IJCRR - 6(6), March, 2014
Pages: 09-13
Print Article
Download XML Download PDF
USAGE OF PROTEIN/CREATININE RATIO IN SPOT URINE SPECIMEN FOR EARLY IDENTIFICATION OF PRE-ECLAMPSIA
Author: Jaya Choudhary, Vineeta Garg , Abhilasha Bansal Department
Category: Healthcare
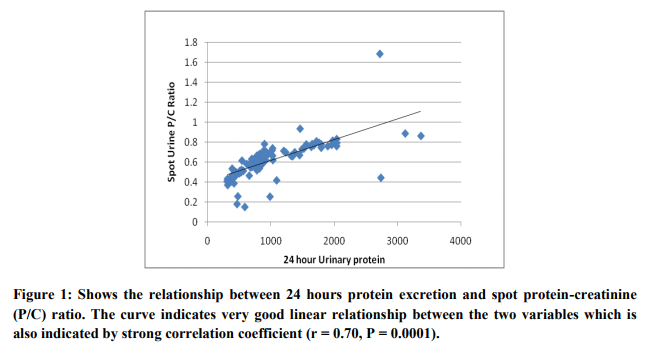
Abstract:Objective: To evaluate the diagnostic usage of spot urine protein-creatinine (P/C) ratio for quantification of proteinuria for predicting pre-eclampsia. Methods: A spot mid stream urine sample were collected for estimation of P/C ratio and the 24- hour urine sample for protein estimation was collected. The correlation between the spot P/C ratio and 24-hour urine proteinuria was done. Logistic regression analyses have been used to analyse data. Results: The spot P/C ratio and 24-hour urine protein excretion have well correlated (pearson's correlation coefficient r = 0.70; P < 0.0001). Conclusion: Spot urine P/C ratio is an easy, rapid and useful test for assessment of proteinuria for diagnosis of pre-eclampsia.
Keywords: spot urine specimen, Protein/creatinine ratio, 24 Hour urinary protein, pre-eclampsia.
Full Text:
INTRODUCTION
Obstetricians should be aware about early diagnosis of pre-eclampsia, the hypertensive disorder of pregnancy results in sever maternal and perinatal complications that affects 5% - 10% of pregnancy. (1) Preeclampsia is multisystem disorder related with pregnancy that is characterized by progressively elevation of blood pressure and proteinuria after 20 weeks of gestation. Some time blood pressure and proteinuria become significantly high and causing symptoms of end-organ damage which further results in fetal growth restriction. Preeclampsia is consequences in cerebrovascular and cardiovascular complications, acute renal failure, disseminated intravascular coagulation, placental abruption and maternal death. (2) It is very crucial for pregnant woman. Proteinuria of 0.3 g/day or more is gold standard for diagnosis of pre-eclampsia.(3) The measurement of proteinuria in pregnancy is done by collection of 24 hour urine.(4) The collection of urine is time consuming and uncomfortable for women and ward staff. It requires refrigeration and can create confusion if collected inaccurately. The collection of the urine cannot possible in case of delivery occurs, which lead to uncertainty of diagnosis of pre-eclampsia because proteinuria cannot be measured. (5) A long process in collection and estimation in 24 hour urinary protein causing expanded hospital stay of pregnant women in work up for pre-eclampsia thereby increasing risk of nosocomial infection, anxiety and unnecessary costs to patient. There is requirement an early diagnostic tool for it. The International Society for the Study of Hypertension in Pregnancy has proposed use of protein: creatinine ratio in random urine sample instead of 24 hour urine collection. (6) A rapid and sensitive test which should give equivalent results of 24 hours urine is required. Protein-creatinine ratio in spot urine sample is a substitute to estimation for proteinuria which is convenient, fast method and not influenced by changes in urinary solute concentration.(7) This study was carried out to evaluate the diagnostic accuracy of spot urine proteincreatinine ratio for the detection of significant proteinuria in patients with pre-eclampsia.
MATERIAL AND METHODS
A prospective study was designed which include 115 pregnant women of >20 weeks of gestation period and suspected pre-eclampsia (>140/90 mm hg Blood pressure), admitted in, Dept. of Gynecology, MGM medical college, Jaipur, over a period of 6 months. Pregnant women with chronic hypertension, diabetes mellitus, or preexisting renal disease were excluded. A detailed history with thorough clinical examination and routine investigations, liver function test, renal function test was done to select women. A protein/creatinine ratio was estimated, which was followed by the commencement of a 24-hour urine protein assessment. The relationship between protein-creatinine ratio and 24-hour protein excretion was assessed by Pearson correlation coefficient. Total urine protein quantification was done by well established, Biurate calorimetric assay and urine-creatinine estimation was done by modified Jaffe’s method. The urine P/C ratio was calculated by dividing the urinary protein concentration in mg/dl by the urine creatinine concentration in mg/dl. P value of 0.05 was considered to be significant.
RESULTS
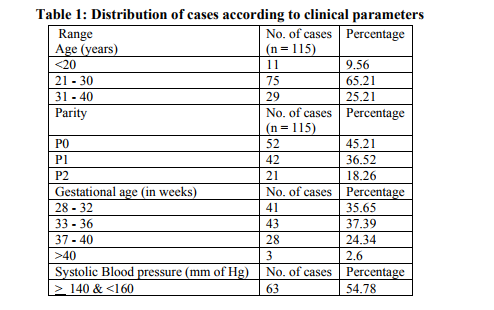
A total of 125 pregnant women with preeclampsia were included according to diagnostic criteria of pre-eclampsia and exclusion criteria.3 women were delivered before proper collection of 24 hour urine, 5 had chronic hypertension and in 2 women, pregnancy had to terminate because of severe preeclampsia, and in another because of placental abruption. Table 1 shows maximum number (65.21%) of subjects of age group 21 to 30 years. Most of the women were nulliparous (54.78%), followed by primipara (45.21%). Majority of pre- eclampsic women were belong to group 33 to 36 weeks gestational age (37.39%), followed by group 28 to 32 week gestational age (35.65%).Most of women (54.78%) were having systolic blood pressure between 140 to 160 mm of Hg and 58 % of women were having diastolic blood pressure between 90 to 110 mm of Hg. Majority of women were detected with proteinuria between > 3 and < 5 gm/24 hrs.

DISCUSSION
Early diagnosis and confirmation of preeclampsia is very crucial for the management of it. For severity Assessment and diagnosis of preeclampsia, estimation of proteinuria is essential. Spot urine sample for urinary protein creatinine ratio is easy and more suitable than 24h urine collection for screening preeclampsia. It is hassle free, rapid and economical for patients. Results are not affected, if collected inaccurately.(8,9) It is very useful when there is less time to collect 24h urine in case of severe hypertension and since delivery is commenced (10) In this study we included 115 pregnant women induced hypertension. The young age group (21 - 30 yrs) showed highest incidence (65.21%) of PIH. J. O. Eigbefoh et al also found the same results and support our data that young age (age group 20 - 29 years (75.6%)) women are affected more with PIH (10) Mostly nulliparous women were affected with PIH in present study. J. O. Eigbefoh et al also showed that most of pregnant women were nullipara (54.7%) followed by primipara (15.15%). (10) Preponderance of preeclampsia were found in group 33 to 36 weeks gestational age (37.39%), followed by group 28 to 32 week gestational age (35.65%), showing that these gestational age range are more prone to PIH. Most of women (54.78%) were having systolic blood pressure between 140 to 160 mm of Hg and 58 % of women were having diastolic blood pressure between 90 to 110 mm of Hg. Majority of women were detected with proteinuria between > 3 and < 5 gm/24 hrs. The study of Amita et al is well correlated with our study. (11) We found an acceptable correlation between Protein/creatinine ratio in spot urine and 24hr urinary protein. Previously some researcher also has been done studies to establishing spot P/C ratio as an indicator for pre-eclampsia. Leonos – Miranda described a significant correlation (r= 0.8 ) (12) Durnwald and Mercer found lower correlation coefficients of 0.56 and not agreed for replacing spot P/C ratio for the 24 hour urine protein collection.(13) But an another study showed a significant relationship between random protein-creatinine ratio and 24-hour protein with higher correlation coefficients (r = 0.56, P < 0.01).(14) Wheeler et al gave the value of the P/C ratio with their corresponding 24 proteinuria values. The value of P/C ratio 0.46, 0.82 and 3.0 corresponded to 1000 mg/ 24 h 2000 mg/ 24 hr and 3000 mg/24 hr, respectively. The proteinuria for 24 hour was represented by the urine P/C ratio of 0.21. (15) The present study proposed that the spot urine protein creatinine ratio can used an alternative method for taking clinical judgment about proteinuria in preeclampsia. This investigation can be used on outdoor basis for fast clinical decision instead of time consuming process 24 hr urine collection. There are some limitation of our study that is small sample size and some false negative results. Further studies can overcome this issue including a larger study population and usefulness of this test in rapid and easy management of preeclamptic patients.
. CONCLUSION
The spot urine P/C ratio and the 24 hour proteinuria were well correlated. Spot urine protein-creatinine ratio can be used to predict the amount of 24 hours urine protein excretion with high accuracy. But the 24 hr urine collection remains the gold standard for evaluation for preeclampsia. So, spot urine protein-creatinine ratio can be used for detection of significant proteinuria in pregnant women with suspected preeclampsia with high accuracy, which is more rapid than 24 hour urine protein excretion. Thus this is a very useful and easy investigation to check the maternal morbidity.
References:
REFERENCES
1. Majhi, A.K., Mondal, A. and Mukherjee, G.G. (2001) Safe motherhood—A long way to achieve. Journal of Indian Medical Association, 99, 132-137.
2. Mackay AP, Berg CJ, Atrash HK. Pregnancyrelated mortality from preeclampsia and eclampsia. Obstet Gynecol 2001;97:533-8.
3. BrownMA, HagueWM, Higgins J, LoweS, McCowanL, Oats J, et al. The detection, investigation and management of hypertension in pregnancy: executive summary. Aust N Z J Obstet Gynaecol 2000;40: 133-8.
4. BrownMA, LindheimerMD, de Swiet M, Van Assche A, Moutquin JM.The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy 2001;20:IX-XIV.
5. Wongkitisophon K, Phupong V, Yamasmit W, Pansin P, Tannirandorn Y, CharoenvidhyaD. Correlation of 4- and 24-hour urine protein in women with initially diagnosed hypertensive disorders in pregnancy. J Med Assoc Thai 2003;86:529-34.
6. Ginsberg JM, Chang BS,Matarese RA, Garella S. Use of single voided urine samples to estimate quantitative proteinuria.N Engl J Med 1983;309:1543-6.
7. Al, R.A., Baykal, C., Karacay, O., Geyik, P.O., Altun, S. and Doten, I. (2004) Random urine protein creatinine ra-tio to predict protenuria in new onset mild hypertension in late preganncy. Obstetrics and Gynecology, 104, 367- 371.
8. Chitalia VC, Kothari J, Wells EJ, Livesey JH, Robson RA, Searle M, Lynn KL. Cost-benefit analysis and prediction of 24-hour proteinuria from the spot urine protein creatinine ratio. Clin Nephrol 2001;55(6):436-47.
9. Menzies J, Magee LA, Macnab YC, Ansermino JM, Li J, Douglas MJ, Gruslin A, Kyle P, Lee SK, Moore MP, Moutquin JM, Smith GN, Walker JJ, Walley KR, Russell JA, von Dadelszen P. Current CHS and NHBPEP criteria for severe preeclampsia do not uniformly predict adverse maternal or perinatal outcomes. Hypertens Pregnancy 2007;26(4):447-62.
10. Eigbejoh, J.O., Abebe, J., Odike, M.A. and Isabu, P. Protein/creatinine ratio in random urine specimen for quantitation of proteinuria in pre-eclampsia. Internet Journal of Gynecology and Obstetrics, 2007; 18:1.
11. Sharma A, Kiran P, Ajai B. Spot urine protein/creatinine ratio—A quick and accurate method for diagnosis of pre-eclampsia. Open Journal of Obstetrics and Gynecology, 2013, 3, 609-612.
12. Leaños-Miranda A, Márquez-Acosta J, Romero-Arauz F, Cárdenas-Mondragón GM, Rivera-Leaños R, Isordia-Salas I, UlloaAguirre A. Protein: creatinine ratio in random urine samples is a reliable marker of increased 24-hour protein excretion in hospitalized women with hypertensive disorders of pregnancy. Clin Chem 2007; 53(9):1623-8.
13. Durnwald, C. and Mercer, B. (2003) A prospective comparison of total protein/creatinine ratio versus 24-hour urine protein in women with suspected preeclampsia. American Journal of Obstetrics and Gynecology, 189, 848- 852.
14. Al, R.A., Baykal, C., Karacay, O., Geyik, P.O., Altun, S. and Doten, I. (2004) Random urine protein creatinine ratio to predict proteinuria in new onset mild hypertension in late pregnancy. Obstetrics and Gynecology, 104, 367- 371.
15. Wheeler 2nd, T.L., Blackhurst, D.W., Dellinger, E.H. and Ramsey, P.S. (2007) Usage of spot urine protein to creatinine ratios in the evaluation of pre-eclampsia. American Journal of Obstetrics and Gynecology, 196, 465e1-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





