IJCRR - 6(6), March, 2014
Pages: 55-57
Print Article
Download XML Download PDF
CASE REPORT OF SYNOSTOSIS OF FIRST AND SECOND RIB - A BRIDGED VARIETY
Author: Uttama U. Joshi, N.R. Mudiraj
Category: Healthcare
Abstract:Congenital anomalies of ribs are rare incidental findings. Structural malformations of first rib are common as compared to other ribs. When such anomaly is present, may lead to compression of neurovascular bundle at the root of the neck causing thoracic outlet syndrome (TOS). The reported case of a rare bone specimen was an incidental finding during routine sorting of bones from the department. The specimen displayed fusion of right sided first and second rib in the midshaft region with free anterior and posterior ends. Such skeletal abnormality may be associated with segmentation defects of bony tissues and variations in the disposition of neurovascular structures, thus making them vulnerable for compression at thoracic outlet. Thus the awareness and precise knowledge of such anomaly is important for the anatomists, radiologists and thoracic surgeons dealing with this region.
Keywords: congenital anomalies, rib, synostosis, bridged, thoracic outlet syndrome.
Full Text:
INTRODUCTION
Ribs are essential components of thoracic cage. Anomalous ribs are rare anatomical findings. Such ribs are usually discovered as an incidental observation on routine chest radiographs or as a part of systemic disorder or syndrome. Almost 22 syndromes are described which involve rib anomalies as one of their component, eg.Poland syndrome, Klippel-Feil syndrome, Jarco-Levin syndrome etc. Presence of cervical rib, hypertrophied scalenus anterior and other factors obliterating either interscalene space or costoclavicular space lead to thoracic outlet syndrome (TOS).6 Abnormal 1st and 2 nd ribs can present with TOS.7,1 These anomalies include fused cervical rib and first rib or fused first and second rib.6 First rib anomalies can cause compression of structures as it creates narrow space through which the brachial plexus and subclavian vessels pass.2 This report is an attempt to throw light on the morphological implications and clinical significance of the specimen.
CASE REPORT
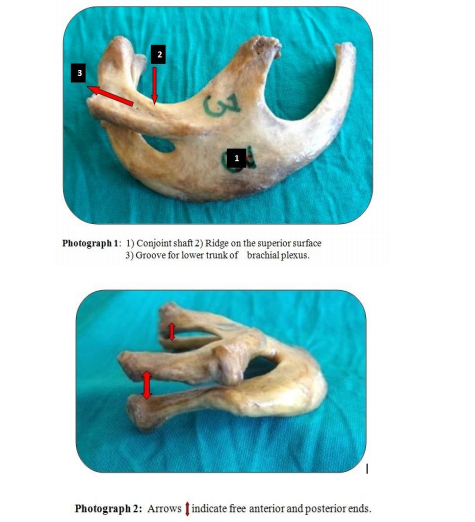
During routine sorting of bones from the departmental collection, a rare bone specimen displaying fusion of right sided 1st and 2nd rib in midshaft region was detected. The specimen was examined in detail for relevant anatomical features and various measurements. The morphological examination revealed fusion of the two ribs in midshaft region with free anterior and posterior ends. Thus the common shaft formed by their junction made it a bridged variety. This has resulted in the obliteration of 1st intercostal space in the conjoint shaft region. But a small intercostal space was present in the anterior and posterior ends. This common shaft had a maximum width of 42.6mm and length of 34.8mm. The first rib presented a facet separately on head and tubercle. The head of second rib had two facets of equal size separated by a ridge. The neckportions of the ribs were directed backwards and laterally. The maximum gap separating the neck regions of the two ribs was 5.92 mm (vertical). The first rib presented inconspicuous scalene tubercle close to the anterior end. The superior surface of the rib (1st) specimen displayed grooves and ridges. It showed a ridge extending from inner border of neck of first rib to the middle of conjoint shaft. Behind this ridge a well-marked large and rough impression was observed on the 1st rib for the attachment of scalenus medius muscle. A prominent bossing was observed on the superior surface of common shaft close to the outer border of 2nd rib for serratus anterior. The inner surface of the conjoint shaft was smooth and featureless and showed few vascular foramina.
DISCUSSION
The ribs develop from the mesenchymal processes of the primitive vertebral arches in the thoracic region. Morphological anomalies of the ribs and vertebrae can occur if malsegmentation of axial skeleton takes place before 20th day. Malexpression of myogenic determination factors like Myo D, Myogenin, Myf 5 and MRF4 could be the potential cause of such anomalies. Errors in segmentation of body tissues during development may be associated with variations in the disposition of nerves and vessels.5 Rib anomalies are traditionally classified into numerical and structural. Numerical anomalies are common such as supernumerary (cervical / lumbar) and deficient pair of 11th rib. Structural abnormalities are quite rare and they can be further classified as bifid, short, fused ribs. The fusion anomalies can be classified in to 3 types: (1) Bicipital rib- fused anterior ends and shafts but free posterior ends; (2) Bridged rib – fused shafts but free anterior and posterior ends; (3) Forked rib – fused posterior ends but separate shafts as well as anterior ends. Such fusion anomalies due to errors in the segmentation of body tissues may be associated with variations in the disposition of nerves and vessels.4 Costal anomalies occur frequently at the thoracic outlet. The abnormal 1st and 2nd rib can present with thoracic outlet syndrome. In the present case report, this rare bone specimen displayed the synostosis of right sided 1st and 2nd rib in the midshaft region leading to the formation of bridged type of anomaly. The anomalous first rib instead of forming synostosis may remain floating in the soft tissue similar to those found in birds, or may be attached by a ligamentous band with sternum. In the present case, both the ribs displayed costal facets which confirmed their articulation with thoracic vertebrae. The separate anterior ends confirmed articulation with sternum. 1 st rib anomaly can cause compression as it creates narrow space through which the plexus and subclavian vessels pass. First rib malformations are commonly associated with postfixed brachial plexus with large contribution from second thoracic nerve.7 Thus, the well formed groove on the superior surface of the first rib may be due to extra pressure contributed by second thoracic nerve or due to greater stretching of the lower trunk of brachial plexus. This may result in the neurological symptoms of TOS. Significant vascular compression and symptoms are also reported with congenitally abnormal first rib and associated second rib synostosis.7, 1 This warrants early surgical intervention. Fusion anomalies of ribs can cause scoliosis and restriction of chest movements, which may require surgical correction. We as an anatomists opine that the precise knowledge and awareness of such fusion anomaly as encountered in the present study has clinical significance besides academic interest.
CONCLUSION
Such fusion anomalies should be kept in mind before surgical interventions for the cases of thoracic outlet syndrome (TOS) and scoliosis.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in reference of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. Baumgartner F, Nelson RJ, Robertson JM. The rudimentary first rib: A cause of thoracic outlet syndrome with arterial compromise. Arch Surg.1989;124: 1090–92.
2. Edrogan Atosy. Thoracic outlet syndrome: anatomy, Hand Clin.2004;20:7-14.
3. Hashimoto H, NikaidoY, Nagai S, Shimada K.A case report of thoracic outlet syndrome with acute arterial obstruction caused by abnormal first rib. Journal of the Japanese association for Thoracic Surgery 1997;45 (12):2026-29.
4. Rani Anita, Rani Archana,Chopra J,Manik P.J. Anat.Soc.India 2009;58(2):189-91.
5. Todd TW.Costal anomalies of the thoracic inlet, interpretation and significance. Anal Anz.1912;41:257-71.
6. Turner WM. Cervical ribs and the so called Bicipital ribs in man in relation to corresponding structures in the Cetacea. Journal of anatomy and Physiology.1883; 17(30):384-400.
7. White JC, Poppel MH, Adams R. Congenital malformations of the first thoracic rib: A cause of brachial neuralgia which simulates the cervical rib syndrome. Surg Gynecol Obstet.1945; 81: 643–59.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





