IJCRR - 6(2), January, 2014
Pages: 26-34
Print Article
Download XML Download PDF
AN EXTREMELY RARE REPORT OF TUBERCULOUS COLD ABSCESS OF THE RIGHT ANTERIOR CHEST WALL PRESENTING AS AN EXTREMELY HARD AND IMMOBILE LUMP MIMICKING CARCINOMA BREAST
Author: Govindarajalu Ganesan, Krishnapillai Ayyappan
Category: Healthcare
Abstract:Tuberculous cold abscess usually presents as soft swelling and occurs commonly in the neck, axilla and inguinal regions due to the presence of lymph nodes in these regions. But tuberculous cold abscess of the anterior chest wall is quite rare. Also tuberculous cold abscess of the anterior chest wall presenting as an extremely hard and immobile lump is extremely rare and is so far not reported in the literature and hence is reported here. Due to the extremely hard and immobile lump, the lesion was initially thought to be due to carcinoma breast. But after detailed investigations, the lump was finally diagnosed to be due to tuberculous cold abscess. The exact reasons for the extreme hardness and immobility of the lump are discussed here in detail. The role of ultrasonography in distinguishing between solid and fluid filled lesions of the anterior chest wall and in showing clearly the exact anatomical relation of the fluid filled lesion to the breast and ribs is discussed here. The importance of doing incisional biopsy before starting antituberculous drugs and its role in excluding malignancy is discussed here. The importance of doing prompt surgical drainage and complete evacuation of the cold abscess inorder to prevent the disastrous complication of rupture of the cold abscess into the underlying pleural cavity and lungs is also discussed here.
Keywords: Tuberculous cold abscess, anterior chest wall, extremely hard and immobile lump, ultrasonography, incisional biopsy, prompt surgical drainage.
Full Text:
INTRODUCTION
Tuberculous cold abscess of the chest wall is quite rare. Tuberculous cold abscess can occur in the anterior chest wall or lateral chest wall or in the posterior chest wall (1,11). Tuberculous cold abscess of the anterior chest wall is commonly reported to occur in association with tuberculosis of the underlying ribs (6,27) or tuberculosis of the underlying lungs (5,.6,7,10,11,21,29). But in the patient reported below the cold abscess of the anterior chest wall was neither associated with tuberculosis of the underlying ribs nor associated with tuberculosis of the underlying lungs. Tuberculous cold abscess of the anterior chest wall lying parasternally is reported to occur mainly due to tuberculous caseation of the internal mammary lymph nodes (3,8,10,18,21,22). Hence the most probable cause of the cold abscess which was lying parasternally in this patient was tuberculous caseation of the internal mammary lymph nodes. Tuberculous cold abscess of the anterior chest wall occurring without tuberculosis of the underlying ribs or lungs is very rare and is hence reported here.
Case report:
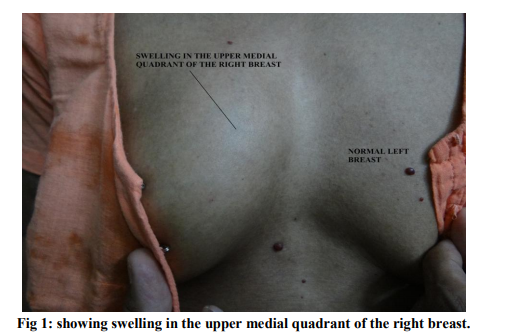
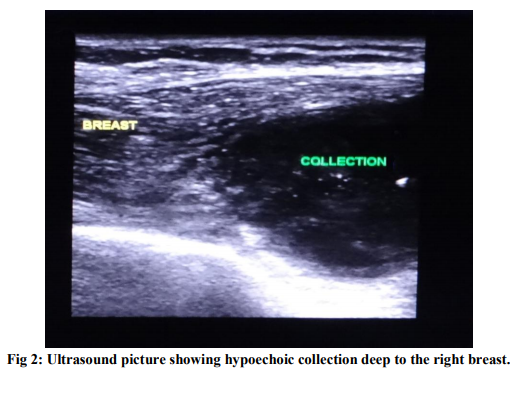
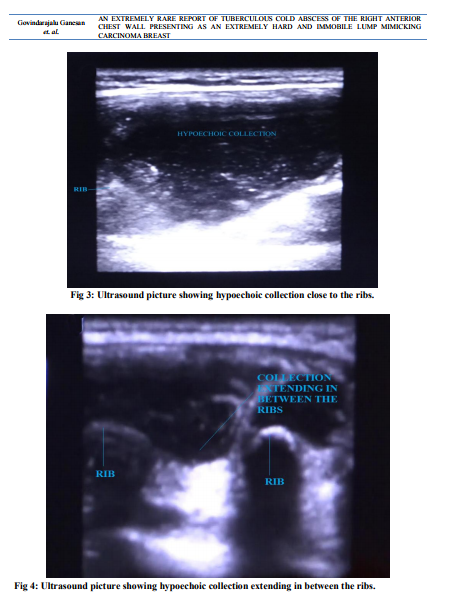
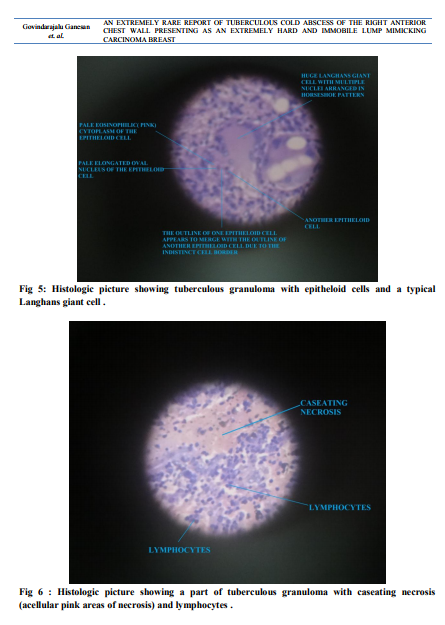
A 55 year old female patient presented with history of painless lump of the right breast, gradually increasing in size for two months. There was no history of fever, loss of appetite or loss of weight. She was non diabetic, human immunodeficiency virus (HIV) negative immunocompetent patient. Local examination revealed an extremely hard, immobile, nontender, smooth lump measuring about 6x3cms in the region of right upper medial quandrant of the right breast (fig 1). Due to the extremely hard and immobile lump, the lesion was initially thought to be due to carcinoma breast and the patient was immediately subjected to ultrasound examination of the right breast. But very interestingly ultrasound examination revealed normal right breast and an abundant amount of collection of dense fluid deep to the right breast (fig 2) extremely close to the ribs (fig 3 ). The collection was also seen to extend in between the ribs by ultrasound examination (fig 4) Mantoux test revealed 29x24mm induration at the end of 48hours. Hence the patient was strongly suspected to have tuberculous cold abscess. But X-ray chest was normal without erosion of the underlying ribs and also revealed normal lung fields. While doing fine needle aspiration cytology (FNAC), aspiration showed pus like material and microscopic examination revealed neutrophils, macrophages and degenerated cells in a necrotic background and the smear for acid fast bacilli was also negative. Despite very strong Mantoux test, since X-ray chest and Fine needle aspiration cytology were inconclusive of tuberculosis, it was decided to do incisional biopsy inorder to get accurate tissue diagnosis. Hence under short general anaesthesia, an incision was made deep into the lesion. About 250 ml of pus was found deep to the right breast and deep to the pectoralis major and minor muscles extremely close to the ribs. After complete evacuation of the pus, an incisional biopsy was done from the wall of the abscess. Histopathological examination revealed epitheloid cell granuloma with langhans giant cells, caseating necrosis and lymphocytes indicating tuberculosis (fig 5,6). Epitheloid cell is identified under light microscope by its lightly stained pale elongated or oval nucleus, lightly stained eosinophilic (pink) cytoplasm and indistinct cell border (fig 5). Due to the indistinct cell border, the outline of one epitheloid cell appears to merge with the outline of the adjacent epitheloid cell (fig 5) (29 to32). Langhans giant cells are huge cells with multiple nuclei arranged as horseshoe pattern in the periphery of the cell (fig 5) (29to32). Caseating necrosis is identified by acellular pink areas of necrosis under light microscope (fig 6) (29). Lymphocytes are cells almost completely filled with haemotoxylin stained blue coloured nucleus. Hence a final diagnosis of tuberculous cold abscess of the right anterior chest wall was made for the patient. The patient was immediately started on 6 months daily course of antituberculous drugs with daily dose of Isoniazid 300mg, Rifmpicin 450mg, Ethambutol 800mg and Pyrazinamide 1500mg for an intial period of two months followed by daily dose of Isoniazid 300mg and Rifmpicin 450mg for the next four months. After completion of three months of antituberculous treatment, the operative wound has healed completely, the patient has become completely asymptomatic and has recovered completely
DISCUSSION
Tuberculous cold abscess of the anterior chest wall usually presents as soft and mobile swelling (1,2,3,9,13,14,16,18,20,32) . But tuberculous cold abscess of the anterior chest wall presenting as an extremely hard and immobile swelling, as in this patient, is extremely rare. The cold abscess of this patient was lying between the strong pectoral muscles in front and the bony ribs behind and was extremely hard and immobile. The exact reasons for the extreme hardness and immobility of this cold abscess are discussed here in detail. Tuberculous cold abscess is a type of false cyst. A cyst is a swelling having fluid inside it. A cyst is of two types- true cyst and false cyst. A true cyst has fluid inside it and is lined by epithelium. A false cyst has fluid inside it but is not lined by epithelium. An abscess is a false cyst as it has pus inside it but is not lined by epithelium. Both pyogenic abscess and tuberculous cold abscess are examples of false cyst. Tuberculous cold abscess is a false cyst as it has caseating material or tuberculous pus inside it but is not lined by epithelium. A false cyst like tuberculous cold abscess has all the clinical features of a true cyst except for the fact that it is not lined by epithelium. A cyst is soft, firm or hard depending upon the tension of the fluid present inside the cyst. A cyst will be hard in consistency if the fluid inside the cyst is under tremendous tension. Being a false cyst, tuberculous cold abscess will also be hard in consistency if the tuberculous pus inside the cold abscess is under tremendous tension. The cold abscess of this patient was filled with abundant amount of tightly packed collection of dense caseating material or tuberculous pus. As the disease progresses, the extent of caseation increases and the tuberculous pus also increases in amount. But this increasing amount of tuberculous pus of this patient could not expand freely both anteriorely and posteriorely due to the highly unyielding extremely strong pectoralis major muscle present anteriorely and the strong bony ribs present posteriorely producing tremendous tension of the tuberculous pus inside the cold abscess. Since the tuberculous pus inside the cold abscess of this patient was under tremendous tension due to the highly unyielding strong pectoralis major muscle present anteriorely and the strong bony ribs present posteriorely, the cold abscess was extremely hard in consistency. Any deep swelling arising from bone or attached to bone is immobile. The cold abscess of this patient was lying extremely close to the ribs and was also seen to extend in between the ribs both by ultrasound examination and during the operation and hence it was immobile. Ultrasonography, with its advantages of being radiation-free, is an extremely useful diagnostic tool for evaluation of chest wall lesions (16) Ultrasonography is a cost-effective and an extremely useful modality to demonstrate rib destruction in a chest wall cold abscess. Ultrasonography shows abscesses as hypoechoic areas and bone fragments due to rib destruction appears as echogenic foci within these hypoechoic collections (15). But in this patient ultrasonography did not show any evidence of rib destruction. Thus ultrasonography shows chest wall cold abscess as hypoechoeic collection (28, 29). Hence ultrasonography in this patient also has shown an hypoechoeic collection deep to the right breast adjacent to the ribs (fig 2,3). Thus ultrasonography is extremely useful to distinguish between solid and fluid filled lesions of the anterior chest wall, shows the exact anatomical relation of the fluid filled lesion and its relation to the breast and ribs (fig 2,3) and can also show clearly the extension of the fluid filled lesion in between the ribs (fig 4). Incisional biopsy is generally avoided in tuberculous cold abscess of cervical, axillary and inguinal lymph nodes due to the fear of occurrence of non-healing sinus or ulcer (33). But in most cases of cold abscess of the anterior chest wall, fine needle aspiration cytology is inconclusive of tuberculosis (2,7,8,9,11,19,24,34). Hence incisional biopsy from the wall of the cold abscess is absolutely mandatory inorder to get accurate tissue diagnosis and to rule out any underlying malignancy(1,2,8,9,18, 20,23,24,29,32). Incisional biopsy is also absolutely necessary since rare organisms other than Mycobacterium tuberculosis like Burkholderia pseudomallei causing melioidosis and even Staphylococcus aureus were reported to cause cold abscess of the anterior chest wall (33,35) Biopsy and histopathological examination facilitates prompt diagnosis of chest wall cold abscess (20). Histologic proof by biopsy facilitates prompt treatment of chest wall cold abscess (20). Such prompt diagnosis and treatment is extremely important to prevent serious bone and joint destruction underlying the chest wall cold abscess (1,18). In this patient, within one week of her clinical presentation, X-ray chest, Mantoux test, ultrasonography and fine needle aspiration cytology was done immediately followed by incisional biopsy from the wall of the abscess after complete surgical evacuation of the abscess. Within few days after doing incisional biopsy, histopathological examination revealed tuberculous granuloma and the patient was immediately started on antituberculous drugs. Hence within two weeks of her clinical presentation, complete surgical drainage of the cold abscess was done, histological diagnosis of tuberculosis was made and antituberculous drugs was started for the patient. Because of such prompt diagnosis and treatment, serious complications like destruction of the adjacent ribs and rupture of the cold abscess into the underlying pleural cavity and lungs was avoided in this patient. Hence prompt histological diagnosis and prompt surgical and medical treatment of the cold abscess of the anterior chest wall is extremely important to avoid the above mentioned serious complications. Tuberculous cold abscess of cervical, axillary and inguinal lymph nodes are generally managed by antigravity or non-dependent wide bore needle aspration along with antituberculous drug treatment (33). But wide bore needle aspration is not adequate for the deep seated cold abscess of the anterior chest wall as it has high risk of incomplete evacuation of the cold abscess. But complete evacuation of the cold abscess of the anterior chest wall is extremely important as the cold abscess can easily rupture into the underlying pleural cavity or lungs with disastrous consequences if not completely evacuated. However complete evacuation of this cold abscess is possible only through open surgical drainage and not by wide bore needle aspration. Cold abscess of the anterior chest wall cannot rupture anteriorely due to the highly unyielding extremely strong pectoralis major muscle present anteriorely. Hence the only way for the cold abscess to rupture is through the space between the ribs into the underlying pleural cavity or lungs with disastrous consequences (24,27). Hence prompt open surgical drainage and complete evacuation of the cold abscess without any undue delay is extremely important inorder to avoid the disastrous consequences of rupture of the cold abscess into the underlying pleural cavity and lungs. The cold abscess of the anterior chest wall of this patient was not associated with tuberculosis of the underlying ribs or lungs. The cold abscess was located deep to the right upper medial quadrant of the right breast just by the side of sternum which is the exact location of the internal mammary lymph nodes. Tuberculous cold abscess of the anterior chest wall lying parasternally is reported to occur due to tuberculous caseation of the internal mammary lymph nodes (3,8,10,18,21,22). Since the underlying ribs and lungs were normal and due to its parasternal location the most probable cause of the cold abscess of this patient was tuberculous caseation of the internal mammary lymph nodes.
CONCLUSION
Six extremely important features of tuberculous cold abscess of the anterior chest wall of this patient are highlighted in this article 1. The cold abscess was extremely hard due to the tremendous tension of tuberculous pus inside the cold abscess due to the highly unyielding strong pectoral muscles in front of it and the bony ribs behind it. 2. The cold abscess was immobile since it was lying extremely close to the ribs and was also extending in between the ribs. 3. Ultrasonography is extremely useful to distinguish between solid and fluid filled lesions of the anterior chest wall and shows clearly the exact anatomical relation of the fluid filled lesion to the breast and ribs. 4. Incisional biopsy from the wall of the cold abscess is absolutely mandatory inorder to get accurate tissue diagnosis and to rule out any underlying malignancy. 5. Prompt open surgical drainage and complete evacuation of the cold abscess without any undue delay is extremely important inorder to avoid the disastrous consequences of rupture of the cold abscess into the underlying pleural cavity and lungs. 6. Since the underlying ribs and lungs were normal and due to its parasternal location the most probable cause of the cold abscess of this patient was tuberculous caseation of the internal mammary lymph nodes
ACKNOWLEDGEMENT
Both the authors gratefully acknowledge with utmost respect Professor Dr. N. Anantha Krishnan, the greatest guru for both of us, whose constant guidance, encouragement and advice has helped us to publish this manuscript. Both the authors also acknowledge with extreme thankfulness Professor Dr.Thirupurasundari, Head of the dept of gynaecology, Aarupadai Veedu Medical College And Hospital, Puducherry for doing thorough gynaecological examination of the patient and ruling out gynaecological pathology in the patient.
References:
REFERENCES
1. Papavramidis TS, Papadopoulos VN, Michalopoulos A, Paramythiotis D, Potsi S, Raptou G, Kalogera-Foutzila A, Harlaftis N. Anterior chest wall tuberculous abscess: a case report.J Med Case Rep. 2007 Nov 26;1:152.
2. Abid, H., Toujani, S., Ammar, J., Marghli, A., Slim, L., Hantous, S.Ayadi A, ... Hamzaoui, A. Chest swelling with adenopathy: Don’t forget tuberculosis. Respiratory Medicine CME, 2011;4(1): 47-49.
3. Prasoon D.Tuberculosis of the intercostal lymph nodes.Acta Cytol. 2003 JanFeb;47(1):51-5
4. Rivo V J, Fernández V A, Cañizares C M. (2004). Cold abscess of the chest wall 58 years after thoracoplasty Arch Bronconeumol. 2004 Nov; 40(11):540-1.
5. Zhang Y, Li H, Li T, Zhang WQ.A tuberculous abscess of the chest wall in a renal allograft recipient.J Thorac Dis. 2013 Aug;5(4):E133-6
6. Sakuraba M, Sagara Y, Komatsu H.Surgical treatment of tuberculous abscess in the chest wall.Ann Thorac Surg. 2005 Mar;79(3):964-7.
7. Kim YT, Han KN, Kang CH, Sung SW, Kim JH.Complete resection is mandatory for tubercular cold abscess of the chest wall.Ann Thorac Surg. 2008 Jan;85(1):273-7.
8. Kuzucu A, Soysal O, Günen H.The role of surgery in chest wall tuberculosis.Interact Cardiovasc Thorac Surg. 2004 Mar;3(1):99- 103.
9. Aghajanzadeh, M., Pourrasouli, Z., Aghajanzadeh, G., and Massahnia, S. Surgical Treatment of Chest Wall Tuberculosis. Tanaffos, 2010; 9(3): 28-32.
10. Morris BS, Maheshwari M, Chalwa A.Chest wall tuberculosis: a review of CT appearances.Br J Radiol. 2004 May;77(917):449-57.
11. Deng B, Tan QY, Wang RW, He Y, Jiang YG, Zhou JH, Liang YG.Surgical strategy for tubercular abscess in the chest wall: experience of 120 cases.Eur J Cardiothorac Surg. 2012 Jun;41(6):1349-52.
12. Ero?lu A, Kürkçüo?lu C, Karao?lano?lu N, Kaynar H.Breast mass caused by rib tuberculosis abscess.Eur J Cardiothorac Surg. 2002 Aug;22(2):324-6.
13. Bekci, T. T., Ya?ar, B. T. S., Kesli, R., Maden, E. Tuberculous Abscess of the Chest Wall. Eur J Gen Med, 2010; 7(3) : 326-329
14. Chang JH, Kim SK, Kim SK, Chung KY, Shin DH, Joo SH, Choe KO. Tuberculosis of the ribs: a recurrent attack of rib caries.Yonsei Med J. 1992 Dec;33(4):374-8.
15. Grover SB, Jain M, Dumeer S, Sirari N, Bansal M, Badgujar D. Chest wall tuberculosis - A clinical and imaging experience.Indian J Radiol Imaging. 2011 Jan;21(1):28-33
16. Huang CY, Su WJ, Perng RP.Childhood tuberculosis presenting as an anterior chest wall abscess.J Formos Med Assoc. 2001 Dec;100(12):829-31.
17. Ekingen G, Guvenc BH, Kahraman H.Multifocal tuberculosis of the chest wall without pulmonary involvement. Acta Chir Belg. 2006 Jan-Feb;106(1):124-6.
18. Jain S, Shrivastava A, Chandra D.Breast lump, a rare presentation of costochondral junction tuberculosis: a case report.Cases J. 2009 Sep; 9(2):7039
19. Koul PA, Ashraf M, Jan RA, Shah S, Khan UH, Ahmad F, Qadri BA, Bazaz SR.An elderly male with tubercular osteomyelitis of the chest wall.BMJ Case Rep. 2011 Mar ; 8:2011
20. Hossain M, Azzad AK, Islam S, Aziz M.Multiple chest wall tuberculous abscesses.J Pak Med Assoc. 2010 Jul;60(7):589-91.
21. Faure E, Souilamas R, Riquet M, Chehab A, Le Pimpec-Barthes F, Manac'h D, Debesse B.Cold abscess of the chest wall: a surgical entity?.Ann Thorac Surg. 1998 Oct;66(4):1174-8.
22. Paik HC, Chung KY, Kang JH, Maeng H.Surgical treatment of tuberculous cold abscess of the chest wall. Yonsei Med J. 2002 Jun;43(3):309-14.
23. Kim Y J, Jeon H J, Kim C H, Park J Y, Jung T H, LeeEB, Cha SI. Chest Wall Tuberculosis: Clinical Features and Treatment Outcomes. Tuberculosis and Respiratory Diseases,2009; 67(4): 318-324.
24. Keum DY, Kim JB, Park CK.Surgical treatment of a tuberculous abscess of the chest wall.Korean J Thorac Cardiovasc Surg. 2012 Jun;45(3):177-82.
25. Tanaka S, Aoki M, Nakanishi T, Otake Y, Matsumoto M, Sakurai T, Tada K, Ikeda A.Retrospective case series analysing the clinical data and treatment options of patients with a tubercular abscess of the chest wall.Interact Cardiovasc Thorac Surg. 2012 Mar;14(3):249-52.
26. Chung SY, Yang I, Bae SH, Lee Y, Park HJ, Kim HH, Im JG.Tuberculous abscess in retromammary region: CT findings.J Comput Assist Tomogr. 1996 Sep-Oct;20(5):766-9.
27. Supe AN, Prabhu RY, Priya H.Role of computed tomography in the diagnosis of rib and lung involvement in tuberculous retromammary abscesses.Skeletal Radiol. 2002 Feb;31(2):96-8.
28. Teo TH, Ho GH, Chaturverdi A, Khoo BK.Tuberculosis of the chest wall: unusual presentation as a breast lump.Singapore Med J. 2009 Mar;50(3):e97-9.
29. Buonsenso D, Focarelli B, Scalzone M, Chiaretti A, Gioè C, Ceccarelli M, Valentini P.Chest wall TB and low 25-hidroxy-vitamin D levels in a 15-month-old girl.Ital J Pediatr. 2012 Apr 17;38:12.
30. Papadimitriou JM, Spector WG.The origin, properties and fate of epithelioid cells.J Pathol. 1971 Nov;105(3):187-203.
31. Kamiyoshihara, M., Ibe, T., Iwasaki, Y., Takise, A., Itou, H., and Takeyoshi, I. Chest wall tuberculoma with tumor-like appearance. Respiratory Medicine CME, 2010; 3(2): 98- 100.
32. Aribas OK, Kanat F, Gormus N, Turk E.Cold abscess of the chest wall as an unusual complication of BCG vaccination.Eur J Cardiothorac Surg. 2002 Feb;21(2):352-4.
33. Vishnu Prasad NR, Balasubramaniam G, Karthikeyan VS, Ramesh CK, Srinivasan K.Melioidosis of chest wall masquerading as a tubercular cold abscess.J Surg Tech Case Rep. 2012 Jul;4(2):115-7.
34. Hsu HS, Wang LS, Wu YC, Fahn HJ, Huang MH.Management of primary chest wall tuberculosis.Scand J Thorac Cardiovasc Surg. 1995;29(3):119-23.
35. Das SK, Das A, Dey S. A rare case of staphylococcal cold abscess of anterior chest wall in an immunocompetent adult. Ann Trop Med Public Health 2012;5:142-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





