IJCRR - 6(4), February, 2014
Pages: 42-45
Date of Publication: 20-Feb-2014
Print Article
Download XML Download PDF
SUBCUTANEOUS PHAEOHYPHOMYCOSIS - A RARE CASE REPORT
Author: Atul K. Jain, Harsh Kumar, Banyameen Iqbal, Tushar Kambale
Category: Healthcare
Abstract:Phaeohyphomycosis is a heterogeneous group of fungal infections caused by a variety of naturally pigmented fungi. A 53 year old woman presented with painless swelling over the lower one third of the left leg medial aspect, of one year duration. Local examination revealed a firm, fluctuant, mobile swelling measuring about 6×4 cm situated over the medial aspect of the lower left leg. It was not painful or tender. Microscopic examination revealed fungal granuloma (the causative organism morphologically identical to pheohypomycosis)
Keywords: Fungal infections, Pigmented fungi, Granuloma
Full Text:
INTRODUCTION
The taxonomy and terminology of dematiaceous fungal infections are difficult. The term phaeohyphomycosis was first coined by Ajello in 1974.1 Earlier, some of the authors had proposed terms such as chloroblastomycosis.2 Later, this term was modified as chloromycosis.3 Phaeohyphomycosis is a heterogeneous group of fungal infections caused by a variety of naturally pigmented fungi. The aetiological agents of this mycosis, which include more than 80 genera and species, are common saprophytes found in soil, wood, and decaying vegetable matter.4,5 Phaeohyphomycosis is rare in humans, although it is more common in immunocompromised individuals.6 Phaeohyphomycosis affects either superficial tissues, such as the skin, cornea, and subcutaneous tissue, or deep tissues, such as the brain and cases of phaeohyphomycosis are classified accordingly.5 The infection typically follows traumatic implantation of the fungi by a wooden splinter or a thorn prick and manifests as a cystic lesion. Herein, we report a typical case of a subcutaneous phaeohypomcosis occurring in an elderly woman.
CASE REPORT
A 53 year old woman presented with painless swelling over the lower one third of the left leg medial aspect, of one year duration. Initially the swelling was small but gradually increased in size. The patient, a labourer had a thorn prick injury while clearing wild bushes one year ago. The Swelling was noticed a few months after the incident. On examination, her general condition was good. She was afebrile. Other systemic examination results were within normal limits. Local examination revealed a firm, fluctuant, mobile swelling measuring about 6×4 cm situated over the medial aspect of the lower left leg. It was not painful or tender. It was not attached to the underlying bone. USG of swelling suggested a differential diagnosis of thrombosed varicose veins, multiple chronic abscesses, Neoplasm. Haemoglobin level was 12.6, TLC 6800 gm/dl, platelet 2.8. PBS was normocytic normochromic, random, blood sugar 176%. The urinalysis results were normal. RFT, LFT was within normal limits. HIV and HBSag negative. Patient was a known case of hypertension and diabetes Mellitus. Pt was sent for FNAC – pus like material admixed with blood was aspirated. Stained smears showed mainly inflammatory cell chiefly polymorphs along with few giant cells in necrotic background. The features were suggestive of an inflammatory lesion or abscess and biopsy was advised.
OPERATIVE FINDINGS
During surgery the swelling was easily separated from the surrounding tissue and removed completely. When the excised cyst was cut open in the surgical theatre, it expelled purulent material. The cyst was immersed in 10% formalin and sent for histopathological examination.
GROSS FINDINGS:
The excised specimen was received as multiple tissue pieces, the largest measuring 5x1.2x1 cm. Other pieces altogether measured 3.5x3.2x1cm.The cut surface was soft to firm in consistency, homogenous, and greyishwhite in colour.
MICROSCOPY:
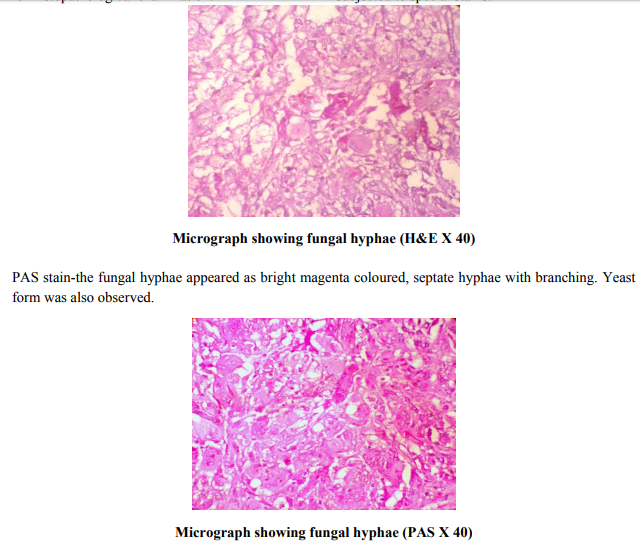
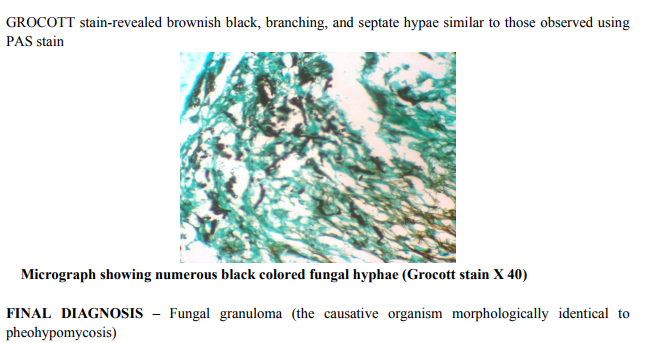
Multiple sections were taken, analysed and showed chronic granulomatous inflammation comprising of numerous epitheloid cell granulomas along with giant cells, macrophages and lymphocytes and areas of necrosis. In foci, pigmented, branching, septate fungal hyphae were visualised which were located within and in between the giant cells. These hyphae morphologically resembled pheohypomycosis species. Tissue sections were subjected to special stains.
DISCUSSION
Phaeohyphomycosis is an infection caused by a heterogeneous group of phaeoid fungi. The disease is more of a histopathological, rather than a clinical entity.7 More than 130 fungal species belonging to 70 diverse genera have been reported as causative agents in human and animal phaeohyphomycosis.8 Subcutaneous phaeohyphomycosis occurs throughout the world in all climatic conditions. In India, the climate ranges from tropical to temperate and the disease has been reported from the extreme north to south, except for the western and eastern regions.9 Males are commonly involved because of their outdoor occupation. In a review published in 2002, eighteen cases of subcutaneous phaeohyphomycosis were reported from India. The article documented involvement of the leg, foot, arm, toes, nails, waist, buttock, left thumb, hand, wrist while some patients had disseminated disease.9 Phaeohyphomycosis is more common in immunodeficient or debilitated hosts and rarely affect healthy individuals.6 Phaeohyphomycosis has been clinically divided into superficial (cutaneous and corneal), subcutaneous, and systemic phaeohyphomycosis by McGinnis.5 Subcutaneous phaeohyphomycosis usually results in a painless subcutaneous abscess or in verrucous plaques on the hand, arm, face, or neck. Although phaeohyphomycosis has distinct clinical features, it is occasionally confused with chromoblastomycosis There are significant clinical differences between chromoblastomycosis and phaeohyphomycosis. Typically, phaeohyphomycosis follows traumatic implantation of the fungus by a wooden splinter, or a thorn as in our case. Lymphangitis and regional lymphadenopathy are unusual. Hence, infective aetiology is often not considered. Our case was clinically suspected to be a multiple chronic absess or a neoplasm. The host reaction to phaeohyphomycosis is similar regardless of the aetiological agent and the anatomic site of involvement. The lesion is usually situated in the dermis and the subcutaneous plane and is characterised by cyst formation with dense collagenous connective tissue with central suppurative necrosis. The overlying epidermis is usually normal (In chromoblatomycosis epidermis is hyperplastic). The wall contains compact aggregates of epithelioid cell histiocytes and numerous giant cells. Pigmented moniliform (spherical and uniform segmentation) fungal elements are usually present inside the giant cells or extracellularly in the necrotic debris. In case of chromoblastomycosis, muriform (brick like cell with both longitudinal and transverse septa) with sclerotic bodies fungi may vary in their degree of pigmentation and may also appear as infrequently branching hyphae measuring 2–6 μm wide. The fungi are closely septate and constricted at their prominent septations.6 Our case exhibited the typical features of phaeohyphomycosis. Regarding the management of subcutaneous phaeohyphomycosis, excision of the localised lesion is usually curative.10
CONCLUSION
Subcutaneous phaeohyphomycosis is a rare fungal infection. It’s caused by a broad variety of dematiaceous fungi. Simple excision is usually curative for localized lesions. When phaeohyphomycosis is suspected, the identification of the fungus by routine histopathological examination is offen sufficient to arrive at a diagnosis of phaeohyphomycosis.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in reference of the manuscript. The Authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been revised and discussed.
References:
1. Ajello L, George LK, Steigbigel RT, Wang CJ. A case of Phaeohyphomycosis caused by new species of phialophora. Mycology 1974;66:490.8.
2. Terra F, Torres M, da Fonseca O. Novo type de dermative verrucosa mycose por: Acrothecacom association de leishmoniosa. Braz Med1992;2:363-8.
3. Moore M, de Alemeida F. Etiologic agents of chromomycosis (Chromoblastomycosis of Terra, Torres Fonseca and Leao 1992) of North and South America. Rev Bio Hyg 1935:6:94.7.
4. Fader RC, McGinnis MR. Infections caused by dematiaceous fungi: Chromoblastomycosis and phaeohyphomycosis. Infect Dis Clin North Am. 1998;2(4):925–938. [PubMed]
5. McGinnis MR. Chromoblastomycosis and phaeohyphomycosis: New concepts, diagnosis, and mycology. J Am Acad Dermatol. 1983;8(1):1–16. [PubMed]
6. Tendolkar UM, Kerkar P, Jerajani H, Gogate A, Padhye AA. Phaeohyphomycotic ulcer caused by Phialophora verrucosa: Successful treatment with itraconazole. J Infect. 1998;36(1):122–125. [PubMed]
7. Suh MK. Phaeohyphomycosis in Korea. Nippon Ishinkin Gakkai Zasshi 2005;46:67- 70.
8. Chandra J. Phaeohyphomycosis in Medical Mycology. 2nd ed. Mehta Publication; 2003. p. 147-54.
9. Sharma NL, Mahajan V, Sharma RC, Sharma A. Subcutaneous Phaeohyphomycosis in India: A case report and review. Int J Dermatol 2002; 41:16- 20.
10. Chandler FW, Watts JC. Phaeohyphomycosis. In: Connor DH, Chandler FW, Schwartz DA, Manz HJ, Lack EE, editors. Pathology of infectious diseases. Hong Kong: Appleton and Lange; 1997. pp. 1059–1066.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





