IJCRR - 6(8), April, 2014
Pages: 52-56
Print Article
Download XML Download PDF
COMPARATIVE STUDY OF HEALTH PROMOTING BEHAVIORS AMONG MANIPURI AND NORTH INDIAN STUDENTS IN CHANDIGARH, INDIA
Author: Suraj S. Senjam
Category: Healthcare
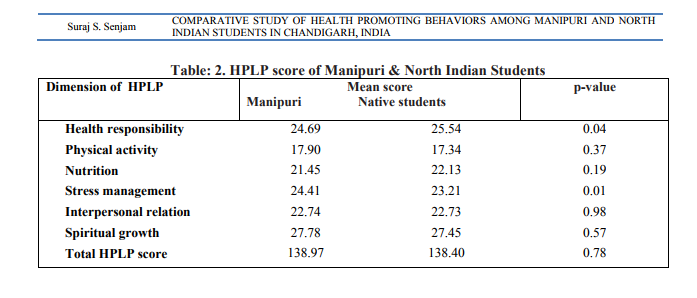
Abstract:Background: Many students from north east India mostly from Manipur have migrated to Chandigarh for further studies. It is worthwhile to know how their health promoting behaviours is different from north Indian students in Chandigarh. Objective: To compare health promoting behaviours of migrant Manipuri students and north Indian students of Chandigarh. Material and Methods: A cross sectional study was conducted in four purposively selected colleges of Chandigarh during September 2007 to June 2008. Two hundred students (Manipuri=100 and north Indian=100 with equal proportion of male and female) were studied using a self administered questionnaires of health promoting lifestyle profile (HPLP). Results and Conclusion: Local students had significantly higher sense of health responsibility than Manipuri students (24.69 vs. 25.54; p< 0.04), whereas Manipuri students had significantly higher skills or capacity for stress management than the local students (24.41 vs. 23.21; p< 0.01). Manipuri students were less concerned regarding their health than Chandigarh students. Total HPLP score was not significantly different in the two groups. Recommendation: Further research like qualitative research needs to be conducted to identify reasons for Manipuri students giving less attention on their health
Keywords: Migration & Health, Health promoting lifestyle profile, Student?s health, lifestyle.
Full Text:
INTRODUCTION
In college life, students pass through in a dynamic transitional period of growth and development. As they grow, the adolescents gradually assume responsibility for their own health1 . Their health promoting practices and behaviors not only impact their immediate health status but also have long term health consequences. It is far more difficult for adults to change unhealthy habits adopted in their youth. Many of the factors that contribute to health risks in older adults are preventable if identified and changed at an early stage of life2 . College life, thus, offers opportunities for inculcating healthy lifestyle behaviors in students. Around 700 Manipuri students are presently pursuing higher studies in Chandigarh3 . Every year, approximately 100 Manipuri students migrate to the Union Territory Chandigarh for the purpose of higher studies. Generally migrant students are likely to be different in several aspects of life from their counterparts in the receiving state. Often, they suffer from nutritional deficiencies and communication problem, social exclusion, social inequality, poverty and lack of social support or protection etc. All these factors have direct adverse health effects on students? lives4 . Against this background, the present study was conducted with an objective to compare the level of engagement in health promoting behaviors among Manipuri and north Indian graduate students of Chandigarh.
METHODOLOGY
This cross sectional study was carried out during September 2007 to June 2008 among 1st year graduate Manipuri students (MN) and north Indian students (NI) in Chandigarh in four purposively selected colleges of Chandigarh where Manipuri students were enrolled. There were 126 Manipuri students (67 male and 59 females) who enrolled in the year 2007-08 in these four colleges of Chandigarh. Of these, convenience sampling of 100 Manipuri students (50 male and 50 female) students were done. Equal numbers of north Indian native students who were in the same college and year, were also selected randomly. The sample size (N=170) was estimated based on an alpha value of ≤0.05, and power level of 0.90 for two independent groups with medium effect size of 0.505 . To be on safer side, a sample size of 200 was taken with each group of 100 students. A selfadministered questionnaire „Health Promoting Lifestyle Profile? (HPLP) was used in this study which measures health promoting behaviors. In the original HPLP questionnaire, all 52 items are scored by a fixed 4-point Likert-type format where: 1 coded as “never”, "sometimes" as 2, "often" as 3, and "routinely" as 4. The term „routinely? was chosen to represent the most frequent response category because it suggests a regular pattern of behaviors or characteristic of life-style6,7 . For the present study, requisite minor language change was done from the original items to make it understand to study population. In addition, two items which were not suitable locally, were deleted from the original HPLP. Remaining 50 items were grouped into six different subscales as original: viz. health responsibility, physical activities, nutrition habits, stress management, interpersonal relationship, and spiritual growth. Face, content and consensus validity of the tool was done with experts. Pretest was also done in 10 each of Manipuri and north Indian Chandigarh students. In analyzing health promoting behaviors, only those who reported “often” or” routinely” or similar option or those who got 3 or 4 score in each items were considered as practicing health promoting behavior and those reported “never” or “sometimes” or got 1 or 2 score were considered as not practicing the particular health promoting behaviors. The internal consistency, reliability coefficients for total scale, and subscales ranged from 0.7- 0.85. The original HPLP had reliability with internal consistency for the total score and subscale ranging from 0.7-0.92. Data were analyzed with SPSS for Windows software, version 16 (Chicga, Illinois, USA). Descriptive statistics, Chi- square test and t-test were used in statistical analysis.
Ethical clearance: Institute ethical clearance was sought before the study. A written permission was obtained from the Vice Chancellor of the Punjab University and respective colleges? principal before study. Consent of students was also taken.
RESULTS
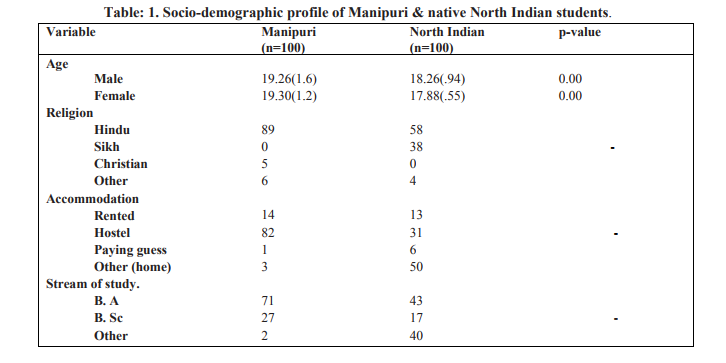
Overall, 200 students were included in the study i.e. 100 Manipuri (50 male and 50 female) and 100 north Indian Chandigarh students (50 male and 50 female). HPLP questionnaires were filled by both groups of students without missing any item. Mean age of Manipuri students was higher as compared to local students (table 1). North Indian Chandigarh students had significantly higher sense of health responsibility than Manipuri students (p=0.04; table 2). While 49% of Manipur students consulted a doctor whenever they had any health problem, 64% native students did so (p<0.05). Frequency of smoking was higher among the MN than local students. Manipuri students were more likely to undertake physical activities than that of Chandigarh students, but difference was not significant. Chandigarh students took breakfast more regularly than MN and also showed higher consumption of green leafy vegetable than MN students. Students from Manipur had significantly higher skills or capacity for stress management than the north Indian Chandigarh students (p=0.01, table 2). More MN students openly expressed their feelings to their friends about their problems than native students (67% vs. 47%; p<0.05). No significant difference was found in total score of HPLP between two groups of students.
DISCUSSIONS
Migration affects lifestyle of people. Migrants are likely to change their behaviors or lifestyle when they come to new environment. Such changes also affect young people who migrate to other cities for studies. In the present study, north Indian students of Chandigarh had comparatively better sense of health responsibility than Manipuri students. It was mainly due to higher consultation rate with doctors of Chandigarh students. Another reason is that, most of MN students stayed in hostels. They may not find it convenient to go to hospital when they fall sick. Moreover, Manipur students have language barriers as they are not fluent in Hindi. Another factor for low consultation rate among MN students may be due to easy accessibility of over-the counter-medicines. In India, procuring medicine without a prescription papers from doctors makes it easier for students to take a medicine from a chemist shop rather than paying consultation fee to doctor. In contrast, Chandigarh students live with their families. There are others family members also to look after about their health. They know the local doctors and go to them if they fall sick. Smoking rate was higher significantly both among male as well as female MN students as compared to Chandigarh students. MN students were away from their parental supervision. This might have made them free to indulge in smoking. In general, Chandigarh students culturally do not accept smoking, Moreover, in Sikh community, smoking is a taboo. Further, most of Chandigarh students stayed at home with regular parental supervision. Other studies have also reported that socially disadvantaged groups like migrant students are likely to indulge in smoking8 . MN students were more likely to engage in physical activities than Chandigarh students. This may be due to fact that exercise was a part of their culture as traditionally Manipuri are sports loving people9 . Chandigarh students were more likely to read foods labels, consumed more leafy vegetables and ate breakfast more regularly than MN students. Culturally, for most of the Manipuri, eating breakfast is not a regular routine in their native land, since people usually have their lunch usually 9-10 AM in the morning. Financial constraints faced by MN students could also be the one reason for these findings. A higher score in stress management by MN students may be a reflection of their better interpersonal relationships, and more involvement in physical activities than north Indian Chandigarh students. Manipuri students who have migrated to Chandigarh may represent a selected sample of motivated students who chose to move out from their native place and were thus ready to face problems which are likely to be there in a new environment. Moreover, mean age of Manipuri students was also higher than Chandigarh students. So, they were more likely to be mature enough to handle stress in life. Present study showed that MN students had more number of friends, and were more likely to discuss their problems with their colleagues than local students. Most MN students stayed together in hostels of their respective colleges.. Majority of Chandigarh students, in contrast, stayed at their respective homes with less chances of daily close interaction among friends. This could be the probable reason that MN students had slightly better interpersonal relationships than their counterpart local students. Moreover, living away from family may encourage closer interpersonal ties among MN students. In study across the Globe, Canadian students? showed better score in health responsibility, physical activities and interpersonal relationship subscale than Jordanian students10. Duffy et al reported that Mexican-American women had lower HPLP scores than those White groups11 . Ahijevych and Bernhard reported that total HPLP and subscale score of African-American women was lower than other groups residing in South Africa12 . Japanese students scored higher on nutrition and health responsibility subscales, whereas US students scored higher on spiritual growth and exercise subscales13 . Peltzer reported that Blacks South African avoided more fat and cholesterol, smoked less and drunk less alcohol than Whites South African, while Whites exercised more than Blacks did14 . Kerr and Ritchey reported that English-speaking migrant workers scored significantly lower on the areas of self-actualization, exercise, and stress management than their Spanish speaking counterparts15 . In our study, some of important domains of health promoting lifestyle profile were significantly different among north Indian and Manipuri Chandigarh students though overall score was similar. Manipur students gave less attention to their health and diets. They also indulged in smoking. This is matter of concerned because this will certainly reflect in students? health as well as carrier. Further research especially qualitative research may be conducted to explore the reason for their not following healthy behaviors. As the study was based on self report, it is possible that responses may be socially desirable and may not be reflect the true information.
CONCLUSION
North Indian students had a higher sense of health responsibility and more likely consulted with doctors for their health problem and ate breakfast more regularly as compared to migrant Manipuri students. Whereas, Manipuri students were more likely engaged in physical activities and outdoor games than their counterpart north Indian students. Further research is recommended to explore the reason for less consulting with and less worried about their health problem of Manipuri students. North Indian students are needed to be encouraged for outdoor games and physical exercise.
ACKNOWLEDGMENT
We would like to thank the teachers and staffs of Chandigarh colleges that were enrolled in the study for their valuable help and support during data collection. We want to acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript and also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. Terries M. Healthy lifestyle: The perspective of epidemiology. J Public Health Policy 1992;13(2):186-94.
2. Lee A, Wun Y, Chan K. Changing family medicine/general practice morbidity patterns in Hong Kong adults. Hong Kong Practitioner 1997;19(10):508-17.
3. Manipur Students? Association Chandigarh, available from http://www.msacmanipur.com (last accessed on August 2007)
4. Shaw M, Dorling D, Smith GD. Poverty, social exclusion, and Minorities: Marmot M and Wilkinson RG. Social determinant of health, 2 nd Edition. London, Oxford University Press, 2003;196-223.
5. Cohen J. Statistical power analysis for the behavioral sciences, 2nd edition. Hillsdale New Jersey, Lawrence Erlbaum Associate Publishers,1988.
6. Walker SN, Sechrist KR, Pender NJ. The Health-Promoting Lifestyle Profile: Development and psychometric characteristics. Nurs Res 1987;36(2):76-81.
7. Walker SN, Hill-Polrecky D. Psychometric evaluation of the Health-Promoting Lifestyle Profile II. In:Proceeding of the 1996 Scientific session of the American Nurse Association?s Council of Nurse Researchers 1996 June13-14 Washington (DC):p-110.
8. Martin JJ, Wardle J. Social patterning of individual health behaviors: the case of cigarette smoking. Marmot M and Wilkinson RG. Social determinant of health, 2nd Edition. London, Oxford University Press, 2003;224- 37.
9. History of Manipur –available from free encyclopedia: en.wikipedia.org/wiki/Manipur (last assessed on July 2010).
10. Haddad L, Kane D, Rajacich D, Cameron S, Al-Ma'aitah R. A comparison of health practices of Canadian and Jordanian nursing students. Public Health Nurs 2004;21:85-90.
11. Duffy ME, Rossow R, Hernandez M. Correlates of health-promotion activities in employed Mexican American women. Nurs Res 1996;25:18–24.
12. Petlzer K. Health behaviors among Black and White South Africans. Perspect Public Health 2002;122:187-93.
13. Steven RH, Hala NM, Ray MM, Marylynn BG, Takeo M. A Cross-cultural comparison of health promoting behaviors among college students. The International Electronic Journal of Health Education 2002;5:84-92
14. Ahijevych K, Bernhard L. Health promoting behaviors of African American women. Nurs Res 1996;43:86-9.
15. Kerr MJ, Ritchey DA. Health-promoting lifestyles of English speaking and Spanishspeaking Mexican-American migrant farm workers. Public Health Nurs 1990;7:80-7
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





