IJCRR - 6(5), March, 2014
Pages: 48-58
Print Article
Download XML Download PDF
HISTOPATHOLOGICAL REVIEW OF SPLEEN SPECIMENS (200 CASES)
Author: Shah S., Gosai R., Gonsai R. N.
Category: Healthcare
Abstract:This is a descriptive / retrospective crosssectional study. This study was carried out at the histopathology laboratory, Department of Pathology, B. J. Medical College, Ahmedabad from January 2008 to December 2009 on all splenecand tomy specimens and one splenculi biopsy. Total 200 cases were studied which were received already fixed in 10% neutral buffer formalin. Among the specimens the most common age group fell in 21-30 years (30%). Male to female sex ratio was1:1.1. In 30% cases cause of splenomegaly was not identified. Most common known cause for splenomegaly was portal hypertension (23.5%) followed by trauma (12.5%). Most common diagnosis made after microscopy and correlating clinical and radiological findings was fibrocongestive splenomegaly (67%), which was most commonly due to hepatic cause. Most common cause identified later in unidentified cases of splenomegaly was also fibrocongestive splenomegaly (69%).
Keywords: splenectomy specimens, splenculi biopsy
Full Text:
INTRODUCTION
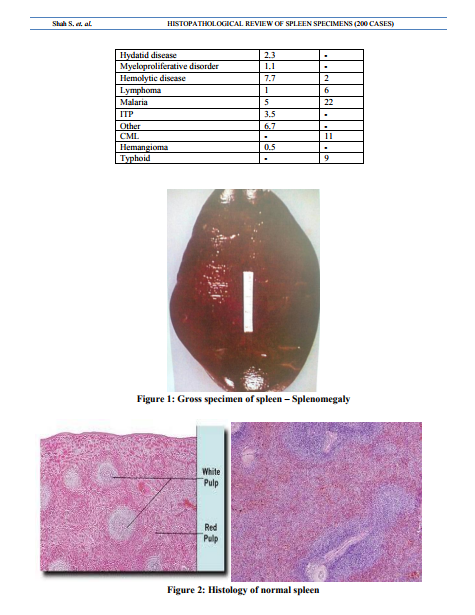
Spleen is mysterious organ, it can be troublesome specimen for surgical pathologist due to discordance between patient’s clinical condition and perceived findings. Patients with a dramatic clinical presentation that point to splenic pathology not infrequently have no discernable or have barely perceptible histological abnormalities of the spleen. Similarly, patients whose spleens contain histological findings that seem to deviate significantly from the “norm” may have no clinically detectable haematological complains.This review presents practical aspects of splenic histopathology specimens and relates this to the pathologist’s approach in evaluating the abnormal spleen and assists in resolving such discordance.Splenectomy dates back to1549 when first reported by Zacarello in Italy. In 1826 Quittenbaum did first elective splenectomy for portal hypertension and in 1866, Bryant did first splenectomy for leukemia. In 1892 emergency splenectomy was done for trauma in Germany. In 1911 and 1916 elective splenectomy was done for autoimmune haemolytic anemia and ITP respectively.6The spleen, in healthy adult human is approximately 11 cms4.3in length,usually weights 150 grams and lies beneath 9th to 12th thoracic rib and between fundus of stomach and diaphragm. It filters foreign matter including old / damaged blood cells : participates in immune response to blood borne antigens; major repository of mononuclear phagocytic cells in red pulp ,lymphoid cells in white pulp and platelets and produces new blood cells in infants / children or adults with severe anemia.Composed of red pulp(76-79%) and white pulp(5-20%) separated by marginal zone (diag 2) Massive splenomegaly ( Spleen > 1000 g) is due to CML, Gaucher’s disease, hairy cell leukemia, marginal zone B cell lymphoma,myelofibrosis,plasmacytoma,prolymph ocytic leukemia.Rupture is due to blunt trauma or abdominal surgery, causing haemoperitoneum and emergency splenectomy.spleen only rarely ruptures spontaneously (associated with infectious mononucleosis, malaria, Typhoid fever, leukemia / Lymphoma, other tumours,subacute bacterial endocarditis, peliosis lienis, acute splenitis, pregnancy) Gross rupture may be a very small capsular tear, often in superior pole or hilum Micro: neutrophil below capsular tear with intraparenchymal haemorrhage ; also lymphoid hyperplasia with prominent marginal zone. Splenectomy is usually performed for traumatic rupture.Usually no clinical consequence in adults. In children, it is associated with increased incidence and severity of infections, particularly encapsulated bacteria such as Streptococcus pneumonia, Neisseria meningitides, Haemophilus influenza; overwhelming infections may begin days to years after splenectomy, without an identifiable focus and have 50-80% mortality despite antibiotics. In children, splenectomy is avoided in favour of splenic repair, partial splenectomy is performed for haematological disorder. Howell-Jolly bodies are evidence of no splenic function.
OBJECTIVE: \
To study incidence of splenectomy in relation to different age ,sex, cause of splenomegaly and final diagnosis of splenectomised patients.\
MATERIALS AND METHODS\
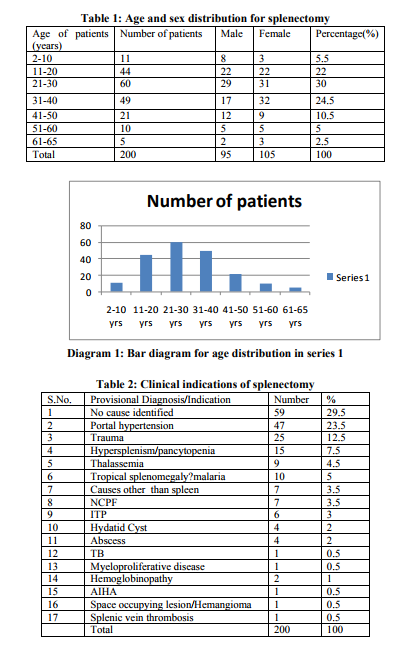
This is a retrospective study carried out in histopathology laboratory of department of pathology, B.J.Medical College, Ahmedabad from January 2008 to December 2009 comprising of 200 cases.The parameters like age, sex, cause of splenomegaly and splenectomy, macroscopic appearance of spleen, final diagnosis ofsplenectomized patients were studied. All specimens were complete splenectomy samples except one which was a splenculi biopsy specimen.the spleens were already fixed in 10% neutral buffer formalin. Detailed clinical histories.clinical examinations and investigations done on patients were noted like personal history,past history, family history, clinical examinations, CBC, serum chemistry,coagulation profile, X-Ray, USG. Indication of splenectomy was noted. Spleens were sectioned serially by blade loafing and re-fixedin 10% formalin saline for 24-48 hrs before sectioning and processing.Gross and microscopic findings were note were weight, size, gross and microscopic findings and finally the pathological diagnosis in respect of different pathologies. In addition to hematoxylin and eosin, stains such as Giemsa, Perl’s, Prussianblue, congo red and Periodic Acid Schiff were used when necessary. RESULTS Total 200 specimens of spleen were studied in histopathology department of BJ medical college, civil hospital, Ahmedabad in period of 2008 to 2009. Table 1 shows age and sex distribution of splenectomy and chart 1 shows bar diagram of age. The age range was 2 to 65 years. Highest incidence was in 21 – 30 yrs group which was 30%, next was 31-40 yrs in which was 24.5%. Incidence declined after 40 yrs and least number of cases were in 61-65 yr group. M:F ratio was almost equal except in 2-10 yr group in which it was 2.6:1 and 31-40 age ratio was 1:1.88
Macroscopic examination Table 3 shows dimentions of spleen specimens. Dimension of spleen were varying from normal size and weight to massively enlarged spleen >1000 gm and huge in size in reactive follicular hyperplasia hyperplasia , hemangioma of spleen and splenomegaly due to other reasons. Out of 25 traumatic cases, laceration was found in 9 cases. Hemorrhagic area was found in 5 cases.spleniculi was found in 5 cases (2.5%), 2 in thalassemia patients, one each in tropical splenomegly syndrome, ITP case and portal hypertension. Infarct like areas were noted in 30 spleens, one in sickle cell anemia patients and all other due to large size of spleen.
Histopathological Diagnosis
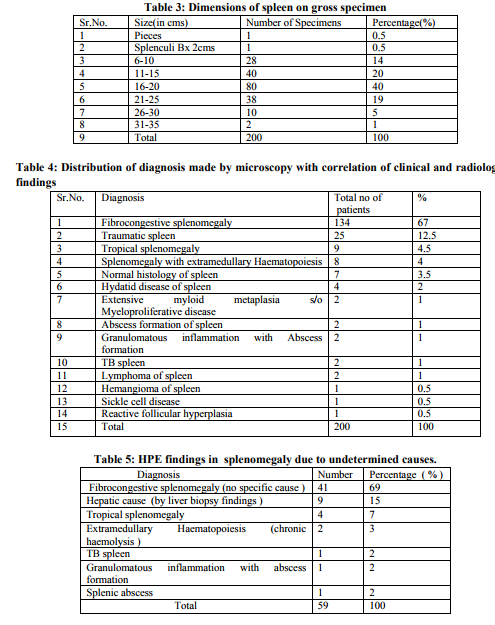
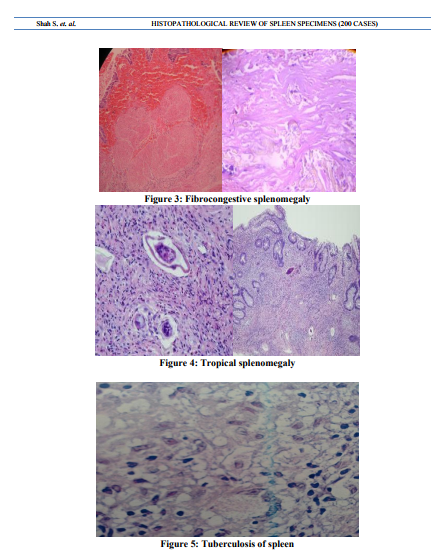
Table 4 shows distribution of various diagnoses made by microscopy and correlating clinical and radiological findings. Fibrocongestive splenomegaly was the most common diagnosis made by microscopy. It was most commonly found in splenomegaly due to hepatic cause .congestion of red pulp and fibrosis was noted. In traumatic spleen no specific findings was noted except hemorrhage and necrosis. 9 cases were diagnosed as tropical splenomegaly – multiple eosinophils, sinusoidal dilation but no fibrosis or hemosiderin deposition led to this diagnosis. Extramedullary haematopoiesis was present in 10 cases in which 2 were of extensive degree found out to be myelofibrosis. In others it was due to chronic haemolytic conditions .Special mention is for a case of multinodular hemangioma found in 23 yr female in which grossely detected tumour of 10 cm size was present.Microscopically markedly proliferating and anastomosing vascular channels lined by endothelial cells showing vague hemangiopericytoma like pattern.At places vascular channels showed evidence of lobular pattern surrounded by hyalinised stroma. Two cases of solitary splenic lymphoma were found in 47 and 60 year males presented with provisional diagnosis of splenic abscess. Grossely multiple whitish nodule was present. Microscopically proliferation of white pulp was noted. There was formation of multiple nodules consisting of monomorphic small lymphocyte like cells having hyperchromatic vesicular nucleus and prominent nucleoli. Diagnosis of NHL of spleen – small lymphocytic variant was made which was confirmed on IHC. Two cases of TB were found having caseous inflammation and two of granulomatous inflammation with abscess formation. One case of reactive follicular hyperplasia was found.
Histopathology in undetermined causes of splenomegaly
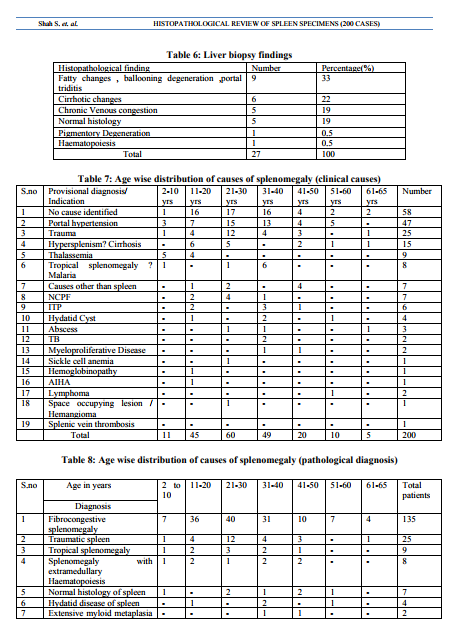
splenomegaly Table 5 shows findings in splenomegaly due to undetermined causes. Out of 59 cases in which no cause was determined clinically or radiologically, in 69 % cases diagnosis of fibrocongestive splenomegaly was given.Hepatic causes were found out in 15 % cases by liver biopsy. In 7 % cases diagnosis of Tropical splenomegaly was given. Liver biopsy was done with splenectomy in 27 cases out of 200 (13.5%) Table 6 shows various liver biopsy findings.Cirrhotic changes were present in 2% of cases. Chronic venous congestion was found in 19% cases. 9 biopsies (33.3 %) gave final diagnosis as hepatic cause of splenomegaly, which is a significant finding.
DISCUSSION
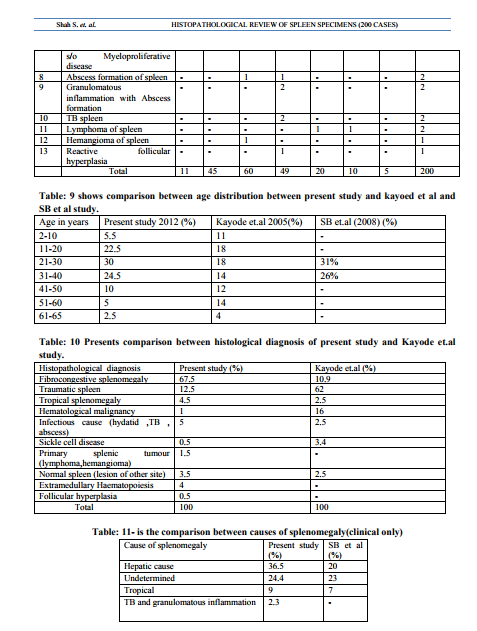
There are very few studies based on Histopathological findings in spleen..This study is a novel study as it involves 200 cases and focussed on histopathological correlation of clinical findings.It revealed cause of splenomegaly in 31 % cases in which no diagnosis was made clinically which is quite significant. A hospital based study of splenomegaly with special reference to the group of indeterminate origin was done in March 2008 by Sundaresan JB, Dutta TK, and et. Al.1 at Department of Medicine, JIPMER, Pondicherry. But it was a clinical study.The common causes of splenomegaly in this study were malaria (22%), chronic myloid leukemia (11%), NCPF(9%), enteric fever (9%), cirrhosis of liver (8%) and HMS (7%). This is significantly different from the observations in previous studies 2,3 on splenomegaly from india. Malaria was observed in 3 patients (4%) only. In 32 patients (42.7%) the cause of splenomegaly could not be determined. In the study of Chandra et al (4) the common cause found were again cirrhosis of liver and chronic myloid leukemia. Idiopathic splenomegaly was found in 15 patients (18.1%) Histopathological study and audit of the spleen in Nigerians was done by Kayode et.al5 during the period of 18 yrs between 1988 and 2005. Only 123 specimens of spleen were received. 119 had adequate data to be included in this study. There were 76 males and 43 females. The age range was 1 yr to 86 yrs. The highest number of splenectomy was in the age group 11-20 (16 male, 6 females). The incidence declined after age of 60. Table 7 shows age wise distribution of various causes of splenomegaly (clinical causes) Thalassemia was most common cause of splenectomy in 2-10 year age group. Portal hypertension and Trauma being the leading cause of splenectomy in 21-30 yr age groupTropical splenomegaly was found out to be most common in 31-40 yr age group. ITP being most common in 31-40 yr age group and male female ratio was 1:5. Lymphoma is common in old age as expected.In present study most common cause of splenomegaly as well as indication of splenectomy comes out to be hepatic.Portal Hypertension is very common in Gujarat, Rajasthan, Maharashtra and M.P. which forms our main patient group. Malaria is common but splenomegaly is rarely needed as diagnosis is earlier and antimalarial are given. Haematological malignancies like CML, is not included our study as most malignancies are referred to Gujarat Cancer Research Institute(GCRI) which is not part of this study . In SB et.al (1) study only causes of splenomegaly are enumerated. It is not based on splenectomy specimens .Trauma is not included in this study.However if we exclude trauma and splenectomy due to other reasons then out of 168 splenectomy cases, as Table 11 showscomparison between present and SB et al study for causes of splenomegaly(clinical only): hepatic cause are the predominant one.Almost 25% cases remain undetermined and no specific cause is identified. Infectious diseases like TB, Hydatid disease, Typhoid are common but typhoid rarely needs splenectomy but it is not present in SB et al study. Hemangioma is most common primary tumour of spleen and it is included in our study
SUMMARY
For the pathologist in training and attending alike, the spleen can be deceptively simple. It is rare as a surgical specimen and when it is encountered ,it seldom contains an abnormality. however occasionally the spleen’s troublingly complex nature is unmasked whenfindings do not correspond to a well definded category of disease of disease or the splenic parenchyma obscures diagnostic features. In our study due to large number of cases the results are fairly significant. Hepatic disease remains the top of all. Trauma is also common indication for splenectomy. Primary splenic tumours like hemangioma are rare but can be encountered. Lymphoma can also be underdiagnosed as reactive so pathologists should be alert. Hydatid disease, TB, Abscess formation are also not very uncommon. Inevitably ,it is these cases in which there is often great clinical pressure and the temptation may be great to force the findings into an existing category of node based or soft tissue based nosology. The key to timely and accurate diagnosis in such situations lays in preparations: obtaining complete clinical information about the patient, taking a systematic approach to prosection, preparing thin sections from well fixed tissue and becoming familiar with the stains and studies that define the intactness of splenic immunoarchitecture.
References:
REFERENCES
1. Bates I , Bedu-Addo G.Review of diagnostic criteria of hyper reactive malarial splenomegaly. Lancet.Apr 19 1997; 349(9059):1178.
2. AhmanDL, Cancer 1966,19 :461-69
3. Madeleine D. Kraus , MD Seminars in Diagnostic Pathology , vol 20 , no 2 (May),2003 : pp 84-93
4. Aranha GV , J Surg O ncol 1976, 8 :481-487
5. Weichselbaum.A. Beitrige zur Geschwulstlehre . Virchows Arch . f . path . Anat., i88i , 85,554-567.
6. Smith,C.E., and Rusk , G. Y. Endothelioma of spleen. A study of 2 cases,with review of the literature of primary malignancy of the spleen. Arch. Surg.,1923 ,7 ,371-414.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





