IJCRR - 6(5), March, 2014
Pages: 25-31
Print Article
Download XML Download PDF
COMPARATIVE STUDY OF FUNCTIONAL OUTCOME OF TIBIAL CONDYLE FRACTURE OPERATIVE (LOCKING COMPRESSION PLATE) VS CONSERVATIVE METHOD
Author: Nitin Sanadhya
Category: Healthcare
Abstract:Aim: was to study the short term follow up and functional outcome of treatment of fracture tibial condyles by conservative and operative methods. And Comparison of result of conservative and operative treatment of the above.And to study the complications of conservative and operative methods. Methodology: The present study had been conducted in Department of Orthopedics Dhanwantri Hospital and research center, Jaipur during the period March 2009 to March 2011. This was a prospective study consist of 50 randomized selected cases of fracture of tibial condyles, treated by conservative and by operative method. Patients older than 15 years were included in this study. Results: In the present study 50 cases of fracture tibia condyle were included patient were divided in 2 groups on random basis managed conservatively and operatively. Majority of cases fall between age group 31-40 and 41-50 age group with average age of 43.86 years and 88% of affected persons were male and commonest mode of injury was RTA accounting for 48% of cases. Most common type of fractures in type C accounting for 40% of cases. Knee instability was found in 32% cases and can be managed conservatively. In the cases with high functional demands type A fracture and type B fractures operative method should be used and in bicondylar comminuted fractures of tibial condyles C3 both the modalities had poor results. Patient treated with operative methods had over all acceptable results in 91.6% as compare to conservative group having 61.5% acceptable results. Conclusion: from this study of 50 cases of tibial condyle fracture we can conclude that the tibial condyle fracture was most commonly caused by RTA and , due to high energy trauma bicondylar fracture were most common type. Type A has excellent results with both the modalities of treatment and type B, C1 and C2 fractures have good results with operative methods; while type C3 had poor results with either of modality.
Keywords: Functional Outcome, Tibial Condyle Fracture, Conservative Method
Full Text:
INTRODUCTION
With the increased density of automobile traffic on our city roads and ever increasing number of road traffic accidents, fractures around the knee have assumed an importance and frequency. In the precarious plight of the city pedestrian, the knee seems to be the most vulnerable point. A hinge joint at the exact level of automobile bumper is most commonly struck on its lateral side resulting in ligament sprains or fracture of one or both condyles. Fracture of tibial condyle were brought into prominence in 1925 by the papers of cotton and Berg in Boston and Conlley and Seiffert in Chicago, one calling them, fender fracture’ and other bumper fracture. The fractures of tibia condyles have three main features. 1) Fractures are intra- articular 2) Occurs in cancellous bone. 3) Involve weight bearing bone. There was great controversy in the past regarding the treatment of fracture of tibial condyles but now with improvement in material and treatment methods of fixation more and more authors agreed that spilt fracture with more than one centimeter displacement, depressed fractures with more than 1 cm displacement Bicondylar fracture with more than 7 mm displacement and depressed fractures of medical condyle shows better results when treated by open reduction and firm internal fixation. (Burri C. et al, 1973: Waddell J.P.et at: 19821: Mason Hole, 1982). While there is still great controversy in the treatment of split depressed fractures with less than 1 cm. displacement, and comminuted fractures. Some authors advocate open reduction and internal fixation (Palmer 1940, Schatzker J. 1979) while other authors advocate conservative treatment (Hohl M. et al 1982; Hugh Dovery 1971: Blockker C.P. et al 1983.) Following operative treatment there is restoration of articular congruity, axial alignment, joint stability and functional movement of joint. Early mobilization is also possible; post traumatic osteoarthritis is less common with operative than with conservative treatment. This treatment modality compromises soft tissue, devascularizes bone fragments and may be complicated with infection, implant failure and wound dehiscence. Difficulties with conservative treatment included inadequate reduction, instability and prolong hospitalization while open reduction and internal fixation is a difficult operation, even in experienced hands. Locking compression plate for proximal tibia are anatomically contured plates with a limited contact profile. The plate is indicated for treatment of split and depressed fractures of the medial and lateral plateau as well Bicondylar fractures of proximal tibia. The goal of treatment of tibial condylar fractures is to obtain a stable pain free, mobile joint and to prevent early degenerative arthritis. The factors producing permanent disability by current methods of treatment are pain, limited motion of the joint, instability, angular deformity, lack of full extension, quadriceps weakness and early degenerative arthritis. An effort was made in this study to analyze the various types of fractures and comparison of end results by conservative and operative treatment. Keeping this in view it is worthwhile to study and evaluate the results of conservative and operative treatment of various types of fracture of tibial condyle and to find out suitable method of treatment for different type of fractures.
AIMS AND OBEJECTIVES
1. To study the short term follow up and functional outcome of treatment of fracture tibial condyles by conservative and operative methods. 2. Comparison of result of conservative and operative treatment of the above. 3. To study the complications of conservative and operative methods.
MATERIAL AND METHODS
The present study has been conducted in Department of Orthopedics Dhanwantri Hospital and research center, Jaipur during the period March 2009 to March 2011. This is a prospective study consist of 50 randomized selected cases of fracture of tibial condyles, treated by conservative and by operative method. Patients older than 15 years were included in this study. Initial management and resuscitation done
CONSERVATIVE METHOD
a) Close reduction and skeletal traction followed by cast brace with hinge knee joints
DISCUSSSION
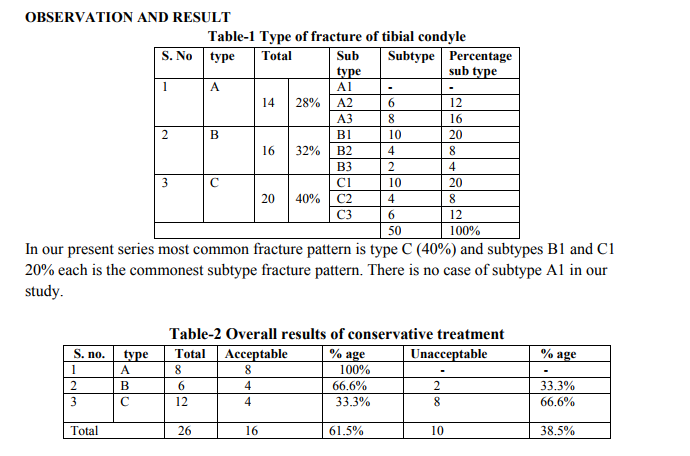
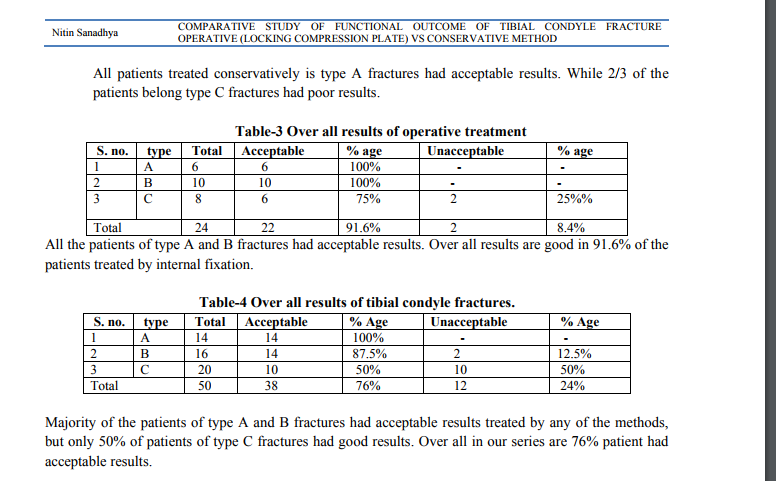
The ideal outcome after a tibia plateau fractures is stable, pain-free, non osteoarthritic knee joint with a range of motion that is adequate for functional requirements. There is virtual universal agreement that reduction and stabilization of displaced fragments , early mobilization and delayed weight bearing are necessary to achieve the optimal results, however controversy exists as how to achieve these aims . There is debate about the efficacy of the different modalities. Closed reduction with lower tibial skeletal traction for three weeks followed by hinge knee cast and later weight bearing permitted as the fracture consolidates, is cost effective treatment with less chances of infection and can be applied to medically unfit patients. In the modern age operative treatment with locking compression plate fixation after adequate reduction permits better stabilization and early weight bearing .But this type of management needs experienced hands ,requires extensive exposures of the knee joint, and have a risk of further devascularization of the bone and chances of infection . In this study critical evaluation is done of the tibial fractures treated with either of the modality. We have classified the fractures according to AO classification and the most common type of fracture in our series was type C (40%) followed by type B (32%) subtype B1 and C1 20% cases was the commonest subtype fracture pattern ,their was no case of subtype A1 in our study. In the study majority of the cases sustained injury due to RTA(48%). 16% were injured due to the motorcycle / scooter skid while in 20% cases the injury was due to pedestrian accidents. The commonest injury results from RTA were A3, B1, C1, C3 due to severe trauma which shatters the upper end of the tibia. The common fracture in the motorcycle skid was C2, C1, B3, while pedestrian commonly had B1 or depressed B2 type fractures. In the present series, 32% cases had ligamentous injuries of the knee, Medial collateral ligament injury was found in 12% cases and the lateral collateral ligament was found in 4% cases. The anterior cruciate ligament injury was in 16% cases. Blocker CP (1983) reported MCL injury in 20% cases. Schatzker et al (1979) reported ligamentous injuries in 32% cases. The associated meniscal injuries cannot be diagnosed at the time of injury because of severe pain and haemarthrosis. After the period of 4 weeks enough fibrosis in the capsule and meniscus developed, so it cannot also be diagnosed at follow up. Diagnosis requires MRI and arthroscopy. These diagnostic tools are not used in the present study. The associated ligament injuries were treated conservatively, provide sufficient ligamentous healing. out of 16 patients of ligament injuries 50% had acceptable results and do well in there daily living activities. In the study no case of peroneal nerve palsy reported. Associated fracture of fibula was found in 64% cases, in displaced lateral condyle and bicondylar fractures. They were treated conservatively and didn’t affect the final out come. Barford (1980) rightly said that fibula head act as a buttress of the lateral plateau, if this gives way entire lateral segment slides down enmass, causing major displacement. Burn (1940) also made similar findings. In the present series knee flexion was restricted in 22 (44%) cases out of which 10 (20%) had minimal restriction (100-120 degree) while 12 (24%) patients had gross restrictions of the knee movements. Most of the patients regain their functional range of motion within 12 weeks of injury. Patient with more comminuted fractures regain their flexion range more slowly because of more pain and swelling. Over all 75% of the patients in our study had acceptable range of movements, results were slightly better in operative group than conservative group. George Rasmussen 1973, Dewelios PJ 1997 Dendrinos GK 1996, Weigel D.P. Marsh JL 2002 ,Lubowitz 2004 reported slight better range of movements from 117 to 120 degrees in cases treated operatively. Extension lag of 5 degree to 10 degree was seen in 8 (16%) cases and was mainly seen in bicondylar fractures with poor fractures reduction , similar observation is noted by Fryjordet (1972) 21%, Jacobson (1953) 17% and Huge Dovery (1971) 22% cases. they all have thigh muscle wasting so advised continues quadriceps strengthening exercises. In the present study, deformities of the knee were found in 14 (28%) cases. varus deformity in 10 (20%) cases and valgus in 4(8%) . Rombold C in 1960 reported deformities of knee in 40% cases and Jacobson (1953) reported deformities in 15% and Huge Dovery (1971) in 10% cases. No deformity was found in undisplaced fractures, varus deformity is a sequel of either displaced medial condyle fracture or bicondylar fracture. In our series varus and valgus deformity were seen in cases treated with skeletal traction with hinge knee cast mainly seen in C3 type of fractures that were severely comminuted and displaced fracture, Displacement may occur during traction, mobilization or weight bearing. Over all 16 patients (32%) complain pain in the present series our findings are similar to Fryjordet (1967) who reported it in 33% cases but in contrast to our study Jacobson reported pain in 63% cases in his series. Pain was more common in patients of bicondylar fractures treated conservatively. Ligamentous injuries are treated conservatively and majority of patients performed well. similarly Moore (1976) and Weisseman and Hrold (1964) favored the non operative treatment; in contrast to view of O,Donogue ( 1976) and Robert J (1960) who insisted upon the open repair of the collateral ligament rupture for optimal joint function. In the present study instability of the knee was found in 16 cases (32%) out of which 50% are asymptomatic and perform well. Similarly knee instability is reported by Rombold C (1950) 20%, Fryjordet (1967) 30% and Huge Dovery (1971) 39%. In this present series Hohl and Luke (1976) criteria was used for the assessment of final results .we had 100% acceptable results in type A fractures, 66.6% in the type B and only 33.3% in type C fractures in the patients treated conservatively. The over all acceptable results with conservative treatment was 61.5% which was similar to the series of Thomas Decoster 1988,who reported 61% good results but results of George brown (1976) 70% and Rick D Hole (1989) 76% were better than our present study. Our results were much better in patient treated by open reduction and internal fixation. There were 100% acceptable results in type A and B fractures while in type C fractures were 75% acceptable results. The over all good results were in 91.6% patients. Similar results had been reported by Dennan and Lubowitz (2004) 94% and Krappinger (2008) 96% our results were slightly better than Rasmessun (1973) 86% , Mikulu(1988) 87%, Weigel DP marsh 87%,Ballmer (2000) 86.7%. Over all results in our series irrespective of method of treatment were 100% acceptable in type A fractures, 87.5% in type B fractures and 50% in type C fractures. We have acceptable results in 76% cases while in 24% cases it is unacceptable. In type C3fractures results were uniformly bad in the cases treated by either method. It can be concluded from the present study that type A fractures can be treated by any of the method with 100% acceptable results. In type B fractures our results were better with open reduction and internal fixation as compared to conservative treatment, 100% and 66.6% respectively. In type C fractures there were only 33.3% acceptable results with conservative treatment as compared to 75% acceptable results with operative treatment. The over all results of type C3 fractures treated by either of method are uniformly bad. However over all results in present series were superior in patients treated by internal fixation than treated conservatively
CONCLUSION
In this study of 50 cases of fractures of tibial condyle. Treatment modalities included were lower tibial skeletal traction and later hinge knee cast, open reduction with proximal tibial locking compression plate fixation. ? Minimum follow up period was 6 months and maximum was 20 months. Average is 13.86 months. ? Majority of cases were in 31-40 and 41- 50 age group with average age was 43.86 years and sex ratio M:F is 7.33:1. ? Left and right knee were involved in equal percentage, lateral condyle was involved in 28% cases, medial condyle was involved in 20% cases and both condyle were involved in 52% percentage of cases. ? Commonest mode of injury was RTA ? No case of common peroneal nerve injury occurred. ? Associated fracture of fibula was found in 64% cases. ? Commonest fracture was type C fractures and subtypes B1 and C1 20% cases each. ? Knee instability was found in 32% cases. An can be managed conservatively. ? Thigh muscle wasting was found in 32% patients but no functional weakness found. ? Gross restriction of knee flexion was present in 24% cases. ? Extension lag was seen in 16% cases. ? Varus deformity was seen in 20% cases and valgus deformity in 8% cases. ? Patient treated with lower tibial skeletal traction and hinge knee cast shows over all 61.5% satisfactory results with subtype A had 100%, subtype B had 66.6% and sub type C had 33.3% acceptable results. ? Patient treated with open reduction and internal fixation shows over all 91.6% satisfactory results with subtype A and B had 100% and sub type C had 75% acceptable results. ? Displaced fractures better be treated with open reduction and internal fixation and comminuted bicondylar fractures C3 has equally poor results with both conservative and operative treatment.
References:
REFERENCES
1. Blockker: A clinical and radiological study tibial condyle fracture:J of ortho trauma:1983, JBJS , 450-60.
2. Dendrinos GK.: Treatment of high energy tibial plateau fractures by the contured locking plates, journal of bone and joint surgery78 (5): 710-7,1996.
3. Duwelivos PJ: Treatment of tibial plateau fracture by limited internal fixation. Clinical orthopedics and related research (339): 47-57, 1997.
4. Fryjordet A. Jr.: Operative treament of tibial condyler fractures. Acta. Orthop Scand: 1967; 113-17.
5. Hohl M. and Luck J.V. Fractures of tibail condyle. A clinical and experimental study. J. Bones and joint Surg. 1967; 49 A: 1455.
6. O’Dongue: Ligament in tibial condyle fracture diagnisis and operative management:JBJS:124-130:1976
7. Porter B. : Crush fractures of the lateral tibial plateau J.Bone and Joint Surg. 1970;528:676.
8. Rombold C,: Depressed fractures of tibial plateau J.Bone and joint Surg. 1960;42A:783.
9. Rasmussen et al: Operative treatment and their outcome of tibial condyle fractures:J of ortho trauma 1973.
10. Rick D and Hole:Conservative treatment of tibial condyle fracture with functional cast brace. JBJS: 23: 132-139:1989.
11. Schatzker et al: Tibial condyle fractures classification and management :1979.JBJS
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





