IJCRR - 6(3), February, 2014
Pages: 01-06
Print Article
Download XML Download PDF
MORPHOMETRIC ANALYSIS OF CHORDA TENDINAE OF MITRAL VALVE IN HUMAN HEARTS
Author: S. Kavitha, A. Anand, K.Y. Manjunath
Category: Healthcare
Abstract:Objective: Chorda tendinae are the connecting link between heart valves and the ventricular chambers. In valve replacement surgeries, the effective post surgical performance of the valve depends on the length of the chordae which are anchored. This study aims at giving a definitive measurement of the chordae from the papillary muscle of the ventricle to the leaflet of the valve so that an operating surgeon can have a fair idea of how much length of the chordae can be sacrificed. Materials and Methods: 50 human hearts were studied and the length, breadth and the numerical count and the position of the chordae of the mitral valve were studied. Results: The mean length of anterior chorda was 12.77mm \?4.03 S.D and posterior 12.33mm \?3.89 S.D. The mean breadth of anterior chorda was .28mm\? .20 S.D and posterior .25mm \? 0.14 S.D .The anterior papillary muscle contained around an average of 10.42 \? 2.48 S.D chordae and the posterior papillary muscle contained around an average of 9.72 \? 2.39 S.D chordae. Based on the position of attachment, lateral chordae were approximately 73.22% and apical chordae 19.06% and marginal chordae was 7.72%. Conclusion: The length and the breadth of the chordae of the anterior papillary muscle were more than the length and breadth of the posterior papillary muscle. Approximate measurements of chordae will give a definitive value in mitral valvular replacement surgeries.
Keywords: chorda, chordae, tendinae, mitral valve, ventricle, leaflet, papillary muscle
Full Text:
INTRODUCTION Cardiovascular diseases are an important cause of morbidity and mortality in our modern world. This is due to affluent practices of the population with associated factors like obesity and a sedentary lifestyle combined with a diet rich in fats. Whatever be the underlying cause which results in a cardiac affliction, it has affected the quality of life and a significant reduction in the life expectancy of individuals with cardiac ailments. Advancements in cardiothoracic surgery has resulted in replacement of heart valves using artificial heart valves which has a definitive life span and issues of compatibility. Of late, cadaveric heart valve replacements have gained precedence. In cadaveric heart valve replacement surgeries, thorough knowledge of valvular anatomy and dimensions of the valves is a must before planning a surgical procedure. Preservation of chordae either in artificial heart valve and cadaveric heart valve replacement surgeries has been advocated for efficient post surgical valvular function of the heart. This study pertains to supplementing the preservation of chordae of the valvular apparatus in replacement surgeries. Detailed approximate measurements of the dimensions of the mitral valve apparatus will serve as a guideline for determining the architecture of chordae during valve replacements. Preservation of chordae is advocated as it contains extensions of ventricular conducting tissues1 . A detailed classification of the types of chordae is not possible because of variations in individuals and in places of free edge of the valve where the chordae are not attached become prone to prolapse1 . This assumes significance because anatomical or near anatomical alignment of the mitral valve has to be maintained post surgically for efficient function of the heart. The opening of the mitral valve is smaller than the tricuspid opening and the annulus itself is made of fibrocollagenous elements of different consistencies which help the annulus change in the shape and dimensions during the phases of cardiac cycle which ensures an optimal efficiency in valvular action2 . Near normal alignment of mitral valve in cadaveric heart valve and artificial heart valve replacements can be achieved by paying attention to the presurgical dimensions of the fibrocollagenous structure of the mitral valve. This study aims to give the operating surgeon a guideline for approximate measurements of chordae tendinae of the mitral valve. Many studies have elaborated on the importance of preservation of the chordae which reduces the risk of catastrophic ventricular rupture3 . Approximate measurements of the chordae have to be known because there is always a possibility of over shortening of the chordae during valve replacement procedures which can result in rupture of papillary muscle4 . This study assumes significance since in conventional operative procedures for replacement of the mitral valve as there is a loss of continuity between the annulus of the mitral valve and the papillary muscles. This loss of continuity results in a decrease in left ventricular ejection fraction and an increase in after load by eliminating regurgitation in patients with mitral regurgitation5 . Left ventricular function in post mitral valvular surgical procedures depend on preservation of chordae tendineae6 because preserved chordae is bound to promote effective valvular function. Moderator bands are structures which connect the septum of the ventricles to the ventricular free wall. These moderator bands histologically are made of cardiac muscle fibres, blood vessels and purkinje fibres and are directly involved in the conduction of electrical impulses in the heart. Presence of conducting structures in the chordae tendinae as an extension of ventricular conducting system will have to be taken into consideration in valve replacement surgeries 7, 8. Hence histological study of the chordae was also performed to demonstrate the presence of conducting tissues of the chordae in the present study.
MATERIALS AND METHODS
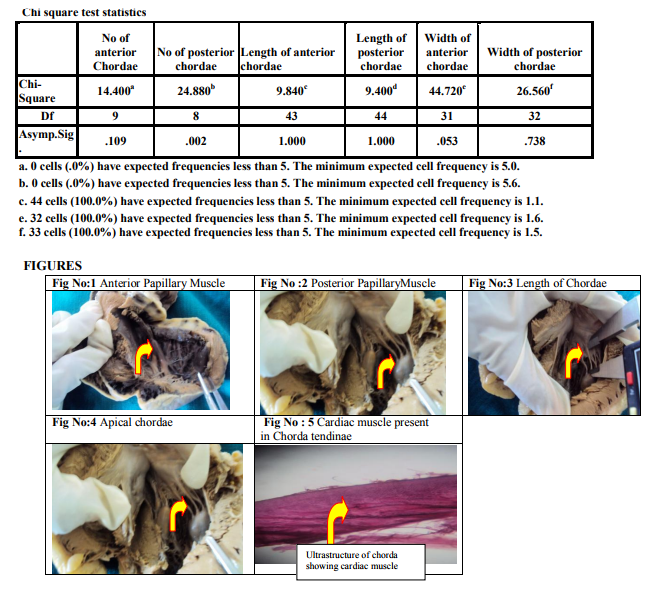
The specimens for the study were obtained from the departments of Forensic medicine and Anatomy of VMKV Medical College & Hospitals, Salem after obtaining necessary clearances from the Institutional Review Board and Ethical Committee for conducting the study. The specimens were fresh cadaveric human hearts numbering 50. The equipments utilized for the study were digital vernier calipers, hand lens, measuring scale and digital photographic equipment. Tissue sample was taken from a few chordae and paraffin wax blocks were prepared after processing, sections were taken and stained and examined under microscope for evidence of any conducting structures present in the chordae. The study pertained only to the chordae and papillary muscles attached to the mitral valve. The requisite parameters of the study were length (fig – 3) and breadth of the chordae, the number of chordae and the position of attachment of the chordae (fig – 4) between the papillary muscle and the annulus was documented. The length of the chorda was measured from the point of origin from the papillary muscle to the point of attachment to the leaflet. The breadth of the chorda was taken at the midpoint of the chorda after measuring the length. The number of chordae was enumerated for both anterior (fig – 1) and posterior papillary (fig – 2) muscles. The measurements obtained from the set parameters were documented.
Statistical Analysis
The measurements were subjected to statistical analysis using SPSS software version 16. The range, standard deviation and mean were calculated. Chi square test was done to compare the variables.
RESULTS
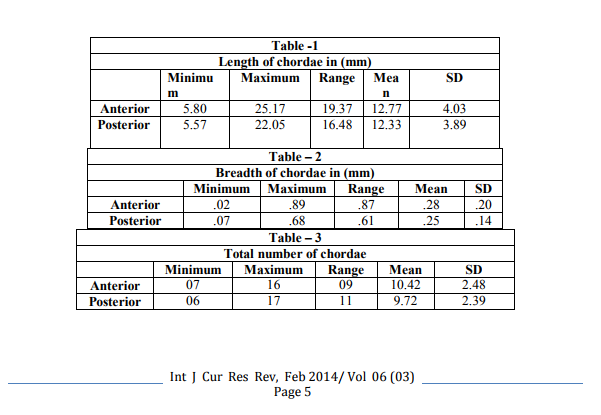
The length of the chordae in anterior papillary muscle ranged from a minimum of 5.80mm to a maximum of 25.17mm with a mean of 12.77mm. The length of chordae in posterior papillary muscle ranged from a minimum of 5.57mm to a maximum of 22.05mm with a mean of 12.33mm. The length of the chordae of anterior papillary muscle was marginally higher than that of the posterior papillary muscle. The breadth of the chordae in anterior papillary muscle ranged from a minimum of .02mm to a maximum of .89mm with a mean of .28mm.The breadth of chordae in posterior papillary muscle ranged from a minimum of .07mm to a maximum of .68mm with a mean of .25mm. The breadth of the anterior papillary muscle was marginally higher than that of posterior papillary muscle. The total number of chordae in anterior papillary muscle ranged from a minimum of 07 to a maximum of 16 with a mean of 10.42 chordae. The total number of chordae in the posterior papillary muscle ranged from a minimum of 06 to a maximum of 17 with a mean of 9.72chordae. In the present study the anterior papillary muscle contained more chordae than the posterior papillary muscle. The position of attachment of chorda tendinae in both anterior and posterior papillary muscles, the laterally attached chordae were 73.22%, apical chordae 19.06% and marginal chordae were 7.72%. The percentage of lateral chordae was more in anterior and posterior papillary muscles The chordae tendinae were stained with haematoxylin and eosin (fig – 5) which showed evidence of collagen fibres and cardiac muscle which collates that the chordae does contain conducting tissue.
DISCUSSION
Although numerous studies have elaborated on the position and attachment of chordae, enumerates the length and breadth of chordae from the tip of papillary muscle to the septal leaflet. These measurements will give a definitive value for preserving the chordae in mitral valvuloplasty performed for mitral valve insufficiency. Post surgical efficiency of the left ventricular function improved after preservation of chordae in patients who underwent mitral valvuloplasty9 . In mitral incompetence the length, location and number of chordae are required to estimate the reattachment of the chordae to the ventricular wall10. The chordal length and breadth measurements play an important role as a long length or short length would lead to mitral valve prolapse syndrome11. The length and breadth of the chordae of anterior and posterior papillary muscles will provide an approximate guideline value for determining the position and attachment of a prosthetic valve. Various authors have elaborate classifications for attached position of the chordae to the papillary muscle. The length and breadth of the chordae is determined based on the position of attachment to the papillary muscle. Based on the position of chordae, the attachments can be apical, marginal and lateral. This inequality in the arrangement of chordae determines the efficacy and robust function of the mitral valve. Hypothetically if all chordae were of equal length and with the same positional attachment, mechanical function of the mitral valve would be inefficient. Too many chordae also will interfere with left ventricular function12 . The length and breadth of the chordae determines the positional attachment of a prosthetic mitral valve in cases where the preservation of chorda papillary complex is advocated. Any laxity in reattachment of the chorda leads to discrepancy of effective valvular function and leads to mitral valve prolapse11 . The measurement of parameters obtained from the present study correlates with a study performed in the United Kingdom13. The sections taken from the chordae when analyzed under microscope after staining with haematoxylin and eosin showed evidence of wavy collagen and cardiac muscle tissue similar to the study performed earlier13. The presence of collagen and some amount of elastic fibres in the chordae is suggestive of the enormous amount of force required for repetitive movements of the valve and optimal performance of the left ventricle. Preservation of the chordae in mitral valve replacement procedures caused significant reduction in the operative mortality14. The preservation of chordae of both anterior and posterior papillary muscles of left ventricle during mitral valve replacement provides a tethering effect of chordal support and totally prevents mitral regurgitation5 . In conventional mitral valve replacements, the mitral regurgitation is more.
CONCLUSION
To summarize as evident from the analysis of the set parameters, it is observed that the length and breadth of the chordae of anterior papillary muscle are higher than the length of the chordae of the posterior papillary muscle. Numerically the chordae of the anterior papillary muscle were significantly more than the chordae of the posterior papillary muscle. In both anterior and papillary muscles of the left ventricle, laterally attached chordae were more in number than the apical and marginal chordae. In the present study the number of apical chordae was more in anterior papillary muscle and the percentage of marginal chordae was more in posterior papillary muscle of the left ventricle. The results obtained from the present study can be used as guideline for measurements in prosthetic valve replacements for mitral valve and will help the surgeons in planning a procedure and have a reduction in morbidity and mortality in critical situations.
ACKNOWLEDGEMENTS
The authors sincerely wish to thank the management, administrators and the Professor and Head of the department of Anatomy and Forensic Medicine of Vinayaka Missions Kirupananda Variyar Medical College, Salem for their whole hearted support and permissions to utilize their resources and conduct this study. The authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
REFERENCES
1. Susan Standring. Gray’s Anatomy, 39th Edition. Anatomical basis of clinical practice, Churchill Livingstone, London. 2005; 39:1008.
2. Susan Standring. Gray’s Anatomy, 40th Edition. Anatomical basis of clinical practice, Churchill Livingstone, London. 2008; 40:970.
3. Miller DW Jr, Johnson DD, Ivey TD. Does preservation of the posterior chordae tendinae enhance survival during mitral valve replacement? Ann Thoracic Surg 1979; 28:22- 7.
4. Trites PN, Kiser JC, Johnson C, et al. Occlusion of Medtronic Hall mitral valve prosthesis by ruptured papillary muscle and chordae tendinae. J Thorac Cardiovasc Surg 1984; 88:301-2.
5. Shigehito Miki, Kenji Kusuhara, Yuichi Ueda et al. Mitral valve Replacement with preservation of chordae tendinae and papillary muscles in Ann Thorac Surg Jan 1988; 45: 28- 34.
6. Spence PA, Peniston CM, David TE, Mihic N, et al. Toward a better understanding of etiology of left ventricular dysfunction after mitral valve replacement: An experimental study with possible clinical implications. Ann Thorac Surg 1986; 41:363-371.
7. Gulyaeva AS, Roshchevskaya IM. Morphology of moderator bands (Septomarginal Trabecula) in porcine heart ventricles. J Vet.Med – Anatomia, Histologia, Embryologia, 2012; 41:1-9.
8. Roberts WC, Cohen LS .Anomalous left ventricular band. An unemphasized cause of a precordial musical murmur. Am.J.Cardiol, 1969; 23:735-8.
9. Jose Luiz Dancini, Pablo Maria Alberto Pomerantzeff,Guilherme Sobreira Spina, et al. Valve Replacement with Chordal preservation and Valvuloplasty for Chronic Mitral Insufficiency. Arq Bras Cardiol 2004; volume 82: 243-50.
10. Gerda L Van Rijk et al. Evolving significance of Human chordae Tendineae. Am. J. of Card Surg 1994; 9:255 – 261.
11. Harken D. E, Ellis L.B, Ware P.F, Norman L.R. The surgical treatment of mitral stenosis, valvuloplasty in New England J Med 1948; 238: pp: 801 – 806.
12. Silverman M E, Hurst J.W, et al. The mitral complex: interaction of anatomy, physiology and pathology of the mitral annulus, mitral valve leaflets, Chordae tendineae and papillary muscle. Am heart J 1968; 76: 399.
13. Millington-Sanders C, Meir A, Lawrence L, Stolinski C. Structure of chorda tendineae in the left ventricle of the human heart. Journal of Anatomy. 1988; 192:573 – 581.
14. Lillehei CW, Levy MJ, Bonnabeau RC. Mitral valve replacement with preservation of papillary muscles and chordae tendineae. J Thorac Cardiovasc Surg 1964; 47:532.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





