IJCRR - 6(6), March, 2014
Pages: 84-86
Print Article
Download XML Download PDF
BIFID RIBS - A RARE CHEST WALL DEFORMITY:A CASE REPORT
Author: Murali Krishna S., Rajesh V., Udaya Kumar P., Kalpana T., Chandra Mohan M., Naveen Kumar B.
Category: Healthcare
Abstract:Aim: Aim of the present case is to report and describe a rare case of chest wall deformity in a 70 years old male cadaver. Case Report: Variations in the anterior chest wall are rare. Present case describes bifid ribs involving the right 3rd rib and 3rd costal cartilage, 5th rib and 5th costal cartilage which were observed during routine dissections for undergraduate medical students. When compared to the lower intercostal spaces, the upper intercostal spaces of the third and fifth bifid ribs were found to be narrow. Intercostal muscles were present in both the bifid spaces. They received their nerve supply and arterial supply from the 3rd and 5th intercostal nerves and arteries respectively. Conclusion: It is important to know about such anatomical variations, for clinicians during differential diagnosis with other diseases, such as a chest wall tumors or costal fracture and for counting the ribs.
Keywords: Bifid rib, intercostal space
Full Text:
INTRODUCTION
Twelve pairs of ribs develop from costal processes in thoracic region during the 9th week of intrauterine life. The elongated cartilaginous costal arches get ossified to form the ribs. True ribs articulate to the sternum via the costal cartilages by 45th day and false ribs do not articulate with the sternum. Secondary ossification centers appear at 15 years. [1] A bifid rib is a congenital abnormality found in the anterior chest wall, with the sternal end of the rib cleaved into two, enclosing an additional intercostal space. The over all prevalence of bifid rib is 0.15% to 3.4% of the population. It is commonly unilateral and may be asymptomatic. This anomaly may be found incidentally on chest radiography [2].
CASE REPORT
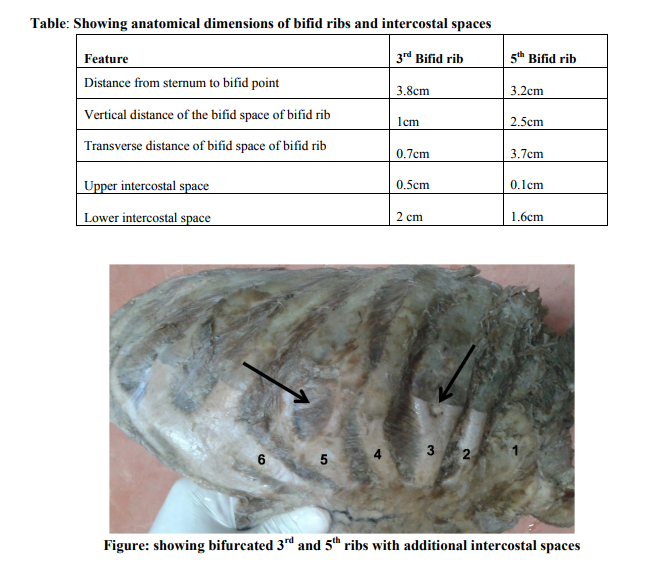
During routine cadaveric dissection of the thorax of a man aged about 70 years, in Department of Anatomy, Mamata Medical College, Khammam, we observed variations of bifid appearance involving the right 3rd rib and 3rd costal cartilage and right 5th rib and 5th costal cartilage enclosing an additional circular intercostal space. On careful observation of the specimen we found that intercostal muscles were present in both the additional intercostal spaces but the 3rd additional intercostal space was too small space for the muscles to be distinguished. They were supplied by collateral branches of 3rd and 5th intercostal nerves. Arterial supply was by 3rd and 5th intercostal arteries. The dimensions of upper intercostal spaces were narrower than the lower intercostal spaces. The morphological measurements revealed that the distance from the lateral border of sternum to the bifid point in the 3rd intercostal space is 3.8 cm and in 5th intercostal space is 3.2 cm. The additional intercostal space of the 3rd bifid rib measured 1 cm in vertical distance and 0.7 cm in transverse distance and of 5th bifid rib is 2.5cm in vertical distance and 3.7 cm in transverse distance. The upper intercostal space between the 2nd and 3rd rib was narrowed and it measured 0.5 cm. The lower intercostal space between the 3rd (unusual rib) and 4th rib was widened measuring 2 cm. The upper intercostal space between the 4th and 5th rib was narrowed and it measured 0.1cm and the lower intercostals space between 5th and 6th rib measured 1.6 cm (Table No. 1).
DISCUSSION
Common congenital rib anomalies can be classified into numerical and structural. Numerical anomalies include supernumerary ribs like cervical, lumbar, pelvic or sacral and sometimes deficiency in total number of ribs. Structural abnormalities include short ribs, bifid ribs, fused or bridged ribs and pseudoarthrosis of first rib. [2, 3] Bifurcation of the rib and presence of additional intercostal spaces is a rare abnormality of thorax. Very few cases have been reported on such variations. Song et al., reported three cases of bifurcation of the right fourth rib [4]. Cristopher D Stickly et al., reported the presence of bifurcated 4th rib in one cadaver [5]. Development of intra thoracic rib is doubtful, however it may result from an incomplete fusion of cephalic and caudal segments of sclerotome during the development, occurring around the 4–6th week of foetal life [6]. The incidence of bifid ribs is more frequent in males than females. It is more common in the third and fourth ribs (degree of incidence - third > fourth > fifth > sixth > second) [5, 7]. Comparatively it is more prevalent on the right side of the chest than on the left side [8]. Some times bifid ribs can be present on both the sides. Presence of bifid rib may be associated with a syndrome called Basal cell nevus syndrome or Gorlin-Goltz syndrome. It is a hereditary multisystemic disorder that predominately affects the skeletal system, skin, eye and reproductive systems [9]. In the present case, bifid ribs were present in 3rd and 5th intercostal spaces on right side with narrowing of upper intercostal spaces.
CONCLUSION
This is the first case reported in cadavers where two bifid ribs are present on right side of the chest wall. It is necessary for the clinicians to know about this malformation because this may cause confusion during counting the ribs for some surgical procedures and diagnostic procedures. It is also necessary for the differential diagnosis with other diseases, such as costal fractures and chest wall tumours.
Competing interests
The authors declare that we have no competing interests
Ethical committee clearance
As the study included only human cadavers, ethical committee clearance was not taken into consideration. Authors will take the responsibility of any further allegations regarding ethical clearance that arise from the study.
References:
REFERENCES
1 Ronald b.j glass,MD,Karen,I,Norton et al, paediatric ribs: a spectrum of abnormalities, Radiographics January 2002 22:1 87-104.
2 Anita R, Archana R, Jyoti C, Punita M. Synostosis of First and Second Rib – Case Report. Jornal of Anatomical Society of India. 2009; 58(2): 189- 191.
3 Deepak S, Dakshayani KR. An unusual Case of a Bicipital Rib – A Report. Anatomica Karnataka. 2011; 5(1): 50-52.
4 Song WC, Kim SH, Park DK, Koh KS. Bifid rib: anatomical considerations in three cases. Yonsei Med J. 2009; 50: 300–303.
5 Cristopher D Stickly, Kaori Tamuri, et al., bifurcation of fourth rib as possible indicator of Gorlin Syndrome in a 85 yr old female cadaver. International Journal of Anatomical variation (2013) 6 : 86 – 89.
6 Satheesha Nayak.B. A case of bifid rib and additional intercostals space. International Journal of Anatomical Variations .2012 ;5:128–129.
7 Schumacher R, Mai A, Gutjahr P. Association of rib anomalies and malignancy in childhood. Eur J Pediatr. 1992; 151: 432–434.
8 Osawa T, Onodera M, Feng XY, Sasaki N, Nagato S, Matsumoto Y, et al., Two cases of bifid rib observed in the fourth and the fifth rib. Dental Journal of Iwate Medical University. 2002; 27: 98–103.
9 Rai S, Gauba K. Jaw cyst-Basal cell nevusBifid rib syndrome: A case report. J Indian Soc Pedod Prevent Dent - September 2007, 25:137-139
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





