IJCRR - 6(5), March, 2014
Pages: 43-47
Print Article
Download XML Download PDF
COMPARISON OF BRONCHOALVEOLAR LAVAGE CYTOLOGY AND BIOPSY IN LUNG MALIGNANCY
Author: Richa Sharma, Hemina Desai, Pankaj Malukani, R.N.Gonsai, H.M.Goswami
Category: Healthcare
Abstract:Background : Respiratory tract cytology is well established throughout the world as a vital diagnostic procedure in the evaluation of any patient with suspected lung malignancy and with the introduction of Flexible Fiberoptic Bronchoscopy, Bronchoalveolar Lavage is a popularly accepted tool for diagnosing lung cancer. Aims and Objestives : 1) To determine the efficacy of BAL cytological technique in diagnosing carcinoma of lung and correlating them with histopathological diagnosis by Bronchial Biopsy 2) To study the variation in the results with regards to different morphological types of lung malignancies. Material And Methods : A retrospective study was conducted at our tertiary care hospital. We selected 100 cases where bonchoalveolar lavage cytology samples as well as Bronchial Biopsy were taken. Samples were processed and reported as per the standard methods. Histopathological diagnosis by Bronchial Biopsy was considered as the \"Gold Standard.\" The samples were obtained by Flexible Fiber-optic Bronchoscopy done by the clinician. Result : Sensitivity of BAL was 42% and Specificity was 89.6%. Positive Predictive Value (86%) and Negative Predictive Value (48%), False Negative Index (60%) and False Positive Index (11%) were also calculated. Accuracy was 59%. Morphologically,44% were classified as poorly differentiated carcinoma, 28% were adenocarcinoma, 16% were squamous cell carcinoma and 12% were small cell carcinoma on BAL cytology. While on Bronchial Biopsy 29% were poorly differentiated carcinomas, 21% were adenocarcinoma,15% were squamous cell carcinoma and 15% were small cell carcinoma. Conclusion: Bronchoalveolar Lavage cytology is a good screening method for diagnosing lung malignancy as it is fairly sensitive and specific when compared with Bronchial Biopsy which is the \"Gold Standard\" method.
Keywords: BAL (Bronchoalveolar Lavage), Bronchial Biopsy, Lung cancer.
Full Text:
INTRODUCTION
Respiratory tract cytology is well established throughout the world as a vital diagnostic procedure in the evaluation of any patient with suspected lung malignancy1,2 . Flexible Fiberoptic Bronchoscopy with its extended visual range, excellent patient?s acceptance, low complication rate, and high diagnostic yield, provides a safe and effective means for making the diagnosis2 and sampling of suspected areas for cytology. Broncho-alveolar lavage (BAL) was originally developed as a therapeutic tool for pulmonary conditions like pulmonary alveolar proteinosis, cystic fibrosis and intractable asthma. Bleeding is always a concern when an airway lesion is biopsied. Pneumothorax occurs in 1-10% of cases of transbronchial biopsies (TBB). Bronchoalveolar lavage cytology is a minimally invasive method and has no absolute contraindications beyond those commonly associated with bronchoscopy. Application of BAL to the diagnosis of pulmonary malignancy was first reported in the early and mid-1980s and has since gained acceptance and steady popularity as a tool for diagnosing lung cancer.1,3,10-16 In this study our objective was to determine the efficacy of BAL cytological technique in diagnosing carcinoma of lung by correlating them with histopathological diagnosis by Bronchial Biopsy. We also aim to study the variation in the results with regards to different morphological types of lung malignancies.
MATERIAL AND METHODS
A retrospective study was conducted at our tertiary care hospital. We selected 100 cases where both Bonchoalveolar Lavage cytology as well as Bronchial Biopsy samples were taken. BAL cytology samples were obtained by Flexible Fiberoptic Bronchoscopy by the clinician. Smears were prepared after centrifugation and were stained as per routine protocol.4 Biopsy samples were processed by routine paraffin method followed by Hematoxylin and Eosin stain.5 For reporting, WHO Classification System was followed.6 Histopathological diagnosis by Bronchial Biopsy was considered as the “Gold Standard.”
RESULTS
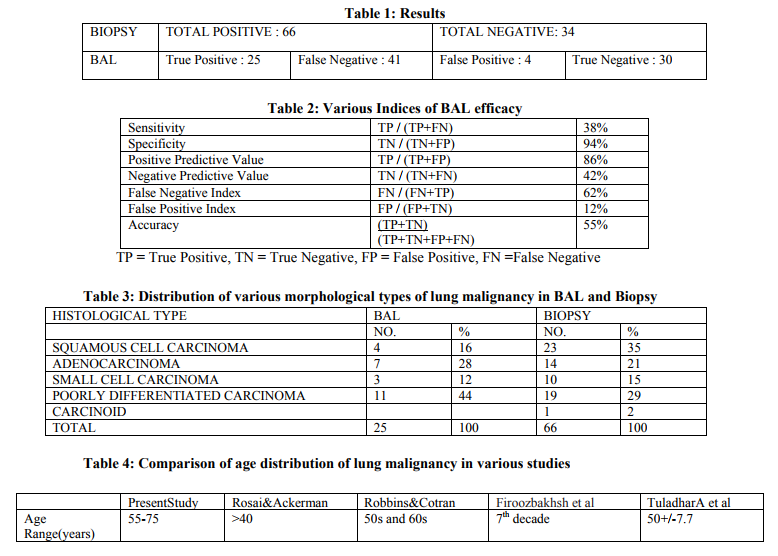
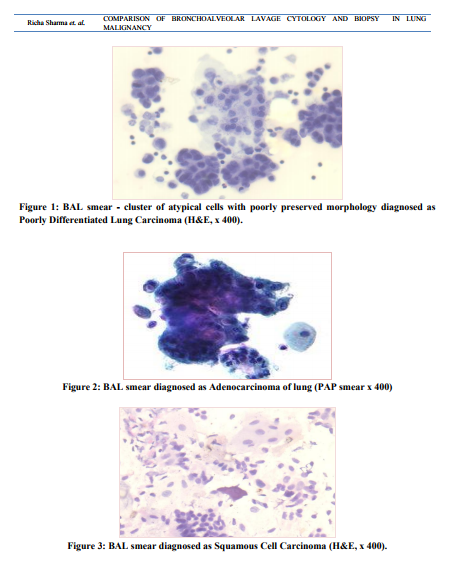
All the patients who were diagnosed with lung malignancy were in the age group of 55 to 75 years and most of them were males. Out of 100 cases, 66 were diagnosed by Bronchial Biopsy as lung cancer. Rest of the cases showed non specific inflammatory or tuberculous lesions or no significant pathology. BAL cytology showed 25 True Positive cases and 34 True Negative cases, as confirmed by Biopsy. 4 cases were diagnosed as False Positive and 37 cases as False Negative by BAL. (Table 1). Thus, Sensitivity of BAL was 42%. And Specificity was 89.6%.Similarly Positive Predictive Value (86%) and Negative Predictive Value (48%), False Negative Index (60%) and False Positive Index (11%) of BAL were calculated. Accuracy of BAL was 59%. (Table 2). Out of 25 True Positive cases diagnosed by BAL, 11 (44%) were classified as Poorly Differentiated Carcinoma (Figure 1), 7(28%) were Adenocarcinoma(Figure 2), 4 (16%) were Squamous Cell Carcinoma(Figure 3) and 3 (12%) were Small Cell Carcinoma. While only 19 (29%) cases out of 66 positive Bronchial Biopsies, were labelled as Poorly Differentiated Carcinomas, 14 (21%) were Adenocarcinoma, 10 (15%) were Squamous Cell Carcinoma and 3 (15%) were Small Cell Carcinoma. (Table 3)
DISCUSSION
Lung cancer is currently the most frequently diagnosed and the most common cause of cancer mortality worldwide.6 Since cytological sampling by BAL technique relies mainly on cells „exfoliated? from the malignant lesion in the bronchial epithelium, the adequacy of its samples depends on several vital factors, especially a) the degree of differentiation of malignant growth; b) preservation of the morphology of cytological material obtained; and c) technical skill of the clinician who is retrieving the lavage fluid from the bronchus1 In our study of 100 cases suspected of lung malignancy 66 were actually diagnosed positive for malignancy. The mean age of positive cases for malignancy was 60 years in our study and majority were males which correlated with most other studies.2,3,7,8 (TABLE : 4) The sensitivity (42%), specificity (89.6), False Negative Index (60%) and False Positive Index (11%) and accuracy (59%) were comparable to a similar study done by Gaur DS et al in which sensitivity, specificity, False Negative Index, False Positive Index and Accuracy were 39.4%, 89.6%, 60.6%, 10.4%, 71.4% respectively.1 In general, less differentiated, anaplastic lesions have more loosely cohesive cells in comparison to well differentiated lesions. Thus such lesions exfoliate larger number of cells into the Bronchial cavity than the well differentiated lesions.1 In our study too poorly differentiated lesions (44%) exceeded all other types among True positive cases. Similar results were obtained by Gaur DS et al also.1 Squamous Cell Carcinoma (35%) was second most common type after Poorly Differentiated Carcinoma in Biopsy samples as against BAL in which Adenocarcinoma (28%) was the second most common morphological type detected. This is supported by the fact that Squamous Cell Carcinoma followed by Adenocarcinoma are the two most common morphological type of lung malignancy worldwide.7 Similar results were also noted by Poletti et al.9 Small Cell Carcinoma was the next morphological type in both BAL(12%) and Biopsy(15%) samples and results were comparable with Gaur DS et al1 (7.1% BAL, 19.7%Biopsy) and Firoozbakhsh SH et al3 (2/17=12% BAL, 6/47=13% Biopsy). Only one case of Carcinoid tumor was diagnosed in Biopsy which was given falsely negative by BAL cytology much similar to the study by Gaur DS et al.1
CONCLUSION
Considering its safety, Bronchoalveolar Lavage cytology is a good screening method for diagnosing lung malignancy as it is fairly sensitive and specific when compared with Bronchial Biopsy which is the “Gold Standard” method.
 a
a
References:
REFERENCES
1. Gaur DS, Thapliyal NC, Kishore S, Pathak VP. Efficacy of Broncho-Alveolar Lavage and Bronchial Brush Cytology in Diagnosing Lung Cancers,Journal of Cytology 2007; 24 (2) : 73- 77
2. Tuladhar, Panth, Joshi. Comparative analyses of cytohistologic techniques in diagnoses of lung lesions, Journal of Pathology of Nepal (2011).Vol.1, 126-130
3. Shahram Firoozbakhsh, Enayat Safavi. Bronchoalveolar Lavage in the Assessment of Peripheral Lung Cancer, Tanaffos 2003; 2(7) : 7-10
4. Johnston WW, Elson CE. Respiratory tract. In: Bibbo M, editor. Comprehensive cytopathology. 2nd ed. Philadelphia: W.B.Saunders Company; 1997. p. 325-401.
5. Bancroft JD, Gamble M, editors. Theory and practice of histological techniques. 5th ed. New York: Churchill Living Stone; 2002.
6. Travis, W. D., Colby, T. V., Corrin, B., Shimosato, Y., and Brambilla, E. Histological typing of tumours of lung and pleura. In: L. H. Sobin (ed.), World Health Organization International Classification of Tumours, Ed. 3. New York: Springer-Verlag, 1999.
7. Husain AN, Kumar V. The Lung. In: Robbins and Cotran. Pathologic basis of disease. 7th ed. Philadelphia: W.B. Saunders Company; 2006. pp711-22.
8. Rosai and Ackerman?s, surgical pathology, 3rd edition, :Chapter 7:291-340.
9. Venerino Poletti, M.D.,Giovanni Poletti, M.D., Bruno Murer, M.D., Luca Saragoni, M.D.,and Marco Chilosi, M.D. Bronchoalveolar Lavage in Malignancy, Seminars In Respiratory And Critical Care Medicine/Volume 28, Number 5 2007 1
0. John D. Mina. Neoplasms of the lung in Braunwald et al.Harrison?s Principle of Internal Medicine 15th ed. United States of America. MC Graw Hill Inc 2001; 567-71.
11. Springmeyer SC, Hackman R, Carlson JJ, et al. Bronchoalveolar cell carcinoma diagnosed by Bronchoalveolar Lavage.Chest 1983;83:378–379Q48
12. Stover DE, Zaman MB, Hajdu SI, Lange M, Gold J,Armstrong D. Bronchoalveolar Lavage in the diagnosis of diffuse pulmonary infiltrates in the immunosuppressed host. Ann Intern Med 1984;101:1–7
13. Young JA, Hopkin JM, Cuthberston WP. Pulmonary infiltrates in immunocompromised patients: diagnosis by cytological examination of Bronchoalveolar Lavage fluid.J Clin Pathol 1984;37:390–397
14. Sestini P, Rottoli L, Gotti G, et al. Bronchoalveolar Lavage diagnosis of bronchiolo-alveolar carcinoma. Eur J Respir Dis1985;66:55–58
15. Rossi GA, Balbi B, Risso M, Repetto M, Ravazzoni C.Acute myelomonocytic leukemia: demonstration of pulmonaryinvolvement by Bronchoalveolar Lavage. Chest 1985;87:259–260
16. Weynants P, Cordier JF, Chapuis Collier C, et al. Primary immunocytoma of the lung: the diagnostic value of Bronchoalveolar Lavage. Thorax 1985;40:542–54
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





