in OPD and ward patients up to 14years of age, who had palpable lymph node. The duration of study was 6 months. Lymphadenopathy was considered to be significant if the cervical group was >1.0cm and the inguinal group was >1.5cm. Detailed clinical history and general, local and systemic examination, along with routine and special investigations was taken. 102 patients weresubjected to FNAC; Histopathological examination was performed in 40 patients. Both dry and wet fixed smears were prepared in all cases and were stained by Hand E, MGG and Papanicolaou stains. Ziehl-Neelsen’s stain was used wherever indicated.
RESULT
In this study, out of 102 cases, 56(54.9%) patients were males and 46(45.0%) patients were females. The male and female ratio was 1.22:1 Generalised lymphadenopathy was defined as the enlargement of more than two non-contiguous node regions.5 In the present study, localised lymphadenopathy was seen in 99 cases (90%) and the generalised category was seen in 11 cases (10 %.). The maximum number of cases had cervical lymphadenopathy (82%), followed by involvement of the axillary (11%) and the inguinal (7%) nodes. Out of the cervical group of nodes, the upper anterior and the upper posterior deep cervical nodes were involved in a majority of cases (60.0%). The size of the nodes was measured in all the cases. The largest node which was seen had a maximum diameter of 3.5 cm. The diagnosis of 102 cases of lymphadenopathy based on cytological examination alone is shown in [Table 1]. However, Cytohistological correlation could be done in 40 cases only, as shown in [Table 2]. The cytological criteria which were adopted for classification were as follows: Inflammatory lesions
Ninety nine nodes were diagnosed as inflammatory by FNAC. They were further grouped into sub-categories.
Chronic non specific lymphedenitis and reactive hyperplasia:
The cytosmears of these cases showed a mixed population of lymphoid cells. The cytological pattern of distribution of the cells depended on whether the follicular or intrafollicular tissue was aspirated. The active germinal centre had many centrocytes and centroblasts, and sparse mature lymphocytes, plasma cells and immunoblasts. (Figure1). Interfollicular tissues have predominantly mature lymphocytes, plasma cells and immunoblasts. They were probably from cases of lymphadenopathy following viral infection
Tubercular lymphedenitis
Out of the 102 cases, 28 cases were diagnosed as Tubercular lymphadenitis (Figure 2). Some cases presented with secondary infection and in them, a course of antibiotics was advised and repeat FNAC was done. In those cases in which only caseous material was seen, repeat FNAC was advised to search for a granuloma. Acid Fast Bacilli (AFB) and only 7% cases proved to be positive. Though granulomatous response is seen in a wide variety of infectious agents and non infectious processes (both benign and malignant), as tuberculosis is so common in our country, every clinically relevant case of granulomatous lymphadenitis should be considered as tuberculous lymphadenitis, unless proved otherwise6 . Out of 10 cases which were diagnosed by cytology, 09 were confirmed by histopathology. One case where the diagnosis of tuberculosis was made on the basis of epithelioid cells, turned out to be reactive hyperplasia by histology. We had correlated all our cases of granulomatous lymphadenitis with the clinical presentation, if done Montoux test, AFB and Culture.
Acute suppurative lymphadenitis
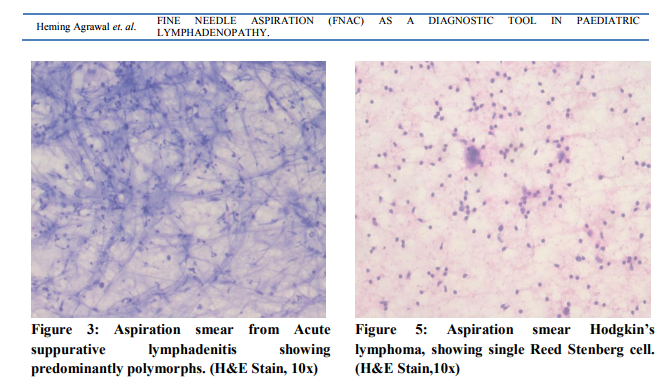
The cytosmears showed degenerated and viable inflammatory cells, predominantly polymorphs (Figure 3). Repeat aspiration was advised after a course of antibiotic therapy.
Malignant lesions Non-Hodgkin’s Lymphoma
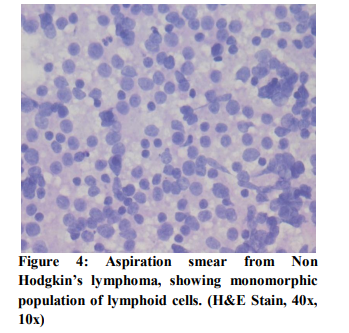
Monotonous population in the smear, was the most important basis for the diagnosis of non Hodgkin’s lymphoma in cytological smears. (Figure 4). In this study, one case was diagnosed correctly by FNAC. One case diagnosed by us as reactive hyperplasia turned out to be non-Hodgkin’s lymphoma. Conversely, one case which we diagnosed as non-Hodgkin’s lymphoma was reactive hyperplasia
Hodgkins lymphoma
The presence of Reed Sternberg cells was essential to diagnose Hodgkin’s lymphoma. Numerous atypical large mononuclear cells with prominent nucleoli were also seen. Besides these cells, variable numbers of plasma cells, lymphocytes, eosinophils and reactive cells were seen in the background (Figure 5). In the present study, one case was diagnosed as Hodgkin’s lymphoma by FNAC and was confirmed by histology.
DISCUSSION
This study was carried out primarily to evaluate the role of FNAC as a diagnostic tool, with it’s advantages and limitations, in paediatric lymphadenopathy. In the present study, cytological examination was done on 102 patients, but histopathological examination of the lymph nodes could be done only in 40 patients. Overall, inflammatory lymphadenopathy comprised 97.05% of the total lesions of the lymph nodes; it included 66.66% cases of reactive hyperplasia, 27.45% cases of tubercular lymphadenitis and 1.96% cases of acute suppurative lymphadenitis. Malignant lesions were seen in 2.94% of the patients. These findings are in agreement of those reported by Locham et al, who diagnosed reactive hyperplasia in 68% cases, tubercular lymphadenopathy in 29% cases and malignancy in 3% cases7 . Tripathi et al found reactive hyperplasia in 64% cases and tuberculosis and neoplasia in 4% of the patients.8 Sankaran et al also observed lymphoid hyperplasia as the most common condition in benign lesions, followed by tuberculosis.9 Jain et al reported 1.8% malignant cases in their study. 10 The overall sensitivity and specificity reported by Prasad et al were 89.2% and 100%, respectively, which matched with our findings.11
CONCLUSIONS
FNAC is a very simple and expeditious procedure which can be carried out with ease in children. The diagnostic accuracy of the cytosmears was 98.89%and the overall sensitivity and specificity were 91.3% and 99.1%, respectively so, FNAC is fairly accurate in the diagnosis of lymphadenopathy. It reduces the neccessity to perform excision biopsy in many cases, thus saving children from surgical complications. It is difficult to understand why such an effective, simple and safe diagnostic modality is so underutilised in the diagnostic workup of paediatric TB, it can be a good diagnostic tool for it in paediatric patients.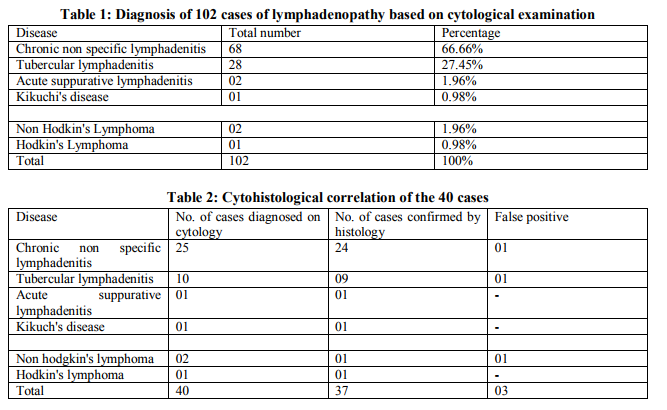

References:
REFERENCES
1. Byun JC, Choe BK, Hwang JB, Kim HS, Lee SS. Diagnostic effectiveness of fine needle aspiration cytology on pediatric cervical lymphadenopathy. Korean J Pediatr 2006;49:162-6.
2. Chu EW, Hoye RC. The clinician and the cytopathologist evaluate fine needle aspiration cytology. Acta cytological.,1973; 21:413-17.
3. Handa U, Mohan. H, Bal .A. Role of fine needle aspiration cytology in evaluation of paediatric lymphadenopathy. Cytopathology. 2003:14; 66 – 69.
4. Ajmal F, Imran A. Comparison of FNAC vs excision biopsy for suspected tuberculous cervical lymphadenopathy. Annals King Edward med coll 2003; 9:216-8.
5. Bedros AA, Mann JP. Lymphadenopathy in children. Adv Pediatr 1981;28:341– 76.
6. Bari A, Wadood A, Qasim K, Fine needle aspiration cytology; evaluation in thediagnosis of lymphadenopathy in children, Professional Med J 2007; 14: 237-240.
7. Locham KK al. Lymphadenopathy in children role of FNAC. Journal of Cytology. 2002; 19:183-86.
8. Tripathi S et al. Orissa Journal of Pathology and Microbiology. 2003; 7: 34-36.
9. Sankaran V, Prasad RR, Narasimhan R, Veliath AJ. Fine needle aspiration cytology in the diagnosis of superficial lymphadenopathy. An analysis of 2,418 cases. Diagn cytopathol. 1996; 15 : 382-16.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





