IJCRR - 6(8), April, 2014
Pages: 57-62
Print Article
Download XML Download PDF
CLINICOPATHOLOGICAL STUDY OF BENIGN SOFT TISSUE TUMORS
Author: Venkatraman J., Rathna S.., Dhananjay S. Kotasthane, Govindaraj T.
Category: Healthcare
Abstract:Objective: \"Soft tissue' is a non epithelial extra skeletal tissue of the body exclusive of the reticuloendothelial system, glia and supporting tissue of the various parenchymal organs\"[1]. Though they can occur anywhere in the body, most commonly they involve upper and lower extremities, trunk, retro-peritoneum and head and neck [1,7]. Biological activity of these tumors varies from benign localized tumors, to benign locally aggressive, to malignant metastatic types [4]. Diagnosis of soft tissue tumors are done by standard methods like Light microscopy, special stains and immune histo chemistry [7,8,9]. This study was conducted with the aim of studying gross and microscopic features of various benign soft tissue tumors and also to correlate them clinically. Materials and methods: The incisional and excisional specimens of various soft tissue tumors were fixed in 10% neutral formalin for 24 hrs and they were subjected for routine processing and reporting. Both gross and light microscopy of the tumors were studied that included the clinicopathological features of 109 cases of soft tissue tumors between the period of May 2008 to May 2012. Results: A total number of 109 cases of soft tissue tumors were studied. Benign soft tissue tumors constituted 79.8% with a peak age occurrence in the fifth decade and showed predilection for upper extremities and lower extremities. Conclusion: Benign soft tissue tumors out number malignant tumors and it is very important to make accurate diagnosis since it has a favourable clinical outcome.
Keywords: Benign tumors, microscopy, soft tissue, lipoma.
Full Text:
INTRODUCTION
“Soft tissue' is a non epithelial extra skeletal tissue of the body exclusive of the reticuloendothelial system, glia and supporting tissue of the various parenchymal organs” [1]. Though they can occur anywhere in the body, most commonly they involve upper and lower extremities, trunk, retro-peritoneum and head and neck [1,7]. The incidence of soft tissue tumors are more when compared to the frequency of malignant ones. Benign soft tissue tumors out number malignant tumors by a margin of about 100:1 in a hospital population, and their annual incidence is approximately 300 per 100,000 population [2,3]. They can occur at any age and, like carcinomas they are more common in older patients; Malignant Soft tissue tumors occur more commonly in males than females, but gender and age-related incidences vary among the histologic types [1]. Biological activity of these tumors varies from benign localized tumors, to benign locally aggressive, to malignant metastatic types [4]. Clinical history, radiography and histopathology are the most reliable guides for making an accurate diagnosis and for predicting the clinical behaviour of the tumor. However grading of malignant soft tissue tumors are much more important in predicting the biological behaviour as well in assessing the prognosis of the tumors [5,6]. The criteria used for grading soft tissue tumors include cellularity, mitotic count, tumor differentiation and necrosis [6,7]. Diagnosis of soft tissue tumors are done by standard methods like Light microscopy of Hematoxylin and Eosin tissue sections, special stains like Masson’s trichrome, PAS and if necessary immunohistochemistry [7,8,9]. Prognosis of soft tissue tumors mainly depend on tumor size, microscopic grade, location, margins, clinical staging, DNA ploidy and genetic alterations [1,6].
SUBJECTS AND METHODS
This study was carried out during May 2008 to May 2012 in a tertiary care hospital in Pondicherry, India. All benign soft tissue tumors received in the department of pathology following surgeries are included in the study. A detailed clinical data of the patient including clinical history and histo-pathological examination of the specimen was carried out. The parameters included were the age, sex, anatomical location, clinical diagnosis and the histo-pathological features. Following surgery, the specimens were received in the Department of Pathology and gross findings like size, shape, colour and consistency were recorded. The specimens were fixed in 10% neutral formalin for 24 hrs and then 4 mm thick sections were cut from representative areas and submitted for routine processing. Sections were studied by light microscopy after H and E staining. Special stains such as periodic acid schiff, Masson’s trichrome and reticulin are done, wherever necessary. Immunohistochemical studies and the electron microscopical studies were advised in some of the soft tissue malignant tumors to support the diagnosis. The data was analyzed and compiled with help of tables, pie chart and bar diagrams. Histological subtypes were classified according to WHO classification of soft tissue tumors.
RESULTS
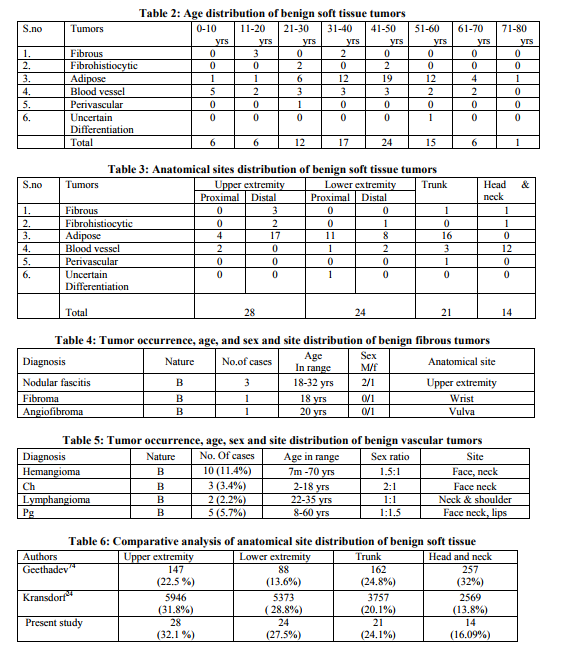
A total of 87 benign soft tissue tumors out of a total of 1010 tumors of all types were included in the present study for final analysis. Incidence Soft tissue tumors constituted 10.7% of all tumors. There were 109 soft tissue tumors in which 87 were benign. Benign soft tissue tumors constituted 79.8 % of all soft tissue tumors. The adipose tumors accounted for the majority of benign soft tissue tumors (53.2%) followed by vascular tumors (21.1%). Benign tumors of smooth muscle and tumor of skeletal muscle were not encountered in the present study (figure 1). Age and sex Benign STT’s were relatively equal in both females and males with a male to female ratio of 1:1.02(Table 1). The youngest patient in the present study was 7 months old while the oldest was 74 years old. Majority of the benign tumors occurred in the fourth, fifth and sixth decade with a peak occurrence in the fifth decade (Table 2). Size and location Benign soft tissue tumors showed a marked predilection for upper extremity followed by lower extremity and trunk in descending order of frequency (Table 3). On gross, Majority of the benign tumors (84 cases, 96.5%) were well circumscribed measuring less than 5 cm. Benign fibrous tumors The commonest benign fibrous tumor was Nodular fasciitis (3 cases, 3.4 %), which occurred, commonly in the adult age group with predilection for upper extremities. There were only one case of Fibroma and Angiofibroma and both of them occurred in females (Table 4). Venkatraman J. et. al. CLINICOPATHOLOGICAL STUDY OF BENIGN SOFT T Fibrohistiocytic tumors There were 4 cases of benign Fibrous histiocytomas (4.5%) involving commonly the upper extremity and all of them occurred in females. Adipose tissue tumors The commonest of adipose tumors were lipomas followed by lipomatosis, which showed a predilection for extremities. Benign adipose tumors are most common tumors of all STT’s (56 cases, 51.37%). Vascular tumors Benign vascular tumors were the second common tumor group (20 cases, 18.3%). Haemangiomas occurred in the first two decades thus accounting for the commonest benign soft tissue tumor of childhood. They showed a striking predilection for the head and neck region unlike other benign soft tissue tumors. Haemangioma of granulation tissue type otherwise called pyogenic granuloma occurred most commonly over the lips (Table 5).
DISCUSSION
Occurrence The commonest benign tumor type was the adipose tumor constituting 64.3 % of benign soft tissue tumors, which is in contrast to the study of Kransdorf [10] where the commonest tumor was fibrous tumor which constituted 20.6 % and the adipose tumor constituted only 16.1 % Age In the present study the age ranged from 7 months to 74 years. Which can be comparable to Tsujimoto[11] study where the age ranged from one month to 84 years. The average age in the case of benign tumors was 45 years which is comparable to the studies of M. Jensen [12]. The age range in the benign tumor group was 7 months to 73 years with a peak occurrence in the fifth decade. Size and anatomic site In the present study the commonest site was the upper extremity followed by lower extremity, which is comparable to the study of Kransdorf [10]. But in Geethadev’s study, the commonest site was the head and neck which constituted 32% followed by trunk (24.8%) [13]. The comparative analysis of anatomical site distribution of benign soft tissue tumors are shown in Table 6. On gross, Majority (96.5%) of benign soft tissue tumors were well encapsulated and presented with a size less than 5 cms while 81.3% of malignant soft tissue tumors measured more than 5 cms, which has been noted by Myhre Jensenwhere the comparative figures were 95% and 75% respectively[12]. Fibrous tumors There was one case of fibroma (1.1%) and 3 cases of nodular fasciitis (3.4%), which seem to be comparatively less than Kransdorf[10] study where they formed 2.6% and 11.3% respectively. Fibrohistiocytic There were 4 cases of benign fibrous histiocytomas, commonest site being upper extremity. The occurrence of benign fibro histiocytic tumors is less when compared to the studies of Myhre Jensenand Kransdorf[10,12]. Adipose In the present study, lipomas are the commonest of soft tissue tumors with a peak occurrence in the fourth, fifth and sixth decade, which is comparable to the studies of Myhre Jensen [12] and Kransdorf [10]. Vascular There were 20 cases of hemangiomas (11.4%) and 11 cases capillary hemangiomas (3.4%) which showed striking predilection for the Head and neck region, which was in favour of other studies [10,12,13]. Perivascular There was 1 case of benign glomus tumor with an occurrence of 1.1% of all benign soft tissue tumors. This was compared to the study of Rao et al [14] which showed female preponderance with an occurrence 1.6%. Tumors of uncertain origin There was 1 case of benign intramuscular myxoma (1.1%) occurred in 6th decade with a predilectionfor lower extremity which was comparable to the study of Theodorou et al [15]
CONCLUSION
Soft tissue tumor accounted for 10.7 % of all tumors (1010 tumors diagnosed during the study period). Benign soft tissue tumors formed 79.8 % of all soft tissue tumors. Benign soft tissue tumor showed a peak age occurrence in the fifth decade. The male to female ratio among benign soft tissue tumors was 1:1.02.The benign and intermediate soft tissue tumor showed predilection for upper extremities and lower extremities. The commonest benign tumor was lipoma (62%) of all benign tumors of soft tissue followed by vascular tumors (22.9%), fibrous tumors (5.7%) and fibrohistiocytic tumors (4.5%) in the decreasing order to frequency. The commonest benign soft tissue tumor in the first and second decade was haemangioma. From this study, it is concluded that the benign soft tissue tumors out number malignant tumors and it is very important to make accurate diagnosis since it has a favourable clinical outcome.
ACKNOWLEDGEMENT
Authors sincerely thank Dr Soumya S, Head, Dept of Pathology and DrAnand s Patil, Associate professor, Dept of Pathology, Sri Manakulavinayagar medical college, Puducherry for their constant support. Authors also acknowledge the immense help received from the scholars who articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
REFERENCES
1. Enzinger FM and Weiss SW. Soft tissue tumors. 3rd edn. Missouri: Mosby Company; 1995.
2. Rydholm A. Management of patients With soft tissue tumors: strategy developed at a regional oncology center. ActaOrthopScand Supp1203:13, 1983.
3. Rydholm A, Berg NO, Gullberg B, et al. Epidemiology of soft tissue sarcoma in the locomotor system: a retrospective population based study of the interrelationships between clinical and morphological variables. ActaPatholMicrobiolImmunol Scand 92A:363, 1984.
4. Espat NJ, Bilsky M, Lewis JJ, Leung D, Brennan MF. Soft tissue sarcoma brain metastasis-prevalence in a cohort of 3829 patients. Cancer 2002; 94:2706-11.
5. Hashimoto H, Daimaru Y, Takeshita S, Tsuneyoshi M, Enjoji M. Prognostic significance of histologic parameters of soft tissue sarcomas. Cancer 1992; 70:2816-22.
6. DreinhoferKE,BaldetorpB,AkermanM,Ferno M,RydholmA,Gustafson P.DNA ploidy in soft tissue sarcoma: comparison of flow and image cytometry with clinical follow up in 93 patients.Cytometry 2002,50:19-24
7. Fletcher CDM, Unni KK, Mertens F edn. WHO Classification of tumors of soft tissue and bone. Lyon: IARC Press 2002.
8. Espat NJ, Bilsky M, Lewis JJ, Leung D, Brennan MF. Soft tissue sarcoma brain metastasis-prevalence in a cohort of 3829 patients. Cancer 2002; 94:2706-11.
9. Tsujimoto M, Aozasa K, Ueda T, Morimura Y, Komatsubra Y, Doi T. Multivariate analysis for histologic prognostic factors in soft tissue sarcomas. Cancer 1988; 994-998.
10. Mark J Kransdorf. Benign soft tissue tumors in a large referral population: Distribution of specific diagnosis by age, sex and location. AJR1995; 164:395-402.
11. Tsujimoto M, Aozasa K, Ueda T, Sakurai M, Ishiguro S, Kurata A, et al. Soft tissue sarcomas in Osaka, Japan (1962-1985): review of 290 cases. Jpn. J. Clin. Oncol. 1988 Sep;18(3):231–4
12. Jensen M, A consecutive 7 year series 0f 1331 Soft tissue tumors-A clinicopathological data comparison with sarcomas.Actaorthopscand 1981;52:287-293.
13. Dev G, Banerjee AK, Aikat BK. Soft tissue tumors. Part I : Benign tumors. Ind J Cancer1974; 2: 336-343.
14. Rao AG, Indira D, Kamal J. Extra digital glomangioma. Indian J Dermatol. 2010 Oct;55(4):397–8.
15. Theodorou D, Kleidi ES, Doulami GI, Drimousis PG, Larentzakis A, Toutouzas K, et al. Intramuscular myxoma associated with an increased carbohydrate antigen 19.9 level in a woman: a case report. J Med Case Rep. 2011;5:184.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





