IJCRR - 6(3), February, 2014
Pages: 53-56
Print Article
Download XML Download PDF
VEIN OF GALEN MALFORMATION IN A 47 YEAR OLD MALE-A RARE ENTITY
Author: Subrata Chakrabarti , Koushik Pan
Category: Healthcare
Abstract:Vein of Galen Malformation (VGM) is a rare vascular malformation representing less than 1% of vascular intracranial abnormalities. It is a congenital anomaly and frequently detected during the last trimester of gestational age, during neonatal period or early childhood. Clinical manifestations can appear at any age but mainly in the neonatal or infancy stage in the form of heart failure, delayed neuropsychomotor development, hydrocephalus and seizures. First presentation in adult age is very rare. We report a case where a patient remained symptom free until presentation following generalized tonic clonic seizures at the age of 47 years.MRI brain and MR Angiography confirmed the presence of VGM.
Keywords: Vein of Galen malformation, generalized tonic clonic seizures
Full Text:
INTRODUCTION
The vein of Galen malformation is a rare cerebrovascular disorder which is characterized by an abnormal direct communication between one or several cerebral arteries and the vein of Galen. Posterior choroidal artery, anterior cerebral artery and transmesencephalic artery are respectively the most common arteries that join the malformation1 . During the neonatal or infancy period, the disease presents with congestive heart failure, intracranial hemorrhage, seizures or focal neurologic symptoms2 . Thereafter, progressive hydrocephalus or headache are the most frequent presentations of the VGM. Rare manifestation of VGM as occurs in adult may include seizures or hemiparesis3 .We report such a case of VGM in which the patient presented with seizures first at the age of 47 years.
CASE REPORT
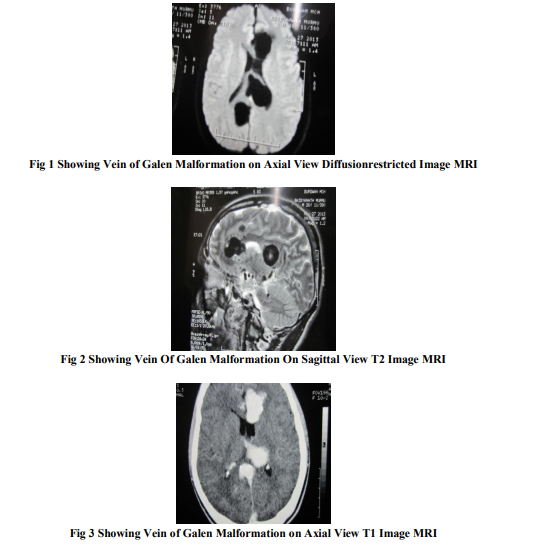
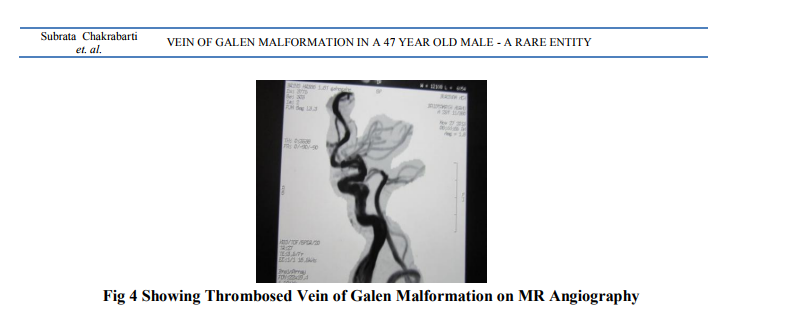
A 47 year old non diabetic, non hypertensive, occasional smoker and alcoholic male was brought to the emergency room because of generalized tonic-clonic seizures which started 1 hour ago. The seizures were associated with urinary incontinence and tongue biting. No antecedent history of head trauma or ingestion of any toxin or recent alcoholic binge or any febrile episode was noted. No history of seizures was present in the past and no similar family history was found.He was born as a normal vaginal delivery and achieved normal developmental milestones at appropriate age and had no history of scholastic performance. During childhood, there was no neuropsychomotor developmental delay. Past medical history was insignificant. Physical examination on admission revealed a blood pressure 130/76, heart rate 112/minute, regular and respiratory rate 26/minute. He was frothing at the mouth and had urinary incontinence. No evidence of any head trauma was noted. No sign of limb abnormality or any skin tag or any facial deformity was noted. No sign of meningeal irritation was found. Fundoscopy revealed features compatible with mild papilledema bilaterally. On admission, he was treate Lorazepam and injection Phenytoin on the lines of standard management as a case of status epilepticus. Routine blood parameters were within normal limits except evidence of lactic acidosis. CSF study was within normal limits. MRI brain was ordered after patient was stable which revealed features compatible with partly thrombosed Vein of Galen Malformation. Subsequently MR Angiography was done which confirmed the diagnosis of VGM. As the aneurysm was already partly thrombosed and also as there were no signs or symptoms of intracranial hypertension or hydrocephalus, the patient was not referred for surgery or endovascular treatment. Improvement in the level of consciousness and absence of seizures episodes were noted during the follow-up period while the patient was kept on therapy for seizures.
DISCUSSION
VGM is a vascular abnormality1 typically found in children2 . The two most used classifications for vein of Galen malformations are those proposed by Lasjaunias et al.4 . and Yasargil5 . According to Lasjaunias et al.4 , these malformations can be divided into mural and coroidal types depending on the fistula localization. The coroidal type is characterized by multiple fistulas at the anterior and terminal segment of the median prosencephalic vein. This type usually presents at the neonatal period causing serious heart failure leading to multiple organ failure and death. The mural type has the fistula at the vascular wall usually at the lateral-inferior wall of the median prosencephalic vein. They are of slow flow and asymptomatic. Yasargil's lesions types 1, 2 and 3 are direct fistulas between the malformations and the vein of Galen. Lesion type 4 are parenchymal arteriovenous malformations, which drain directly into the vein of Galen. It is typically diagnosed during the neonatal period or in childhood with features of heart failure , macrocephaly. Adults may present with slow-flow fistulas, headaches, seizures, hydrocephalus6 . Angiography is the gold standard for the diagnosis of VGM which shows the relationship of the cerebral venous system and vascular relationships to the fistula7,8. Because of its rarity in adults, there is still insufficient information about the course of this disease during adult age. In adults, isolated case reports have been mentioned by some authors9-12. Use of oral contraceptives13, postpartum status14, sickle cell anemia15, and aseptic meningitis16 are considered risk factors related to thrombosis of the vein of Galen. Treatment of VGM is case-based. No standard treatment guideline is available. Even considering recent micro-neurosurgery advances, the lesion resection usually is not possible. However, recently it has been shown, interventional neuroradiology can lead to good results. Nowadays, endovascular techniques are the procedures of choice17. However, conservative treatment may be considered, especially for the elderly with co-morbidities, and neurological stable patients without severe neurological signs or symptoms. The presence of partial thrombosis in the malformation, absence of signs or symptoms of intracranial hypertension, and pharmacological control of seizures led us to conservative treatment of the patient presented here.
CONCLUSION
Possibility of VGM as the underlying etiology in a case of a 47 year old patient presenting for the first time with generalized tonic-clonic seizures is relatively remote but appropriate investigations namely MRI brain and MRAngiography can unravel this rare but fascinating entity.
ACKNOWLEDGEMENT
We wish to thank the faculty of Radiology Department, SSKM for prompt performance of the MRI and MRA of the patient which helped us
in reaching this interesting diagnosis and also providing us with valuable inputs regarding the disease which helped us in preparing the manuscript. CONFLICT OF INTEREST: NIL
References:
REFERRENCES
1. Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989;31:109- 128.
2. Jones BV, Bal WS, Tomsick TA, Millard J, Crone KR. Vein of Galen aneurysmal malformation: diagnosis and treatment of 13 children with extended clinical follow-up. AJNR 2002;23:1717-1724.
3. Abe T, Matsumoto K, Kiyota K, Tanaka H. Vein of Galen aneurysmal malformation in an adult: a case report. Surg Neurol 1996;45:39- 43.
4. Lasjaunias P, Ter Brugge K, Ibor LL, et al. The role of dural anomalies in vein of Galen aneurysms: report of six cases and review of the literature. AJNR 1987;8:185-192
5. Yasargil MG. Microneurosurgery IIIB. New York: Thieme Medical Publishers, 1988: 323- 357.
6. Rosenfeld JV, Fabinyi GC. Acute hydrocephalus in an elderly woman with an aneurysm of the vein of Galen. Neurosurgery 1984;15:852-854.
7. Seidenwurm D, Berenstein A, Hyman A, Kowalski H. Vein of Galen malformation: correlation of clinical presentation, arteriography, and MR imaging. AJNR 1991;12:347-354.
8. Hassan T, Timofeev EV, Ezura M, et al. Hemodynamic analysis of an adult vein of Galen aneurysm malformation by use of 3D image-based computational fluid dynamics. AJNR 2003;24:1075-1082.
9. Cordonnier C, Lucas C, Leclerc X, Gauvrit JY, Leys D. Giant arteriovenous malformation of the vein of Galen in a 50 year old man. Rev Neurol (Paris) 2002;158:731-733.
10. Porzionato A, Macchi V, Parenti A, De Caro R. Vein of Galen aneurysm: anatomical study of an adult autopsy case. Clin Anat 2004;17:458-462.
11. Xavier J, Alves V, Vasconcelos C, Leite A, Cruz R. Aneurysmal malformation of the vein of Galen in adults. Acta Med Port 2003;16:203-206.
12. Ribeiro VT, Botelho LF, Lopes AC, et al. Choroidal type aneurysmal malformation of the vein of Galen associated with DandyWalker malformation in an adult. Acta Med Port 2003;16:217-220.
13. Marques MCP, Pires LA, Damasceno CA, Felício AC, Atala A, Franco GM. Galen vein thrombosis: case report. Arq Neuropsiquiatr 2003;61: 285-287.
14. Krenz I, Power KJ. Postpartum thrombosis of the great vein of Galen. Anaesthesia 1990;45:643-645.
15. Ildan F, Cetinalp E, Bagdatoglu H, Boyar B. Evolution of thrombosis of the vein of Galen in sickle cell disease. J Child Neurol 1993;8:189-191.
16. Collins JJ, Fisher WS. Vein of Galen aneurysm presenting with recurrent aseptic meningitis and subsequent spontaneous thrombosis. Surg Neurol 1990;33:325-328.
17. Shin M, Kurita H, Tago M, Kirino T. Stereotactic radiosurgery for tentorial dural arteriovenous fistulae draining into the vein of Galen: report of two cases. Neurosurgery 2000;46:730-733
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





