IJCRR - 6(4), February, 2014
Pages: 26-30
Date of Publication: 20-Feb-2014
Print Article
Download XML Download PDF
STUDY OF NEWER INVASIVE AND NON-INVASIVE METHODS OF HAEMOGLOBIN ESTIMATION IN BLOOD DONOR SCREENING - A STUDY ON 200 DONORS
Author: Pankaj Malukani, M. D. Gajjar, R. N. Gonsai, Nidhi Bhatnagar, H. M. Goswami
Category: Healthcare
Abstract:Background: Despite the wide range of methods available for measurement of haemoglobin (Hb), no single technique has emerged as the most appropriate and ideal for a blood donation setup. To cater to this need both invasive and non-invasive techniques of haemoglobin estimation were analysed. Aims and Objectives: To compare invasive and non-invasive methods of haemoglobin estimation in terms of accuracy, sensitivity and donor satisfaction. Materials and Methods: A prospective study utilizing 200 blood samples was carried out in a blood donation setting for quality evaluation of five methods of haemoglobin estimation: Haematology cell analyser (reference), DiaSpect, CuSO4, HemoCue and NBM-200. Results: Mean value of HemoCue (mean \? SD = 13.8 \? 1.7 g/dl) was higher by 0.26 compared to reference (mean \? SD = 13.54 \? 1.52 g/dl). DiaSpect proved to be the best technique (sensitivity 99.4%, specificity 94.4% and likelihood ratio 17.75). CuSO4 proved to be good with Negative Predictive Value close to 91.4%. NBM-200 shows wide variation but the mean of the difference being statistically not significant. Conclusion: CuSO4 method gives accurate results, if strict quality control is applied. HemoCue and DiaSpect are too expensive to be used as a primary screening method in an economically restricted country like India, but are accurate. NBM-200 is a non-invasive method and gives good result with better compliance and donor satisfaction.
Keywords: Blood donation, haematology cell analyser, DiaSpect, HemoCue, NBM-200, CuSO4
Full Text:
INTRODUCTION
Pre-donation haemoglobin (Hb) screening is vital for blood donor selection with the main intention of preventing blood collection from an anaemic donor and for protecting the health of potential blood donors. It is therefore essential, that there should be an accurate and reliable method for haemoglobin determination. According to the Indian Drugs and Cosmetics Act, 1940 for blood donation, the minimum acceptable haemoglobin (Hb) is 12.5 g/dl or haematocrit (Hct) of 38% for both males and females.[1] There are various methods of haemoglobin estimation which vary from simple CuSO4 method to measurement by photometer, each with its own advantages and limitations. The copper sulphate (CuSO4) specific gravity method[2] is the traditional method being used for donor screening at many blood centres. Though a cheap and easy method, it does not provide an acceptable degree of accuracy[3],[4]. In recent years, portable, point-of-care (POC) devices have become the standard to measuring Hb levels. This form of measurement is applied in settings such as blood banks due to quicker test results with smaller blood samples, typically from a capillary source at the fingertip. The HemoCue and DiaSpect test systems are portable, battery-operated photometric device for rapid determination of haemoglobin[6]. Both tests involve digital needle puncture to obtain samples, leading to blood donor discomfort and complaints. Recently, a new method to determine Hb levels has been developed, using the principle of occlusion spectroscopy[8] which exempts the donor from finger prick and makes the procedure more comfortable. This could therefore contribute to greater donor retention. The aim of this study was to analyse the feasibility of the use of this new non-invasive method. We also compared results of routinely used invasive haemoglobinometer with that of automated blood analyser (reference).
MATERIAL AND METHODS
This prospective study was conducted on 200 consecutive blood donors attending routine donor sessions at a tertiary care hospital based blood centre in Ahmedabad, Gujarat. Informed consent was obtained explaining the need of a venous blood sample and also the application of the device on their finger to perform the Hb measurements using the new method. The non-invasive Hb determination was performed using a NBM-200 (Orsense Ltd., Nez Ziona, Israel), based on occlusion spectroscopy. Briefly, a pressure is applied by a ring-shaped multi wavelength sensor probe containing a pneumatic cuff that temporarily occludes the blood flow in the base of the finger and generates a strong optical signal, yielding a high signal-tonoise ratio that is wholly blood specific. Analysis of the signal in the wavelength range of 600 to 1500 nm provides the necessary sensitivity for measuring Hb concentration and pulse rate. The test is performed in 90 seconds, according to manufacturer’s instructions. Two ml of venous blood sample in dipotassium EDTA under identical conditions were drawn from apparently healthy donors. Samples were analyzed using four different methods of Hb estimation: Automated haematology cell analyzer (Sysmex KX 21, Sysmex America, Inc. Lincolnshire), CuSO4 specific gravity method, Hemocue (Hemocue B - haemoglobin photometer; Angelholm, Sweden), DiaSpect T system (DiaSpect Medical AB Uppsala, Sweden). Testing on CuSO4, Diaspect and HemoCue was done without delay while samples were run on the automated cell analyser (reference haemoglobin value) immediately or within 30-60 minutes of collection. To avoid inter-observer variability, blood sampling and analysis of Hb was performed by a single trained operator. The working CuSO4 solution was prepared (specific gravity 1.053) and standardized every day using standard operating procedure (SOP). Quality control and calibration of automated haematology analyser was done as per SOP using manufacturer provided stabilized control reagents. Results of CuSO4 were interpreted as “pass” or “fail” at Hb cut-off of ≥ 12.5 g/dl. Statistical Analysis Statistical analysis was performed using SPSS 12.0 for Windows (Microsoft, Seattle, WA, USA). Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of each method was calculated and results were compared with automated cell analyser (gold standard).
RESULTS
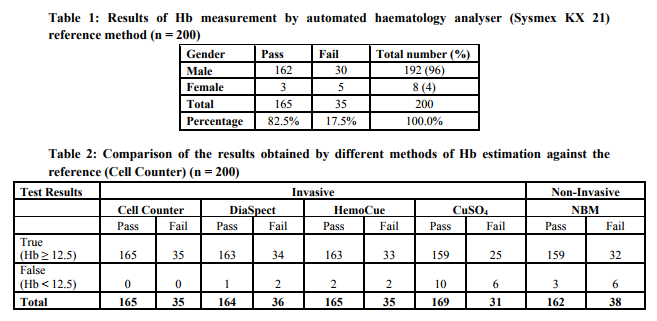
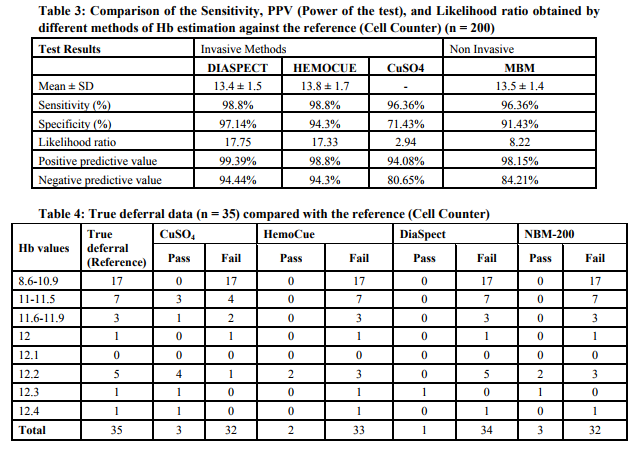
The gender distribution of 200 donor population predominantly consisted of males with only 4% female representation [Table 1]. A total of 35 (17.5%) donors were deferred due to low Hb. A comparison of different methods used in the present study against the reference haematology analyzer is summarized in [Table 2]. We assessed the Hb values (mean ± standard deviation) for 200 venous samples tested with each method. Hb values by HemoCue and Diaspect showed quite similar results against the reference. However, mean Hb value of HemoCue (13.8 ± 1.7 g/dl) was higher by 0.26 when compared with reference (13.54 ± 1.53 g/dl). The mean Hb values for NBM were 13.5 ± 1.4 g/dl. DiaSpect was found to be most accurate technique (sensitivity 98.8%; specificity 97.14%). CuSO4 also gave good results with overall 8% (16/200) false results, sensitivity of 96.36%, but specificity of 71.43%, PPV of 94.08% and NPV of 80.65% [Table 3]. The CuSO4 screening test inappropriately passed 5% (10/200) donors. Out of these, 6 donors had Hb values between 12.4-12.0 g/dl when tested by reference method [Table 4]. The results by NBM shows wide variation when compared to reference but the mean of the difference is not significant (P > 0.05). NBM (non-invasive) also gave good results with overall 4.5% (9/200) false results with sensitivity of 97.6%, specificity of 88.2%.
DISCUSSION
For blood collection an appropriate Hb screening method should be available so as to accept as many suitable donors as possible and to prevent any inappropriate deferrals. Any new method to be introduced for Hb screening should save time and expenditure and should be validated against ICSH standards.[5][7] It is true the capillary method, unlike venous sampling method of Hb estimation in field conditions for DiaSpect/CuSO4/HemoCue is more practical. But, as our reference method was based on venous samples, to maintain homogeneity and to have near true values only venous samples were used in this study. Additionally, donor acceptance policies are based on venous Hb standards and not on capillary Hb values. To avoid multiple sampling we used only single venous sampling in our study. In our study CuSO4 method inappropriately passed 5% of prospective donors, of which a majority (70%) were within 1.0 g/dl of threshold against the reference values. This finding was quite similar to the observations made by James et al.[9] Similarly Boulton et al. observed more inappropriate passes by CuSO4 method with inappropriate passes being within 1.0 g/dl of the threshold for their gender.[10] CuSO4 has been a traditional way of donor Hb screening despite its limitations. To ensure correct results, CuSO4 solution of accurate specific gravity should be used besides taking other technical precautions. Each drop of blood added to the solution affects the specific gravity, therefore changing the solution daily or at least after 25 tests has been recommended.[12] The CuSO4 method has also been found to give inappropriate deferral and significant number of such deferred donors could be recovered by using an alternative screening method. [13] Using a secondary method of screening, many donors could be retained that would otherwise be inappropriately deferred. We found CuSO4 inappropriately deferred 3% (06/200) of the prospective donors in comparison to 1% (02/200) of inappropriate deferral by using HemoCue. HemoCue is an easy, rapid and reliable method of donor screening.[14] However its use adds extra expense in a donor screening program if implemented as a primary Hb screening method.[7] The DiaSpect system compared well with established methods of blood donor screening, producing similar readings as the reference analyser, with highest sensitivity, specificity and likelihood ratio. NBM is precise than the routine accepted CuSO4 in use, preventing donation by anaemic donor (1.5% inappropriately passed). On the other hand, this could lead to unnecessary donor deferral (3% false deferral). Being non-invasive it exempts donor from finger prick and does not involve biohazard material handling.
CONCLUSION
DiaSpect is the best method for donor screening. HemoCue is a good method with high accuracy.NBM-200 seems to be a good method in terms of precision and feasibility for anaemia screening of blood donors as well as being much more comfortable for donors. CuSO4 method is cheap and gives accurate results, if strict quality control is applied. This method can be retained as the primary screening method; however, to save inappropriate deferrals, subsequent testing can be done with more precise method (i.e, HemoCue / DiaSpect / NBM).
References:
1. The Drugs and Cosmetics Act, 1940 and the Drugs and Cosmetics Rules 1945, Amendment upto 30th September, 1999.
2. Philipps RA, VanSlyke DD, Hamilton PB, Dole VP. Measurement of specific gravities of whole blood and plasma by standard copper sulphate solutions. J Biol Chem 1950;183:305-30.
3. Ross DG, Gilfillan AC, Houston DE, Heaton WA. Evaluation of haemoglobin screening methods in prospective blood donors. Vox Sang 1986;50:78-80.
4. Radtke H, Polat G, Kalus U, Salama A, Kiesewetter H. Haemoglobin screening in prospective blood donors: Comparison of different blood samples and different quantitative methods. Transfus Apher Sci 2005;33:31-5.
5. Zwart A, van Assendelft OW, Bull BS, England JM, Lewis SM, Zijlstra WG. ICSH Recommendations for reference method for haemoglobinometry in human blood (ICSH standards 1995) and specifications for international haemoglobincyanamyde standard. J Clin Pathol 1996;49:271-4.
6. Dacie JV, Lewis SM. Practical Haematology. 9 th ed. Edinburgh: Churchill Livingstone; 2001. p. 23.
7. Tondon R, Verma A, Pandey P, Chaudhary R. Quality evaluation of four hemoglobin screening methods in a blood donor setting along with their comparative cost analysis in an Indian scenario. Asian J Transfus Sci 2009;3:66-9
8. Weinstein A, Herzenstein O, Gabis E, Korenberg A. Screening of anemia using noninvasive occlusion spectroscopy sensor. Transfusion 2010;50:91a-2a.
9. James V, Jones KF, Turner EM, Sokol RJ. Statistical analysis of inappropriate results from current Hb screening methods for blood donors. Transfusion 2003;43:400-4.
10. Boulton FE, Nightingale MJ, Reynolds W. Improved strategy for screening prospective blood donors for anemia. Transfusion Med 1994;4:221-5.
11. Timan IS, Tatsumi N, Aulia D, Wangsasaputra E. Comparison of haemoglobinometry by WHO Haemoglobin colour scale and copper sulphate against haemoglobincyanide reference method. Clin Lab Haematol 2004;26:253-8.
12. Brecher MG, leger RM, Linden JV, Roseff SD. Blood collection, storage and component preparation. Technical manual. 15thed. Maryland: American Association of Blood Banks (AABB); 2005. p. 799-800.
13. Cable RG. Haemoglobin determination in blood donors. Transfusion Med Rev1995;9:131-44.
14. von Schenck H, Falkensson M, Lundberg B. Evaluation of HemoCue: A new device for determining haemoglobin. Clin Chem 1986;32:526-9.
15. Paddle JJ. Evaluation of the Haemoglobin colour Scale and comparison with the HemoCue haemoglobin assay. Bull World Health Organ 2002;80:813-6.
16. Lewis SM and Emmanuel J. Validity of the haemoglobin colour scale in blood donor screening. Vox Sanguinis 2001;80;28-53.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





