IJCRR - 6(2), January, 2014
Pages: 17-25
Print Article
Download XML Download PDF
OUTCOME OF PHYSICAL REHABILITATION IN PATIENTS WITH SPINAL CORD INJURY
Author: Devangi S. Desai
Category: Healthcare
Abstract:Introduction: Spinal Cord Injury (SCI) results in long-term disability and can dramatically affect quality of life. The effects of SCI have an impact not only on the lives of the client and family but also on society as a whole. Patients with SCI need a well coordinated, specialized rehabilitation program consisting of a team of physicians and health care professionals to provide the tool necessary to develop a satisfying and productive post injury life style. Objective: To assess effectiveness of physical rehabilitation in patients with spinalcord injury (SCI) and also to assess the functional improvement in patients with SCI with physical therapy. Methodology: In this study 30 paraplegic patients were selected, whose fracture level was below D9 vertebrae. Physical rehabilitation was started depending on the patient's assessment. In general physical rehabilitation includes ROM exercises and positioning, strengthening, mat activities, transfer training, wheelchair skills, gait training, etc. Patients were reevaluated after six weeks of rehabilitation. Outcome measures were ASIA motor score, ASIA sensory score and FIM to assess motor function, sensory function and level of independence respectively. Result: The result shows highly significant improvement in ASIA motor score, ASIA sensory score, motor score of FIM following six weeks of physical rehabilitation in paraplegics at 5% significance level except cognitive score of FIM. Conclusion: The conclusion of the study is that physical rehabilitation plays very important role in improving physical capacity of patients as well as in making them functionally as much independent as possible.
Keywords: Rehabilitation, Paraplegia, FIM, ASIA, Physical Therapy
Full Text:
INTRODUCTION
Spinal Cord Injury (SCI) typically results in impaired motion and loss of function, both of which are associated with a decrease in quality of life. 1 Spinal Cord Injury (SCI) is a low incidence, high cost disability requiring tremendous changes in an individual lifestyle.2 The effect of SCI have an impact not only on the lives of the client and family but also on society as a whole.3 Spinal injury units now exist worldwide and international symposia on the treatment of those with spinal cord lesions take place regularly.4 Improvements in administering care at the time of accident, technological advances in diagnosis and in management have contributed to a continuing fall in mortality and morbidity rates over recent years.5 Spinal cord injuries can be grossly divided into two broad etiological categories: Traumatic injuries and non-traumatic damage.2 Statistics from the NSCID (National Spinal Cord Injury Database) indicate that accidents involving motor vehicles are the most frequent cause of traumatic SCI (45.6%), followed by falls (19.6%), acts of violence (17.8%), recreation sports injuries (10.7%) and other etiologies (6.3%).6 Non-traumatic conditions that damage spinal cord are vascular malfunctions, vertebral subluxations secondary to rheumatoid arthritis, transverse myelitis, spinal neoplasm etc. They account for 30% of all spinal cord injuries. The areas of spine that demonstrate the highest frequency of injury are between C5 and C7 in cervical region and between T12 and L2 in the thoracolumbar region.2 The International Standards for Neurological and Functional Classification of Spinal Cord Injury (ISNCSCI) provide a straightforward, internationally accepted procedure for classifying spinal cord injury based on a systematic motor and sensory examination of neurological function.7 Functional Independence Measure (FIM) is devised to measure function for any disability. Each area of function is evaluated in terms of independence using a seven point scale.4 Patients with SCI need a well coordinated, specialized rehabilitation program consisting of a team of physicians and health care professionals to provide the tool necessary to develop a satisfying and productive post injury life style.8,9 The rehabilitation team for SCI is composed of the physician, orthopedic surgeons, physical therapist, occupational therapist, orthotist, nurses, speech language pathologist, dietician, psychologist, vocational counselor, social worker, engineer etc.10,11,12,13 The patients, their family members and NGOs are also the important part of rehabilitation team. A coordinated system of care shortens hospital stays and improves efficiency of functional gains during rehabilitation.14, 15 SCI usually happens to active, independent people who at one moment are in control of their lives and in the next moment are paralyzed, with loss of sensation and loss of body function and dependence on others for their basic needs so this study was chosen to assess effectiveness of physical rehabilitation in patients with spinal cord injury and also to assess the functional improvement in patients with SCI with physical therapy.
MATERIAL AND METHODOLOGY Study Design:
Prospective longitudinal follow up study
Study Setting: Physiotherapy department of Govt. Physiotherapy College, Ahmedabad. DURATION OF STUDY: 4 months. The duration of treatment program for each subject was 6 weeks. INCLUSION CRITERIAS Traumatic Spinal Cord Injury Operated cases Fracture below D9 vertebrae Duration since injury not more than 2 months Age 18 – 50 years Sex: Both males and females Willing to participate
EXCLUSION CRITERIA
Non traumatic cause of spinal cord injury Fracture above D9 vertebrae Patients treated conservatively Any other associated major neurological, musculoskeletal or cardiopulmonary condition Subject mentally unstable in the judgment of the investigator Subjects whose Modified Ashworth Scale is 3/4 or 4/4 at hip or knee at any time during the study
DATA COLLECTION AND PROCEDURE: MATERIALS
Plinth, Tilt table, Push up blocks Medicine ball, dumbbells Floor Mat, Wheelchair Parallel bars with mirror Posterior knee guard and Toe raising splint Walker, stick Evaluation format including ASIA motor form, ASIA sensory form, FIM Hammer, cotton, pin, pen
OUTCOME MEASURES
? American Spinal Injury Association (ASIA) motor score ? American Spinal Injury Association (ASIA) light touch score ? American Spinal Injury Association (ASIA) pinprick score ? Functional Independence Measure (FIM)
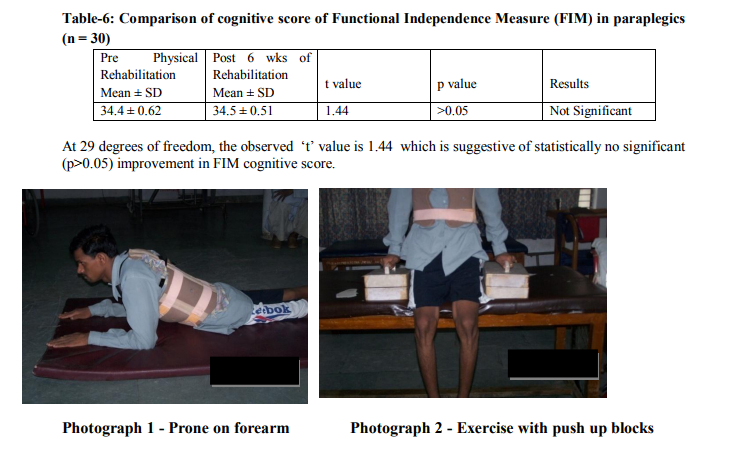
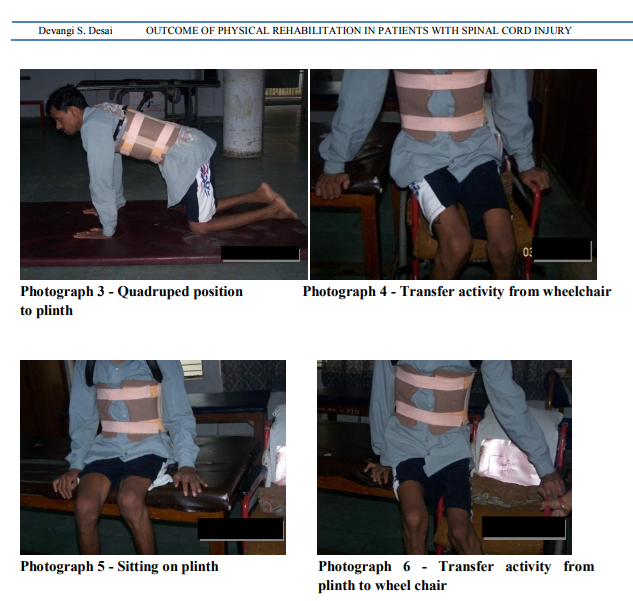
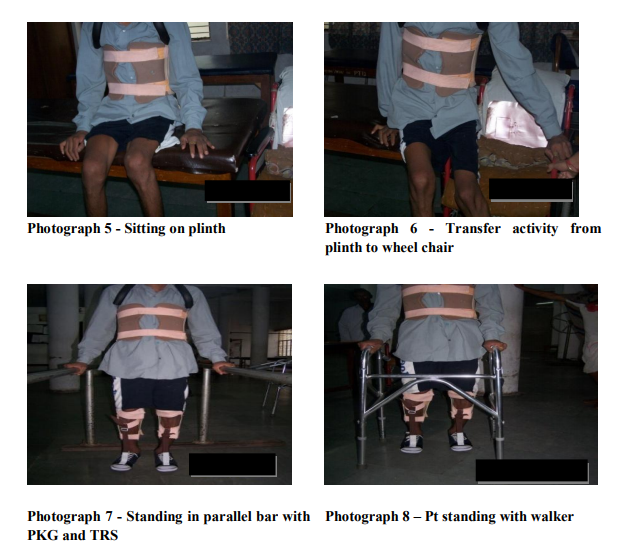
PROCEDURE For this study, a convenient sample of 30 paraplegic patients was taken from Paraplegia Hospital, Civil Hospital, Ahmedabad. All of them took part in the study on a voluntary basis after signing consent form. All the subjects were assessed as per the evaluation format. Those who fulfilled inclusion criteria were taken up for the study. The procedure was explained to all the subjects. Physical rehabilitation program was tailored for each subject depending on their evaluation. Orientation to vertical position was given by use of tilt table and by slowly elevating the head of the bed. Vitals were monitored during this period.2 To maintain R.O.M. in lower limbs, passive movements were given to hip, knee, ankle joints. Stretching exercises were also used mainly for gastro soleus and hamstring muscle. Hamstring stretching is given more emphasis to achieve a straight leg raise of 100 degrees. All upper extremity muscles were strengthened by progressive resistive exercises using manual resistance, weight cuffs or dumbbells. Mainly emphasis was given to shoulder depressors, triceps, and latissimus dorsi, which are required for transfers and ambulation. All the muscles of trunk and lower extremity which remain innervated were strengthened in similar manner.2 Mat activities2 constitute a major component of treatment during rehabilitation phase. Following activities were taught on mat. Rolling, Prone on forearm (photograph 1), Prone-on-hands position , Supine on elbows position, sitting, Balance exercises in sitting, Sitting push-ups using push-up blocks (photograph 2), Quadruped position (photograph 3) and Kneeling. Basic movements within the wheelchair like to manipulate the brakes, to remove the armrest, to pick up objects from the floor, to reach down to the foot plates; to lift the buttocks forward in the chair were taught. 10 to 15 seconds of pressure relief for every 10 minutes of sitting should become part of the patient’s daily routine. Techniques include wheelchair push-ups, hooking elbow or wrist around the push handle and leaning toward the opposite wheel.4 Transfer training was initiated after achievement of good sitting balance. Training was given on different surfaces such as bed, toilet, and chair to floor etc (Photograph 4-6). For standing and walking, basic requirements are to fix the knee joints and to hold the feet in dorsiflexion.4 To fix the knee joints and to maintain dorsiflexion of feet, posterior knee guard and toe raising splint were used respectively. With the use of necessary orthoses, standing between the parallel bars (Photograph 7) was given. Balance exercises in standing were given in parallel bar. Patient should learn to tilt his pelvis by using latissimus dorsi. Even pelvic side tilting was taught. Gait training was also given in parallel bars. Progression was made by making pt. walk with walker. Balance exercises in walker (Photograph 8) were also given. Patients were reevaluated after six weeks of rehabilitation for ASIA motor score, ASIA light touch score, ASIA pin prick score, Functional Independence Measure. In FIM, score of self care, sphincter control, transfers, and locomotion were considered as motor score and score of communication and social cognition were considered as cognitive score.
RESULTS
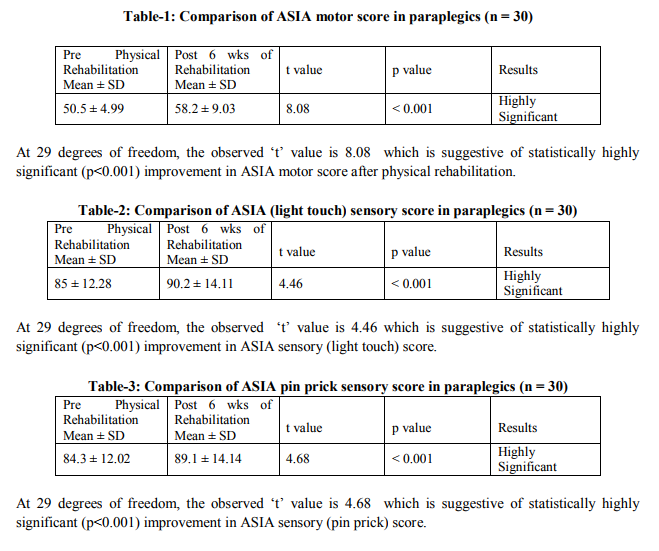
In this study 30 paraplegic patients were selected and evaluated by the physical therapist. Then physical rehabilitation was started depending onthe patients’ assessment. Patients were reevaluated after six weeks of physical rehabilitation. Here paired t-test was used for statistical analysis of outcome measures. Outcome measures were ASIA motor score, ASIA light touch score, ASIA pin prick score, motor score of FIM and cognitive score of FIM. Results of ASIA motor score (Table–1), ASIA sensory score (Table–2 and 3), motor score of FIM (Table–5) showed highly significant improvement after six weeks of physical rehabilitation at 5% level of significance. Results of cognitive score of FIM (Table–6) showed no statistically significant improvement after 6 weeks of physical rehabilitation.
DISCUSSION
Data collected through this study showed highly significant improvement in ASIA motor score, ASIA sensory score, motor score of FIM following six weeks of physical rehabilitation in paraplegics except cognitive score of FIM. In this study, standing and Gait training was given with the use of posterior knee guard and toe raising splint than Knee Ankle Foot Orthosis (KAFO) because of their cost effectiveness. Walker was used for gait training than forearm crutches because it increases base of support so patient feels secure. The other important reason is that all patients were coming from towns and residing on ground floor so they don’t have to climb stairs in their routine. In FIM transfer to bath, shower was taken as whether pt was able to transfer from wheelchair to floor because patients take bath on floor. Transfer to toilet was taken as whether pt was able to transfer to same level stool or chair because they didn’t have facility of western commode so they are going to use such modification. In this study 22 patients were men and 8 were women so 73% were men and 27% were women. This finding is nearer to finding of National Spinal Cord Injury Database in which 81% pts were men.6 The age of patients was ranging from 18-50 years with mean age of 27.83 years. At the starting of the study ASIA impairment scale was A for 17 patients, B for 7 patients, C for 7 patients so 53.33% had A scale, 23.33% had B scale and 23.33% had C scale. The mode of injury was fall from ht. in 13 pts. (43.33%), fall of heavy wt on back in 10 pts (33.33%), RTA in 7 pts. (23.33%). Muslumanoglu L, Aki S, Ozturk Y, et al 1997, Bode RK, Heinemann AW 2002, Jongjit J, Sutharom W, et al 2004, Hall KM, Cohen ME, et al 1999 , all these studies support the results found in this study but the follow up of pts was for a long duration. All these studies have shown improvement in ASIA motor score, ASIA light touch score and FIM motor score. They also didn’t find improvement in cognitive score of FIM.17, 18, 19, 20 M J De Vivo, J S Richards, S L Stover et al 1991 also found improved independence in activities of daily living following acute care and rehabilitation in pts with spinal cord injury.21 Sandy Stevens, Don Morgan, Ph.D.2 et al 2008 found strong positive association (r = .75; p<.05) between level of physical activity and quality of life so interventions aimed at promoting physical activity may be effective in improving quality of life in adults with spinal cord injury.22 This study also supports the role of physical rehabilitation in improving productivity of patients life. Rehabilitation should be continued after six weeks because interventions aimed at promoting physical activity beyond tradition rehabilitation period may be effective in improving quality of life in adults with spinal cord injury.22 Ota T, Nagata M et al 1996 found that FIM score reached the plateau in approximately 10 months, 6 months and 3 months post injury, in tetraplegia, paraplegia above T5 and that below T6 respectively.23 Ditor DS, Latimer AE et al 2003 concluded that findings of their study emphasize the importance of continued exercise adherence to the maintenance of exercise-related increases in psychological well-being among individuals with SCI.24 Bizzarini E, Saccavini M et al 2005 found that strengthening and aerobic rehabilitation programs for patients with subacute SCI should be limited to 4 weeks, followed by an independent maintenance exercise program. The strengthening program is safe for this patients.25 Noreau L, Shephard RJ 1995 concluded that quality of life is closely associated with independent living and, increasingly, it is a key outcome when measuring the success of rehabilitation. Consequently, research designs that examine the impact of exercise upon individuals with disabilities should not only include objective outcome measures, but also subjective measures relating to life-satisfaction and quality of life.26 Spinal Cord Independence Measure (SCIM) can be used which is a reliable disability scale and is more sensitive to changes in function in spinal cord lesion patients than the FIM.27
Limitation of the Study ? Small sample size ? Limited time duration of rehabilitation (6 weeks) ? Modification in the assessment of FIM score was required ? Patients treated conservatively were not selected. ? Quality of life was not assessed Future Suggestion ? The same study can be carried out by using SCIM than FIM which is more sensitive and more reliable to functional change in patients with spinal cord injury. ? Study can be carried out in patients with traumatic and non traumatic SCI as well as patients with any level of lesi
CONCLUSION
The conclusion of the study is that highly significant difference is found in ASIA motor score, ASIA sensory score and motor score of FIM following six weeks of physical rehabilitation in paraplegics. Hence physical rehabilitation plays very important role in improving physical capacity of patients as well as in making them functionally as much independent as possible.
ACKNOWLEDGEMENT
I am sincerely thankful to Dr. M. M. Prabhakar, Superintendent of civil hospital and Director of Paraplegia Hospital for allowing me to use the hospital records and facilities for preparation of my dissertation. I am profoundly thankful to Dr. Dilip A. Patel, for providing continuous guidance, inspiration, advice and suggestions throughout my study. I would like to thank Dr. Gita Kedia and Dr. Atul Trivedi, Assistant Professor of PSM department of B.J.Medical College for helping me in statistical analysis of the results. It is my privilege to thank all my staff members, internees and my colleagues of Government Physiotherapy College, Civil Hospital, Ahmedabad who have helped me during my study. I would like to thank my friends Nimisha Shah, Antara Desai and Arjun Menon for their genuine help and valuable guidance. I would like to thank all my patients for their active participation in this study, which would not have been possible without them. I express my deepest gratitude and dedicate this work to my parents, my husband, my daughter and all my family members without whose blessings and love this work would not have been materialized. I acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. I am also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. I am grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.

References:
REFERENCES
1. Boswell B, Dawson M, Heininger E. Quality of life as defined by adults with spinal cord injuries. J Rehabilitation 1998; 64:27-32
2. Susan B O’Sullivan, Thomas J Schmitz. Physical Rehabilitation. In: George D. Fulk,Thomas J Schmitz, Andrea L. Behrman, editors. Traumatic Spinal Cord Injury. 5th edition. Jaypee Brothers, F.A.Davis Company, Philadelphia; 2007.p.937-990.
3. Darcy A Umphred. Neurological Rehabilitation. In: Myrtice B. Atrice, Sarah A Morrison, Shari L. McDowell, Betsy Shandalov, editors. Traumatic Spinal Cord Injury. 4th edition. Mosby; 2001.p. 477-528.
4. Ida Bromley. Tetraplegia and Paraplegia A Guide for Physiotherapists. In: Ida Bromely, editor. Spinal Cord Injury. 5th edition. Churchill Livingstone;2006.p.1-9.
5. Jennifer A Pryor, S Ammani Prasad. Physiotherapy for Respiratory and Cardiac Problems Adults and Paediatrics. In: Trudy Ward, athryn Harris, editors. Spinal Cord Injury. 3rd edition. Churchill Livingstone;2005.p.537-547
6. Jackson AB, Dijkers M, Devivo MJ,et al. A demographic profile of new traumatic spinal cord injuries: Change and stability over 30 years. Arch Phys Med Rehabil 2004; 85:1740 – 1748.
7. American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury. Chicago: ASIA; 2002
8. Brown DJ. Spinal Cord Injuries: The last decade and the next. Paraplegia 1992; 30:77- 82.
9. Whiteneck GG, et al. Mortality, morbidity and Psychological outcomes of persons spinal cord injured more than 20 years ago Paraplegia1992; 30:617-630.
10. DeLisa JA, Martin GM, Currie DM. Rehabilitation medicine: past, present, and future. In DeLisa JA (ed). Rehabilitation Medicine Principle and Practice. Philadelphia: Lippincott; 1993. p. 3-27.
11. Dollfus P. Rehabilitation following injury to the spinal cord. J Emerg Med 1993;11:57-61.
12. Nickel VL. The rationale and rewards of team care. In Nickel VL, Botte MJ(eds). Orthopaedic Rehabilitation, 2nd ed. New York, Churchill Livingstone, 1992.p. 243-256.
13. Randall L. Braddom. Physical Medicine and Rehabiliation. In: Thomas N. Bryce, Kristjan T. Ragnarsson, Adam B. Stein, editors. Spinal Cord Injury. 3rd edition.Saunders;2007.p.1285- 1350.
14. Apple DF, Hudson LM, (eds).Spinal Cord Injury: The model. In proceedings of the National Consensus Conference on Catastrophic Illness and Injury, December 1989. Atlanta: Shepherd Center for treatment of spinal injuries, 1990.
15. Frost FS: Role of rehabilitation after spinal cord injury. Urol Clin North Am 1993;20:549- 559.
16. Hamilton BB, Anne Deutsch, Carol Russell,Roger C. Fiedler, Carl V Granger. Relation of disability costs to function: Spinal cord Injury. Arch Phys Med Rehabil 1993; 80: 385-391.
17. Hall KM, Cohen ME, et al. Characteristics of the Functional Independence Measure in traumatic spinal cord injury. Arch Phys Med Rehabil 1999; 80:1471-6.
18. Muslumanoglu L, Aki S, Ozturk Y, et al. Motor, sensory and functional recovery in patients with spinal cord lesions. Spinal Cord 1997; 35:386-9.
19. Bode RK, Heinemann AW. Course of functional improvement after stroke, spinal cord injury, and traumatic brain injury.Arch Phys Med Rehabil 2002; 83:100-6.
20. Jongjit J, Sutharom W, et al.Functional independence and rehabilitation outcome in traumatic spinal cord injury. Southeast Asian J Trop Med Public Health 2004; 35:980-5.
21. M J De Vivo, J S Richards, S L Stover et al. Spinal cord injury. Rehabilitation adds life to years. West J Med 1991; 154: 602–606.
22. Sandy L Stevens,Jennifer L Caputo, Dana K Fuller, Don Morgan. Physical Activity and Quality of Life in Adults with Spinal Cord Injury. J Spinal Cord Med 2008; 31:373-378.
23. Ota T, Akaboshi K, Nagata M, et al. Functional assessment of patients with spinal cord injury: measured by the motor score and the Functional Independence Measure. Spinal Cord. 1996; 34:531-5
24. Ditor DS, Latimer AE, Ginis KA, Arbour KP, McCartney N, Hicks AL.Maintenance of exercise participation in individuals with spinal cord injury: Effects on quality of life, stress and pain. Spinal Cord 2003; 41:446-50. 2
5. Bizzarini E, Saccavini M et al Exercise prescription in subjects with spinal cord injuries. Arch Phys Med Rehabil. 2005 Jun;86(6):1170-5.
26. Scelza WM, Kalpakjian CZ et al Perceived barriers to exercise in people with spinal cord injury.Am J Phys Med Rehabil. 2005 Aug;84(8):576-83.
27. Catz A, Itzkovich M, Agranov E et al. SCIM– –spinal cord independence measure: A new disability scale for patients with spinal cord lesions. Spinal Cord 1997; 35:850-6.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





