IJCRR - 6(7), April, 2014
Pages: 26-30
Print Article
Download XML Download PDF
DELAYED DIAGNOSIS OF THE ACTUAL CAUSE FOR WHEEZE IN A LABELLED BRONCHIAL ASTHMATIC - ROLE OF ANAESTHESIOLOGIST AS A PERIOPERATIVE PHYSICIAN
Author: Dhanabagyam Govindarajulu, Vinodhadevi Vijayakumar, D.M. Mohan
Category: Healthcare
Abstract:Aim: Approach to a patient like a primary physician with meticulousness in eliciting history and evaluation, makes an anaesthesiolgist a perioperative physician. Case Report: Our patient was diagnosed to have bronchial asthma for 3 years duration and admitted with a renal malignancy. During pre operative evaluation he was found to have mediastinal widening. On further evaluation with computerized tomography, diagnosed to have retrosternal goitre compressing the trachea. Combined procedure of right nephrectomy and right hemithyroidectomy was done necessitating sternotomy. On post-operative follow up patient had no wheeze after the thyroidectomy. Discussion: The natural history of retrosternal goitre is of a slow increase in size, often presenting as an incidental finding on a chest x-ray. Patients with retrosternal/substernal goiter may not have an obvious swelling in the neck. They may present with wheeze and wrongly labelled as an asthmatic like in our patient. Late onset wheeze, persistent wheeze inspite of treatment, exertional dyspnoea, widening of superior mediastinum in chest x-ray made us to think about possible airway obstruction other than bronchial asthma for wheeze. Confirmed it to be a paratracheal, retrosternal colloid goitre. Conclusion: The late onset wheezer to be evaluated for anatomical airway obstructions. Approach to a patient like a primary physician with meticulousness in eliciting history and evaluation, makes an anaesthesiolgist a perioperative physician.
Keywords: Retro sternal goitre, Bronchial asthma, Wheeze, Mediastinal mass.
Full Text:
INTRODUCTION
The natural history of retrosternal goitre is of a slow relentless increase in size, often presenting as an incidental finding on a chest x-ray. Patients may have retrosternal/substernal goiter without obvious swelling in the neck. The majority of patients with retrosternal goiter presents with shortness of breath or asthma like symptoms.
CASE REPORT
A 64 year old male, known diabetic and bronchial asthmatic was diagnosed to have right renal cell carcinoma and posted for open right nephrectomy. He is a diabetic on oral hypoglycemic agents for 6 years, on regular follow up and good glycemic control. Bronchial asthmatic for the past 3 years on fluticasone and salbutamol inhalers. During pre-anaesthetic evaluation, physical examination was normal other than the bilateral occasional wheeze on auscultation. Airway examination revealed short neck and all other parameters were normal. Blood investigations and ECG were within normal limits. Computerized Tomography (CT) of abdomen revealed a large heterogeneously enhancing mass lesion arising from the lower half of right kidney suggestive of
DISCUSSION
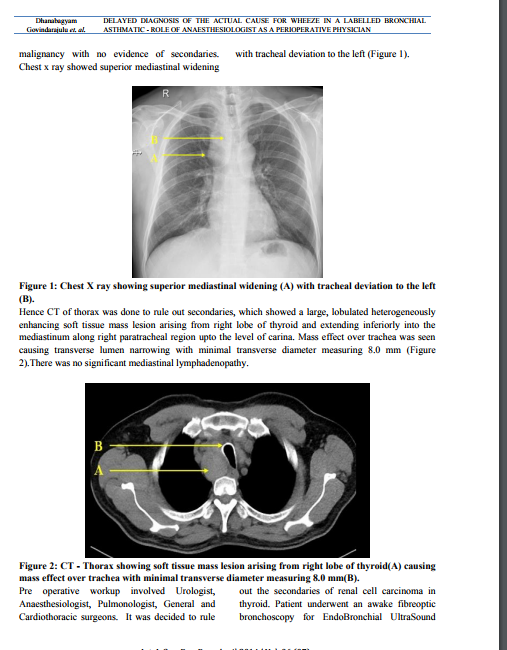
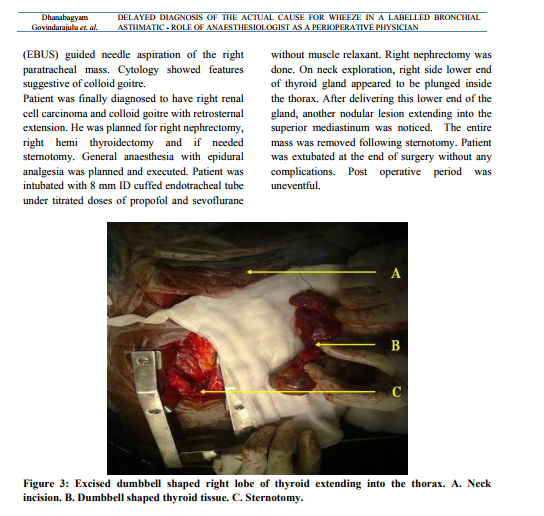
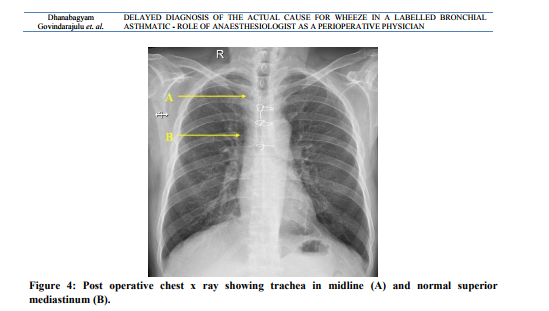
In our patient he was diagnosed to have bronchial asthma for 3 years duration and treated with bronchodilators. As he came with haematuria, dysuria and urgency, on evaluation he was suspected to have a renal malignancy by ultrasound and CT scan of the abdomen. During pre operative evaluation for anaesthesia and to rule out secondaries chest x ray was done, which showed a mediastinal widening and led us to do a CT scan of thorax. CT Thorax showed a retrosternal goitre compressing the trachea which gave us a clue for the possible etiology of his wheeze. Combined procedure of right hemithyroidectomy and right nephrectomy was done. Intraoperatively, the thyroid gland was plunging inside the thorax in the shape of dumbbell, necessitating sternotomy. Postoperative follow up revealed that the patient had no wheeze after the thyroidectomy.
Terms such as retrosternal, substernal, intrathoracic or mediastinal have been used to describe a goitre that extends beyond the thoracic inlet. However, there is a lack of consensus regarding the exact definition of a retrosternal goitre (RSG).1 The natural history of retrosternal goitre is of a slow relentless increase in size, often presenting as an incidental finding on a chest x-ray in the fifth or sixth decade of life.2 The majority of patients with retrosternal goiter presents with shortness of breath or asthma like symptoms. Other symptoms and signs include neck mass, hoarseness of voice, dysphagia or superior vena caval obstruction. Airway obstruction due to thyroid gland has been reported up to 31%3 and difficulty in intubation has been reported in 11%4. The reported incidence of substernal thyroid gland in the general population varies from 0.02 to 0.5% based on chest x-ray screening reports.5 The CT scan is the most useful tool showing the nature and extent of the lesion.6 The thyroid is usually removed through a conventional thyroid incision in the neck, but occasionally division of the upper part of the sternum is necessary. Unrecognized mediastinal goitre can produce asthma-like symptoms, which may lead to late diagnosis or misdiagnosis and deficient treatment. 7 The cause for wheeze need not be always bronchial asthma. Late onset wheeze, persistent wheeze inspite of treatment, exertional dyspnoea, widening of superior mediastinum in chest x-ray made us to think about possible airway obstruction other than bronchial asthma for wheeze. Confirmed it to be a paratracheal, retrosternal colloid goitre. Anaesthesiologist’s careful history taking, examination and evaluation have been useful to identify a curable cause for wheeze. Due to the active multidisciplinary approach, both the surgeries were done simultaneously and safely after thorough evaluation. If we would have missed it could have resulted in unanticipated difficult airway, post extubation airway issues, persistent wheeze with poor response to bronchodilators life long.
CONCLUSION
Patients with retrosternal/substernal goiter without obvious swelling in the neck can present with airway obstruction. The late onset wheezer to be evaluated for anatomical airway obstructions. Approach to a patient like a primary physician with meticulousness in eliciting history and evaluation, makes an anaesthesiolgist a perioperative physician.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. Hunis CT, Gerogalas C, Mehrzad H, Tolley NS. A new classification system for retrosternal goiter based on a systemic review of its complications and management. Int J Surg. 2008;6:71-6.
2. Mack E. Management of patients with substernal goiters. Surg Clin North Am. 1995;75:377-94.
3. Hedayati N, McHenry CR. The clinical presentation and operative management of nodular and diffuse substernal thyroid disease. Am Surg. 2002;68:245-51.
4. Amathieu R, Smail N, Catineau J. Difficult intubation in thyroid surgery: myth or reality. Anesth Analg. 2006;103:965-8.
5. Reeve TS, Rubenstein C, Rundle FF. Intrathoracic goiter: Its prevalence in Sydney metropolitan mass x-ray survey. Med J Aust. 1957;2:149-51.
6. Grainger J, Saravanappa N, D’Souza A, Wilcock D, Wilson PS. The surgical approach to retrosternal goiters: the role of computerized tomography. Otolaryngol Head Neck Surg. 2005;132(6):849-51.
7. Vadasz P, Kotsis L. Surgical aspects of 175 mediastinal goiters. Eur J Cardiothorac Surg. 1998;14:393-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





