IJCRR - 6(7), April, 2014
Pages: 65-73
Print Article
Download XML Download PDF
ASSESSMENT OF OXIDATIVE STRESS AND ANTIOXIDANT STATUS AMONG NEWBORNS IN RELATION TO MODE OF DELIVERY
Author: Soumika Biswas, Swati Bhattacharyya, Chinmoy Ghosh, Sayari Banerjee, Kasturi Mukherjee, Arghya Basu
Category: Healthcare
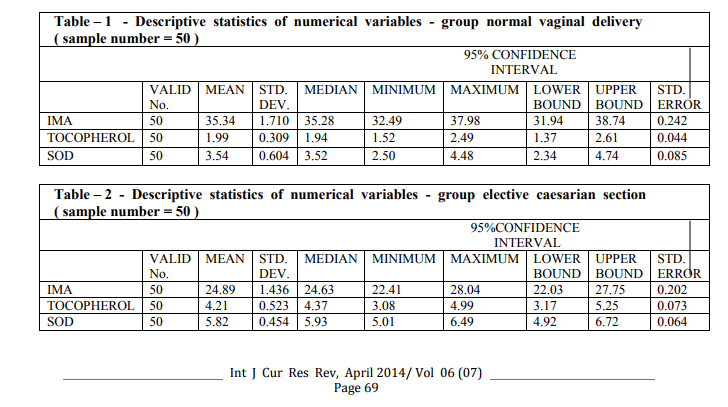
Abstract:Oxidative stress results from an imbalance between reducing agents and enzymes involved in the removal of free radicals (FR) and/or reactive oxygen species (ROS). Objective of the study was to compare oxidative stress between newborns delivered by normal vaginal delivery and elective caesarean section by estimation of cord blood ischemia modified albumin (IMA) and to compare antioxidant status between them by measuring activity of super oxide dismutase and tocopherol in their cord blood. Cord blood was collected from 50 newborns delivered by uncomplicated normal vaginal delivery and 50 newborns delivered by elective caesarean section. Mean serum ischemia modified albumin level in cord blood of newborns born by normal vaginal delivery (35.34+-3.4U/ml, mean+-2SD) was higher than serum IMA values in cord blood of newborns born by caesarean section(24.89+-2.86U/ml, mean+-2SD)( by albumin cobalt binding assay method). Mean serum tocopherol in cord blood of newborns born by normal vaginal delivery was found to be lower (1.99+-0.62mg/lit, mean+-2SD), than that of cord blood of newborns born by caesarean section (4.21+-1.04mg/lit, mean+-2SD) in this study( by Baker and Frank method). Mean cord blood plasma super oxide dismutase values were found to be lower in cord blood of normal delivery born babies (3.54+-0.60U/ml, mean+-1SD), than that of caesarean section born babies (5.82+-0.45U/ml, mean+-1SD) (by Kakkar's method). So, there is increased antioxidant status in cord blood of caesarean section born babies and increased oxidative stress (which is indicated by raised ischemia modified albumin) in cord blood of normal delivery born newborns. Antioxidant supplementation to mothers and newborns may be considered.
Keywords: Oxidative stress, Normal vaginal delivery, Elective caesarean section, Antioxidants
Full Text:
INTRODUCTION
Oxidative stress results from an imbalance between reducing agents and enzymes involved in the removal of free radicals (FR) and/or reactive oxygen species (ROS)[1]. Pregnancy, mostly because of the mitochondria rich placenta ,is a condition that favours oxidative stress .Transition metals ,especially iron, which is particularly abundant in the placenta, are important in the production of free radicals, The lungs of the newborns are especially prone to oxidative damage induced by both reactive oxygen species and reactive nitrogen species[2]. Yet these infants are often -exposed to high oxygen conc., have infection or inflammation, have reduced antioxidant defence and high free iron levels which enhance toxic radical generation, this is ‘oxygen radical diseases of neonatology’, Oxidative stress increases when more resuscitation with pure oxygen and nasopharyngeal tubing is done[3].So,at birth the newborn encounters an environment much richer in oxygen(PO2 100 TORR) than the intrauterine environment(20-25 TORR), this 4-5 fold increase exposes the newborn to a flood of free radicals[1]. The consequence of oxidative stress on foetal structure involves the activation of a complex array of genes involved in inflammation, coagulation, fibrinolysis, cell cycle and signal transduction [4]. In moderate quantities and in presence of a good antioxidant capacity, free radicals are continuously generated in the organism and are essential for cell aerobic metabolism and foetal growth, but they are toxic when overproduced, resulting in an attack on all classes of biological macromolecules, polysaccharides, nucleic acid ,lipids and proteins[5]. Hypoxia, hyperoxia, inflammation, fenton chemistry, endothelial damage, arachidonic acid cascade are other mechanisms that form highly reactive products. Free radical reactions lead to DNA damage (fragmentation, apoptosis, base modifications and strand breaks)[6]. Therefore, estimation of the antioxidant status of the newborn will help us to predict the defence mechanism of them against oxidative injury. In this study, cord blood plasma level of super oxide dismutase and cord blood serum level of alphatocopherol was measured in normal vaginal delivery group and elective caesarean section group and comparison was done to predict which group has higher antioxidant status. In this study, serum ischemia modified albumin in cord blood was measured in the above two groups and oxidative stress was compared between those two groups. Estimation of antioxidant status of the newborn in both modes of delivery leads to prediction of which mode has higher oxidative stress. In modern era, there has been a rise of caesarean section rate all over the world, this study will help to decide whether caesarean section is truly beneficial from the point of view of oxidative stress.
REVIEW
OF LITERATURE Antioxidant is any substance that when present at low concentrations compared with those of an oxidizable substrate significantly delays or prevents oxidation of that substrate. The main antioxidant defence comprises of Superoxide dismutase, Catalase, Glutathione Peroxidase (they catalytically remove free radicals and other reactive species).Super oxide dismutase converts superoxide to hydrogen peroxide and oxygen. Alpha tocopherol, retinol, Ascorbic acid, Bilirubin,Uric acid, these agents scavenge the reactive oxygen species with help of their large molecular size and presence of double bonds [7]. Ischemia/reperfusion induced oxidative stress changes the structure of the amino terminus of albumin in such a way that causes the loss of its Co2+ binding capacity leading to the formation of an ‘ischemia-modified albumin'. HPLC, LC-MS and NMR analysis have shown that the N terminal region of human serum albumin Asp-Ala-His-Lys binds the transition metals cobalt and nickel, modification of this region by way of N acetylation or the deletion of one or more amino acid resulted in no binding of cobalt, an assay that detects this reduced binding could be useful in the diagnosis of ischaemia [8]. Super oxide dismutase activity per gram haemoglobin in cord blood erythrocytes from normal term infants is significantly lower than that of red blood cells from adults. When the activity was expressed per erythrocyte no difference was found, the normocromic macrocytic red blood cells of the neonate most likely explain this discrepancy [9]. In Indian population mean cord blood SOD values is lower in preterm deliveries than full term deliveries. Increase in red cell super oxide dismutase activity in response to hypoxic stress may prevent toxic effects of O2 - radicals and oxygen toxicity to the lung [10]. Serum maternal ischemia modified albumin significantly increased during pregnancy in comparison to non pregnant controls, this may be due to physiologic oxidative stress state of pregnancy[11]. Abnormal Doppler examinations are associated with elevated ischemia modified albumin levels in complicated pregnancies where oxidative stress was more. This is higher in newborns with perinatal asphyxia as compared to healthy controls [12]. Reduced blood flow, such as that resulting from vascular compressions in complicated labor or placental ischemia, may increase IMA.IMA level in cord blood can serve as an indicator of foetal hypoxia and foetal tissue ischaemia.IMA levels in neonates from non complicated deliveries are also significantly higher than those of an adult control population, suggesting that IMA may increase as a consequence of labor,. This transient increase in IMA reflects in part transient localized tissue ischemia due to external forces exerted on foetus during the mechanism of labor during normal vaginal delivery.IMA levels in cord blood from complicated delivery neonates are 50% higher than that in neonates from uneventful deliveries, while their albumin values were not significantly different [13]. In comparison to healthy adults, newborn infants have lower levels of serum tocopherol. Tocopherol is present in significantly higher concentration in maternal plasma than in cord plasma [3]. In two separate studies done in 2000and 2005, it has been shown that route of delivery has an effect on oxidative stress in newborns exposed to oxidative stress during delivery and super oxide dismutase levels were significantly higher in the elective caesarean group than the normal vaginal delivery group [14, 15]. In 2009 a study investigated the effect of two modes of labor (vaginal delivery and elective caesarean section)on thiobarbituric reactive substances (TBARS) as markers of lipid per oxidation and oxidative stress, total antioxidant power (TAP, ferric reducing ability),and total thiol molecules (TTM) in blood of mothers and their newborns. The results indicated that mothers in vaginal delivery and their newborns are in more oxidative stress than those who underwent elective caesarean section for delivery [16]. In 2011 a study on Asian population found that malondialdehyde levels in the umbilical cord blood (which is a sensitive indicator of lipid per oxidation and thus of oxidative stress), was statistically and significantly higher in normal vaginal delivery group than those in the elective caesarean section group [17]. In 2007 a study proved that 15-f(2t)-isoprostane levels, an index of oxidative stress levels, were statistically and significantly higher in infants born after vaginal delivery compared to those delivered by elective caesarean section[18]. In 2002 a study showed the effect of delivery on umbilical cord blood gases and lipid per oxidation and observed that C.S. with epidural anesthesia is safer than NVD when lipid per oxidation were concerned[19]. In 2005, researchers investigated arterial and venous umbilical cord levels of glutathione in neonates born by vaginal delivery or cesarean section . Glutathione levels in venous and arterial umbilical samples were higher after vaginal delivery as compared to cesarean section, (P < 0.03) and (P < 0.02), respectively. These results suggest that vaginal delivery is associated with more oxidative stress than delivery by cesarean section[20]. In 2013 a study determined maternal and fetal oxidative stress levels by measuring concentrations of derivatives of reactive oxygen metabolites (d-ROMs) in umbilical artery at delivery. They also measured the pH, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2) and base excess (BE) in umbilical artery blood collected at delivery. They found that the concentrations of d-ROMs in umbilical artery were significantly higher in the VD group than the CD group. Compared to the CD group, umbilical artery pH tended to be lower (p<0.05), and BE significantly lower (p<0.005), in the VD group. There were no significant differences in umbilical artery PaO2 and PaCO2 between the two groups. They concluded that the production levels of oxygen free radicals in neonates are greater by VD than by CD[21]. In a study in 2001, lower oxidative stress was found in the newborns of the ECS group with spinal anaesthesia and higher was found in the VD group. During vaginal birth, prostaglandins and thromboxans are released to induce labour. It is known that the synthesis of these products increases lipid per oxidation. Since MDA was reported to pass from the placenta to foetal circulation, increased MDA production in the mother causes high levels of MDA in newborns. In addition, the pain and stress of mothers due to lack of anaesthesia in case of VD results in higher production of MDA[22]. On the contrary, a study in 2007 showed that the antioxidant enzyme activities were higher in the vaginal delivery group, although the differences were non significant, but the level of reduced glutathione was significantly higher in the vaginal delivery group, and vaginal born newborns exhibited lower oxidative stress and DNA damage, so there should be a strict guideline to follow before going for elective caesarean section[23]. A study in 2013, found no major difference between uncomplicated vaginal delivery and elective caesarean section[24].
Rationale
The above background shows that there is considerable difference in oxidative stress and antioxidant status in newborns born by different delivery mode, So, several research with different parameters, in different race, ethnicity, dietary habits should be done to obtain a reliable and authentic finding. In recent years, trend to deliver babies by elective caesarean section has risen, this study will help to predict whether this is beneficial or not. In a clinical trial in 2009, researchers administered antioxidant therapies and melatonin (a highly effective antioxidant and free radical scavenger) to newborns. They documented that short term melatonin therapy is beneficial to reduce foetal oxidative stress and has a remarkably benign safety profile even with pharmacological doses [25]. So estimation of antioxidant status of the newborn leads to prediction of whether intervention with diets or therapeutic antioxidant to newborns and/or pregnant females is necessary to increase the antioxidant status of the newborn.
MATERIAL AND METHODS
The study was conducted in Dept of Biochemistry and Dept of Gynaecology and Obstetrics in Medical College and Hospital, Kolkata, West Bengal, India, with approval of Institutional Ethical Committee. The study was a tertiary hospital based, non interventional, observational, comparative, cross sectional study. The study was started on January 2012 and ended on August 2013, total study duration was 18 months. 50 newborns delivered by Normal vaginal delivery and 50 newborns delivered by Elective caesarean section was randomly selected after considering inclusion and exclusion criteria and cord blood was collected. The sample size was chosen after detailed discussion with the Statistician of Medical College and Hospital, Kolkata and going through past three years record of normal and caesarean babies and mothers free of any other ailments. Patient consent was obtained from each patient who fitted the inclusion criteria.
Inclusion Criteria
Full term, mature, singleton newborns of both sexes born by NVD and ECS were included in the study after randomised selection and obtaining parental consent. All the mothers received complete pregnancy care. All of them had birth weight more than 2.5 kgs. Both the newborns and their mothers were free from complications after delivery .The APGAR score after 5 minutes was 8-10.All the mothers were normotensive, normoglycaemic, euthyroid and nonobese. Exclusion Criteria Birth weight less than 2.5 KG., APGAR score less than 8 and those who denied of informed consent for the study were excluded. Patients with a history of renal disease, diabetes, cardiac disease, hypothyroidism, hyperthyroidism, any sexually transmitted disease or significant perinatal complications, congenital anomalies or special morbidities in both mother and newborn and patients with a history of hypertension, preeclampsia, eclampsia, malignancy, history of addiction and morbid obesity were excluded. Patients taking antioxidants as medication or food supplement were excluded. Sampling technique and methods Immediately on delivery of infant, a segment of cord approx. 15-30 cm long was doubly clamped. To ensure good vessel filling, the clamp was placed on the cord close to the infant and then the cord was milked from placenta towards the 1st clamp. Subsequently a 2nd clamp was placed 10-35 cm distal to the 1st clamp. About 10 ml of cord blood was collected after cutting the cord, of which 8 ml was collected in plain vial to obtain serum,2 ml was collected in EDTA vial to obtain plasma[10]. The samples were taken to the laboratory for prompt analysis. Plasma level of super oxide dismutase was estimated by Kakkar’s method (1984)[26] , serum levels of tocopherol by Baker and Frank method(1968)[27] and serum levels of ischemia modified albumin by Albumin Cobalt binding assay[28] were estimated in cord blood.
RESULTS
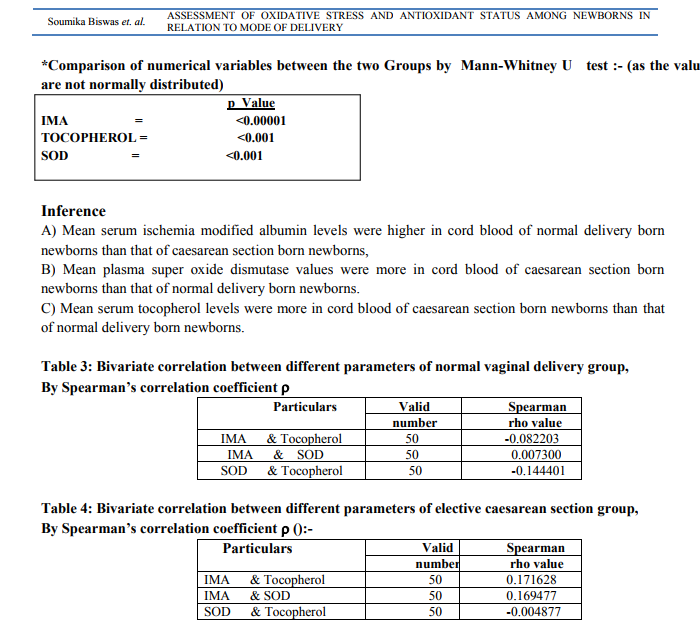
AND ANALYSIS Statistical analysis were done by Mann-Whitney U test, as the values were not normally distributed ( by Kolmogorov -smirnov goodness of fit test). After statistical analysis, it was found that ischemia modified albumin among normal vaginal delivery babies increased significantly,( p Value<0.00001). For normal vaginal delivery babies mean +/- 2SD was 35.34 +/- 1.7 U/ml. For caesarean section babies mean+-2SD was 24.89+- 2.86 U/ml. (vide table 1and 2). Super oxide dismutase in normal vaginal delivery cases (Mean+/- 2 SD =3.54+/- 0.60 U/ml) were significantly lower (p Value < 0.001), when compared to caesarean section cases (Mean +/- 2 SD =5.82+/-0.45 U/ml).(vide table 1 and 2). Serum Tocopherol levels in normal vaginal delivery cases (Mean+/- 2 SD =1.99+/- 0.31 mg/lit) were also significantly lower (p Value <0.001) when compared to caesarean section cases (Mean +/- 2 SD =4.21+/- 0.52 mg/lit). (vide table 1 and 2).
Inference
There was no significant positive or negative correlation among different parameters in both normal vaginal delivery and caesarean section group.
DISCUSSION
After completion of the present study, following salient points that merit further discussion have come to the forefront: Serum ischemia modified albumin level in cord blood of newborns born by normal vaginal delivery was higher than serum IMA values in cord blood of newborns born by caesarean section. Plasma super oxide dismutase values were more in cord blood of caesarean section born newborns than that of normal delivery born newborns and serum tocopherol levels were more in cord blood of caesarean section born newborns than that of normal delivery born newborns. This suggests that there is increased antioxidant status (super oxide dismutase and tocopherol) in cord blood of caesarean section born babies and increased oxidative stress(which is indicated by raised ischemia modified albumin) is present in cord blood of normal delivery born newborns.The studies which are in agreement with these results are of A. Gugliucci et al[13], Y.Sazzad et al[14], Inanc F et al[15], Vakilian K et al[16], S.Gulbayzar et al[17], Greco A et al[18], Pence S et al[19], M. T. M. Raijmakers et al[20], Watanabe K et al[21] and U. Mehmetoulu et al[22]. The studies which show contrary findings are Saphire O et al [24] and Z.Hracsko et al [23]. So, according to the present as well as majority of studies done in other parts of the world, caesarean section proves to be better than normal delivery, as in caesarean section the oxidative stress is less and antioxidant level is better, and there are studies which show no significant difference between normal vaginal delivery and elective caesarean section in respect to oxidative stress and antioxidant status. And there are studies which show a totally opposite finding. So, this part of the total oxidative stress which directly involves foetal outcome needs to be explored from many other angles including the social structure, the economic background, ethnicity, genetic preponderance, diet, nutritional status and susceptibility to oxidative stress. The studies regarding melatonin [25] given in newborns may show new horizon to combat oxidative stress in future and easing the management of newborn complications, though for that more such studies with larger sample size, newer and more reliable techniques are required.
CONCLUSION
The study found that there is increased antioxidant status (super oxide dismutase and tocopherol) in cord blood of caesarean section born babies and increased oxidative stress (which is indicated by raised ischemia modified albumin) is present in cord blood of normal delivery born newborns. So, the neonates born by normal vaginal delivery and elective caesarean section behave completely differently when oxidative stress and antioxidant status is concerned. This study, which was done in a tertiary care hospital in urban eastern India, may not be representative of the rest of the population. There is scope to elaborate this field with larger sample size, inclusion of different race, and with other oxidative stress parameters.
ACKNOWLEDGEMENT
All faculty members, colleagues, technicians and other stuff members of the Dept of Biochemistry and Dept. of Gynaecology and Obstetrics, all laboratory personneles, labour room personneles who helped to collect and recording of data. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
REFERENCES
1. Buonocore G,Perrone S.Biomarkers of oxidative stress in the fetus and newborn.[haematological reports] 2006; 2(10):103-107,
2. Casanova E, Viteri FE.Iron and oxidative stress in pregnancy. J Nutr 2003 May; 133(5 suppl 2):1700S-1708S,
3. Gitto E, Pellegrino S, D’Arrigo S, Barberi I, Reiter RJ.Oxidative stress in resuscitation and in ventilation of newborns. Eur Respir J 2009Dec; 34(6):1461-9.
4. Wagenaar GT, Horst SA, Van Gastelen MA,Leijser LM,Maunad T,Van der Velden PA et al .Gene expression profile and histopathology of experimental bronchopulmonary dysplasia induced by prolonged oxidative stress. Free Radical Biol Med 2004;36:782-801.
5. Halliwell B, Free radicals, antioxidants and human disease:curiosity,cause or consequence? Lancet 1994; 344:721-24.
6. Saugstad OD.Mechanisms of tissue injury by oxygen radicals: implications for neonatal disease.Acta Paediatr1996;85:1-4.
7. Halliwell B,Gutteridge JMC,1999.Free radicals in biology and medicine,3rd ed. Oxford university press Inc.New York.
8. Bar-Or D, Curtis G, Rao N. Characterization of the Co2+ and Ni2+ binding amino-acid residues of the N terminus of human albumin: an insight into the mechanism of a new assay for myocardial ischemia. Eur J Biochem.2001;268:42-47.
9. Haga P,Kran S. Ceruloplasmin levels and RBC SOD activity in small preterm infants during the early anaemia of prematurity. Acta Peadiatrica(1981);70:861-64.
10. Soumitra Chakravarty,Alka N. Sontakke.A correlation of antioxidants and lipid peroxidation between maternal and cord blood in full term and preterm deliveries.Curr Pediatr Res 2012 ;16(2):167-174.
11. Guven S,Alver A,Mentese A,Ilhan F.C.,Calapoglu,M, Unsal A.The novel ischaemia marker Ischaemia modified albumin is increased in normal pregnancies. Acta Obstet Gynaecol Scand 2009;88(4):479- 82.
12. Kumral A,Okyay E,Guclu S,Gencpinar P, Islekel GH,SS oguz,Kant M,Demirel G,Duman N,Ozkan Het al. Cord blood IMA:Is it associated with abnormal Doppler findings in complicated pregnancies and predictive of perinatal asphyxia?. Journal of obstetrics and gynaecology research 2012(Dec.):1-4.
13. Gugliucci A,Hermo R,Monroy C,Numaguchi M,Kimura S. Ischaemia modified albumin levels in cord blood: a case control study in uncomplicated and complicated deliveries. Clinica chimica acta international journal of clinical chemistry(2005);362:155-160.
14. Sazzad Y,Leonard M,Doyle M.Antioxidant levels in the cord blood of term fetus.Journal of obstetrics and gynaecology.2000;(20)No.5:468-471.
15. Inanc F,Kilinc M,Kiran G,Guven A,Kurutas EB,Cikim IG,Akyol O.Relationship between oxidative stress in cord blood and route of delivery. Fetal Diagn Ther.2005 SepOct;20(5):450-3.
16. Vakilian K,Ranjbar A,Zarganjfard A,Mortazavi M,Vosough-Ghanbari S,Mashaiee S,Abdollahi M.On the relation of oxidative stress in delivery mode in pregnant women;a toxicological concern. Toxicol Mech Methods 2009 Feb;19(2):94-9.
17. Gulbayzar S, Arica V,Hatipoglu S,Kaya A,Arica S,Karatekin G. Malondialdehyde level in cord blood of newborn infants. Iran J Paediatr 2011 September;21(3):313-319.
18. Greco A,Minghetti L,Puopolo M,Pietrobon B,Franzoi M,Chiandetti L,Suppiej A.Plasma levels of 15-F(2t)-isoprostane in newborn infants are affected by mode of delivery. Clin Biochem 2007 Dec;40(18):p.1420-22.
19. Pence S,Kocoglu H,Balat O,Balat A.The effect of delivery on umbilical arterial cord blood gases and lipid peroxides :comparison of vaginal delivery and caesarean section. Clin exp obstet gynaecol 2002;29(3):p.212-4.
20. M. T. M. Raijmakers , E. M. Roes , E. A. P. Steegers , B. van der Wildt , W. H. M. Peters.Umbilical glutathione levels are higher after vaginal birth than after cesarean section. Journal of Perinatal Medicine; Volume 31, Issue 6: Pages 520–522.
21. Watanabe K , Iwasaki A , Mori T, Kimura C, Matsushita H, Shinohara K, Wakatsuki A. Differences in levels of oxidative stress in mothers and neonate: the impact of mode of delivery. J Matern Fetal Neonatal Med. 2013 Jun 20. [Epub ahead of print]
22. Üdris Mehmetoúlu (Akkuþ),Ali Kart,Osman .Aúlayan,Metin.Apar,Recep G.K.E. Oxidative Stress in Mothers and Their Newborns in Different Types of Labour. Turk J Med Sci (2002);32: 427-429.
23. Z.Hracsko,Z.Safar,H.Orvos,Z.Novak,A.Pal,I S Varga.Evaluation of oxidative stress markers after vaginal delivery or caesarean section. in vivo 2007; 21 :703-706.
24. Saphire O,Schneid-Kofman N,Silberstein E,Silberstein T. Does mode of delivery affect neonate oxidative stress in parturition?.Arch gynaecol obstet 2013 Mar;287(3):403-6.
25. Gitto E,Pellegrino S,Gitto P,Barberi I,Reiter RJ .Oxidative stress of the newborn in the pre and postnatal period and the clinical utility of melatonin.J Pineal Res 2009 Mar;46(2):128- 39.
26. Kakkar P,Das B, Vishwanathan PN. A modified spectrophotometric assay of super oxide dismutase.Ind J Biochem Biophys1984;21:130-132.
27. Gowenlock AH,Mc Murray JR,Mc Lauchlan DM. Determination of serum tocopherol ,Baker and Frank,1968.Varley’s Clinical Biochemistry 1988:902.
28. Robert H. Christenson, Show Hong Duh. Characteristics of an Albumin Cobalt Binding Test for Assessment of Acute Coronary Syndrome Patients: A Multicenter study. Clinical Chemistry 2001;47:464-470.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





