IJCRR - 6(4), February, 2014
Pages: 21-25
Date of Publication: 20-Feb-2014
Print Article
Download XML Download PDF
PLACENTA PRAEVIA: CORRELATION WITH CAESAREAN SECTIONS, MULTIPARITY AND SMOKING
Author: Madulika Sharma, Jaya Choudhary
Category: Healthcare
Abstract:Objective: This study is planned to assess the various risk factors of placenta previa such as with multi-parity, previous caesarean section and smoking. Methodology: This study conducted at the department of obstetrics and gynaecology, J.L.N.Medicalcollege, Ajmer from Oct 2009 to September 201. Detailed obstetrical and surgical history were documented. All those attending antenatal clinic in third trimester of pregnancy, 32 weeks onwards with or without symptoms of placenta previa and showing placental implantation in lower uterine segment and In the obstetric ward all the patients presented in emergency (unbooked) with antepartum haemorrhage and diagnosed as case of placenta previa by Ultrasound examination, were documented. Statistical analysis was performed using the Vasserstats software, Chi square test; Risk ratio and Percentage of incidence were used to show association of risk factors with PP, where appropriate. Results: Out of total admissions, 4000 patients at random were taken for the study.150 patients were diagnosed as placenta previa of various degrees. Out of the 150 PP patients, 72 were multipara, 65 were grand multipara and rest were primigrvida.400 patients had previous history of one or more caesarean section.85 patients are those who smoked, having placenta previa. Conclusion: The data of this study is concluded that there is a good association between increasing incidence of placenta previa with the increase in parity (p< 0.001), c-sections (p< 0.001), and smoking (p< 0.0001, RR=4.5, CI: 95).
Keywords: Placenta previa, Caesarean section, smoking.
Full Text:
INTRODUCTION
When placenta is attached in lower uterine segment called as placenta praevia.(1) In general It take place in the second or third trimester but sometimes it can observed in the later part of the first trimester. It is an important obstretic complication which can cause of antepartum haemorrhage (vaginal bleeding). It involve about 0.4-0.5% of all labours.(2) Traditionally four types of placenta previa recognised.(2, 3, 4) 1. Total placenta previa: internal cervical os is completely covered with placenta. 2. Partial placenta previa: internal cervical os partially covered with placenta previa. 3. Marginal placenta previa: edge of placenta does nat cover but lie in close proximity to the internal cervical os. 4. Low lying placenta: edge is not near os, but can be palpated by examining finger introduced through the os, generally 2 cms from os. Placenta previa currently, can be classified on the basis of usg findings as (5) Group 1: Placental edge reached or overlapping internal os.
Group 2: Placental edge was from 0.1 to 2cms from internal os. Group 3: Placental edge was more than 2cms from internal os. The overall incidence is 1/200 births, and 1/1,000 are grade IV with placenta over the entire cervix. (6) The overall prevalence of placenta praevia was 5.2 per 1000 pregnancies (95% CI: 4.5–5.9). However, there was evidence of regional variation (P = 0.0001); prevalence was highest among Asian studies (12.2 per 1000 pregnancies). The prevalence of major placenta praevia was 4.3 per 1000 pregnancies (95% CI: 3.3–5.4).(7) Surgical disruption of uterine cavity is a potential risk factor for placenta previa.(8) Cesarean delivery is the most common operative procedure in practice of OBG,which is known to cause lasting damage to myometrium and endometrium,and thus increases the incidence of PP.(9) In United States, Placenta previa occurs in 0.3-0.5% of all pregnancies. The risks increase 1.5- to 5-fold with a history of caesarean delivery. (10) In India, according to P. M. Singh, A. N. Gupta, C. Rodrigues, overall incidence of placenta previa 1.9 per cent but the incidence in cases with previous cesarean section (C.S.) was found to be 3.9 per cent. (p <0.01) (11) One study showed that previous caesarean sections increased risk of developing placenta previa from 2.2 to 22.4 times.(12) Multiparity is also an important risk factor for previa with RR of 1.18 (13) The risk of having placenta previa increases with increasing parity (14) The incidence of placenta previa was 2.4% among smokers women, which is an eight times more compared with the incidence of a placenta previa among all births. So, maternal smoking appeared as an independent risk factor for placenta previa. (15) Shown in one more study, with smoking, the relative risk for placenta previa was 1.36 (95% Cl 1.04-1.79). (16) Placenta praevia is associated with Severe bleeding, which further results in severe maternal morbidity and sometimes mortality. In developing countries a few women attend antenatal care, operative delivery are late because of logistical problems. The causative risk factors for severe haemorrhage during delivery with placenta previa are not well analysed. The major objective of this study so was to identify the risk factors for parturients with placenta praevia to reduce the maternal morbidity and mortality associated with this condition.
MATERIAL AND METHODS
This descriptive non interventional study was conducted at the department of obstetrics and gynaecology, Rajkiya Mahila chikitsalaya, J.L.N. Medical College, Ajmer from October 2009 to September 2011. Detailed obstetrical and surgical history was documented. All those attending antenatal clinic in third trimester of pregnancy, 32 weeks onwards with or without symptoms of placenta previa and showing placental implantation in lower uterine segment and In the obstetric ward all the patients presented in emergency (unbooked) with antepartum haemorrhage and diagnosed as case of placenta previa by Ultrasound examination, were documented. After completion of two years of specified time period, collected information was analysed. Information on cigarette smoking was collected both at the first prenatal visit and at the time of admission to the hospital for delivery. Women were asked whether they had ever smoked during the current pregnancy and, if they were smokers, the number of cigarettes smoked per day. Changes in smoking behavior during the course of pregnancy were not recorded Two methods were used to analysis smoking relationship with placenta previa. First, smoking was categorized as a dichotomous variable (yes/no). Second, to evaluate the effect of dose of smoking in terms of number of cigarette smoked per day as the risk for causing placenta previa. For this assessment, number of cigarettes smoked daily was grouped as none, 1-5, 6-10, 11-15,≥16.
Statistical analysis was performed using the Vasserstats software; Chi square test, risk ratios, and percentage of incidences were used to show association of risk factors with PP, where appropriate.
RESULTS
Out of total admissions during the specified time period, 4000 patients were taken for the study.150 patients were diagnosed as placenta previa of various degrees. They were analysed, and percentage of incidence, RR were calculated out to examine the relationship between Parity, prevoius c-sections and smoking.
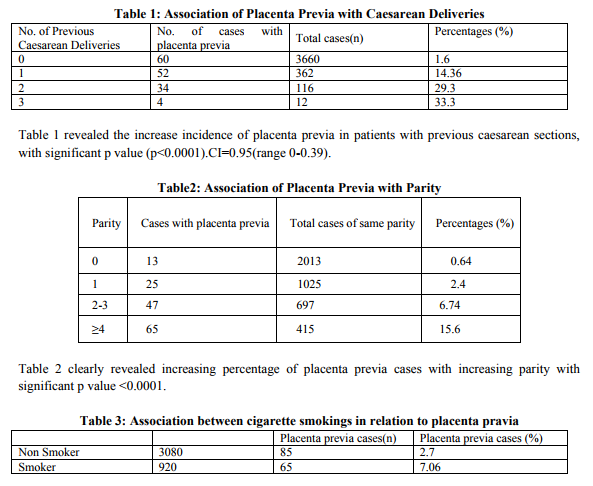
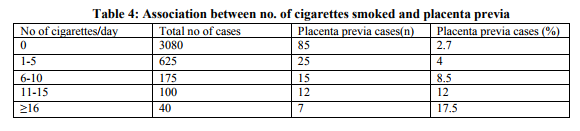
Table 3 showed ,with smoking ,there is increased risk of having placenta previa as compared to non smokers women with Risk Ratio (RR)=4.3.CI=0.95(3.19-5.9) and significant p value <0.001. The overall prevalence of smoking during pregnancy was 23 percent. Cigarette smoking was associated with a fourfold increase in the risk of placental abruption (relative risk (RR) = 4.5, 95 percent confidence interval (CI) =3.19-5.9), with gradient of increasing incidence of placenta previa with increasing number of cigarettes smoked per day with significant p value≤0.001. (Table 4)
DISCUSSION
No. of studies have been conducted earlier to examine the association of placenta previa with caesarean section but most of them failed to quantify the increased risk associated. For instance,Clark et al showed that in women with one uterine incision,the risk of placenta previa was 0.26% compared with 10%in women with four or more.but this study didn’t take into account other risk factors like parity.(17) Mc Mohan et al attempted to account for risk factors like age, parity, and race but did not examine the role of multiple c-sections. In this study, we evaluated the association between one csection and successive placenta previa. (18) We also demonstrated that possibility of PP increases with greater parity independent of no of prior caesarean deliveries.One caesarean delivery does not significantly increases the possibility of PP in primiparous, however subsequent deliveries, whether c-section or vaginal, particularly caesarean deliveries increases the possibility of future PP. Our study corroborates and strengthens earlier findings on the positive association between smoking and placenta previa. With odds ratios ranging from 1.3 to 2.6 in previous studies, while we observed a relative risk of 4.3.Several potential mechanisms relating cigarette smoking during pregnancy to the development placenta previa have been proposed. Some morphological changes in the placentas of smokers are described such as large surface area of placentas, with increased size, and to have lesion typical area of uterus showing under perfuse lesion. (19) While Spira et al.observed an increased frequency of hypoxia among smokers compared with nonsmokers. (20) Suzuki et al. speculated that smoking may be a reason for pathological changes in endothelial cell of placenta which further consequence in rigidity of the arteriolar walls and vasoconstriction. (21)
CONCLUSION
From the present study and available data it is concluded that there is a direct association between incidence of placenta previa with the increase in parity, previous caesarean section and smoking. Any women with pervious history of caesarean section, multiparity and smoking have high risk for placenta previa. In such case they should counselled and made aware about symptom and complication of placenta previa. Early detection of placenta previa with ultrasound and monitoring during pregnancy can lower the risk and proper management of sudden bleeding which further reduces perinatal morbidity and mortality due to placental abruption.
References:
1. AbramowiczJS,SchienerE.inutero imaging of placenta;importance for diseases of pregnancy.Placenta 2007 ;28 (Suppl.A):S14- 22.
2. Bhide A,ThilaganathanB,Recent advances in the management of placenta previa. Curr Opin Obstet Gynaecol 2004;16:447-51
3. Oyelese KO,Smulian JC. Placenta previa,placenta accrete,and vasa previa. Obstet Gynecol 2006;107:927-41. 4. Timor-Tritsch IE,MONteagudoA, Diagnosis of placenta previa by transvaginal sonography. Ann med 1993;25:279-83
5. Amarnath Bhide, Federico Prefumo, Jessica Moore, Brian Hollis, Basky Thilaganathan: Placental edge to internal os distance in the late third trimester and mode of delivery in placenta praevia.BJOG: an International Journal of Obstetrics and GynaecologySeptember 2003, Vol. 110, pp. 860–864.
6. Neilson JP; Interventions for suspected placenta praevia. Cochrane Database Syst Rev. 2003;(2):CD001998.
7. Jenny A. Cresswell, CarineRonsmans,Clara Calvert, Véronique Filippi;Tropical Medicine and International Health;Volume 18, Issue 6, pages 712–724, June 2013.
8. BarettJM,BoehmFH,KillamAP;induced abortion, a risk factor for placenta previa;AmJ Obstet Gynecol 1981;141:769-72.
9. Morris H. Surgical pathology of the lower uterine segment caesarean section scar: is the scar a source of clinical symptoms? Int J GynecolPathol 1995;14:16-20.
10. US Census Bureau, Population Estimates, 2004.
11. P. M. Singh M.D.,C. Rodrigues , A. N. Gupta, Placenta previa and previous cesarean section. Acta Obstetricia et GynecologicaScandinavica;2011;60(4):367– 368. Article first published online:2011
12. Marianne S. Hendricks;Y. H. Chow;B. Bhagavat;Dr. Kuldip Singh; Previous Cesarean Section and Abortion as Risk Factors for Developing Placenta PreviaJournal of Obstetrics and Gynaecology Research, 1999;25:2,137–142.
13. Yoshio Matsuda, Kunihiko Hayashi ,Arihiro Shiozaki, Yayoi Kawamichi, Shoji Satoh, Shigeru Saito ; Comparison of risk factors for placental abruption and placenta previa: Casecohort study.Journal of Obstetrics and Gynaecology Research.2011;37(6):538–546.
14. Abu Hijja AT,EI Jallad,ZiadehS, Placenta previa, effect of age, gravidity, parity, and previous c-sections.Gynecol ObstetInvestb1999;47:6-8.
15. G. Monica, C. Lilja: Placenta previa, maternal smoking and recurrence risk. Acta Obstetricia et GynecologicaScandinavica,1995;74(5):341– 345.
16. Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and metaanalysis of observational studies. J Matern Fetal Neonatal Med 2003;13:175-90.
17. Clark SL, Koonings PP, Phelan JP. Placenta previa / accrete and prior cesarean section. Obstet Gynecol 1985;66:89-92.
18. Mc Mohan McMahon MJ, Rongling L, Schenck AP, Olshan AF, Royce RA. Previous caesarean birth, a risk factor for placenta previa? J Reprod Med 1997;7:409-12.
19. Christianson RE. Gross differences observed in the placentas of smokers and nonsmokers. Am J Epidemiol 1979; 110:178 87.
20. Spira A, Philippe E, Spira N, et al. Smoking during pregnancy and placental pathology. Biomedicine 1977;27:266-70
21. Suzuki K, Minei LJ, Johnson EE. Effect of nicotine upon uterine blood flow in the pregnant rhesus monkey. Am J Obstet Gynecol 198O;136:1OO9-13
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





