IJCRR - 6(8), April, 2014
Pages: 18-27
Print Article
Download XML Download PDF
A CROSS SECTIONAL STUDY ON RISK FACTORS OF TYPE 2 DIABETES AMONG SEDENTARY MALE OFFICE WORKERS
Author: Muhil S.
Category: Healthcare
Abstract:Introduction: Although many studies have focused on studying risk factors of diabetes, this study has highlighted the presence of modifiable risk factors of type 2 diabetes (T2DM) among young adults whose age range from 30 and so on. In addition to other possible risk factors, the current study has thrown a light on unhealthy waist stature ratio among office workers who spend more time as couch potatoes.
Objectives
• To describe the proportion of various modifiable and non-modifiable risk factors of T2DM among sedentary male office workers
• To explore the distribution of diabetic risk factors with respect to HbA1c categories
Material and Methods: After considering the non-modifiable risk factors such as age, gender, ethnicity and family history, the current study has addressed all possible modifiable risk factors of T2DM. Based on selection criteria, 146 office workers with the age of 30 years and above were considered for this cross sectional study.
Statistical Methods: Simple percentage and confidence interval (for large proportion) were used to describe the data.
Results: After grouping the subjects' data based on their extent of risk factors, they were categorized under HbA1c level such as normal (13%), prediabetic (65.8%) and diabetic (13%) groups. The high proportion of prediabetes (65.8%) in younger age group than older adults (8.2%) isan unusual startling finding. While considering the anthropometric factors of office workers, 73.9 % showed their waist circumference in high risk zone, 44.5% had risky waist hip ratio, 78.1% of subjects with abnormal waist stature ratio and 93.2% were above the recommended cut off value of body mass index (?23 kg/m²).
Conclusion: The current study concluded that there were 73.97% of young prediabetic subjects among sedentary male office workers which is of paramount importance as a critical health risk to the community. With a concomitant hike in sedentary lifestyle, younger adults are in the serious development of debilitating lifestyle diseases such as T2DM, heart attack, stroke and so on. Hence this study recommends a systematically designed, effective and economically feasible approach to reverse these risk factors in order to prevent or delay T2DM.
Keywords: Cross sectional study, type 2 diabetes, risk factors, sedentary and office workers
Full Text:
INTRODUCTION
Every mankind wishes to be in a comfort zone within which human feels an anxiety-neutral state. Unbelievable growth of science and technology has put forth a not an invisible but a visible trap, if it is not for all, at least for those in sedentarism. By seeking calm and stress-free environment, our physique strives hard for comfort position. Undoubtedly, people spend more time in sitting and sleeping which is really a predisposing factor of many detrimental lifestyle diseases such as diabetes, stroke, heart attack and so on. World Health Organization (WHO) and International Diabetes Federation (IDF) state that “Diabetes is a life-threatening condition, a major threat to global public health that is rapidly getting worse and its frequency is dramatically rising all over the world. The biggest impact is on adults of working age in developing countries and in many cases, diabetes can be prevented”1 . Although many studies have focused on prevalence of diabetic risk factors2-4 , the current study had explored the proportionate distribution of T2DM risk factors under the categories of glycosilated hemoglobin levels (HbA1c) among young adults whose age range from 30 years. According to IDF, in South East Asia (SEA), the proportion of mortality due to diabetes in people under 60 years of age is 55% (for the year 2013) and out of 382 million of total diabetic people in the world, SEA has 72 million which urges us to think seriously about the silently killing disease diabetes5 . Moreover, out of this 72 million, 46% are undiagnosed and as of 2013, being the second of top ten countries having diabetic citizens (20 to 79 years), India has 65.1 million diabetic people5 . Whilst considering the Tamilnadu state of India, the prevalence of total diabetes (known and unknown) is around 10.4% and 8.3% of prediabetic subjects6 . While comparing with other ethnic groups, Indians have a strong genetic susceptibility of getting diabetes and lower cut-off values of demographic and anthropometric risk factors such as 30 years of age, 90 cms of waist circumference (WC), and 0.90 cms of waist-hip ratio (WHR) and with ≥ 23 kg /m² of body mass index (BMI)7 . Surprisingly, diabetes is no longer considered as rich people’s disease; rather it has now received a notation, ‘the disease of poor’8 . Due to the impact of rapid urbanization and sedentary lifestyle, even the people from lower economic status are quietly getting into the dreadful morbidity of life style diseases like diabetes and other9 . Thus it is wise to think of reversing the modifiable risk factors since it is feasible than to treat it once it has already affected a person10. In such contemplation, as a first move to trigger primary prevention, the current study has described the proportionate existence of T2DM risk factors among office workers who spend more time in sitting posture i.e. as couch potatoes11. Objectives • To describe the proportion of various modifiable and non-modifiable risk factors of T2DM among sedentary male office workers • To explore the distribution of diabetic risk factors under HbA1c categories
MATERIALS AND METHODS
An awareness campaign was conducted for the office workers in and around Dharapuram urban area of Tamilnadu state, India who were in sitting posture in their office hours (6 to 8 hours). In order to emphasize the emerging life style diseases such as diabetes, stroke and heart attack, this study specifically targeted the employees who are being engaged in clerical and administrative work called office workers. In the current study, excluding the age, sex (male), ethnicity (Asian) and family history, all other factors considered were non modifiable risk factors12,13. Since it is well known that the males are highly susceptible to type 2 diabetes than females, the author focused 273 male office workers and they were screened for baseline assessment14. Based on the selection criteria, about 127 subjects with known history of hypertension, diabetes and regular physical activity (>2 days consecutively) were excluded and 146 office workers with the age of 30 years and above were considered for the study. The current study adopted single group cross sectional study design and the formula (Zα/2)²pq)/dwas used to calculatethe sample size (n) of the study15. Although the estimated sample size was 117, since there was a plan of administering interventions and conducting an experimental study with the same subjects in future, 146 office workers were randomly selected and analyzed for the current study. Since the study used glycosilated haemoglobin (HbA1c) level to categorize the subjects, they were grouped based on the specifications of American Diabetic Association (ADA) such as those with ≤ 5.6% were considered under normal group, 5.7% to 6.4% were in prediabetic group and diabetic group included those with 6.5% and above16. In addition to HbA1c level, all 146 subjects were screened for demographical, anthropometrical, physiological, familial and behavioral risk factors of T2DM. The anthropometric measures such as WC, hip circumference (HC), WHR and waist stature ratio (WSR) were taken based on WHO standards17. A digital weighing scale (Camry ® EF432, ISO 9001:2008 certified by SGS) was used to measure the weight of the subjects and the Blood Pressure was measured by a digital blood pressure monitor (OMRAN HM 780). Moreover details regarding family and behavioral history were noted by one to one interaction between researcher and the subjects. Subjects who had <90 cms of WC and 0.90 of WHR were grouped in low risk and rest of them were in high risk group13. The WSRof 0.5 and above was noted as high risk14. The range of BMI between 23.0 and 24.9 kg/m² was considered as overweight and the subjects who had their BMI ≥25.0 kg/m² were specified as clinically obese. Subjects with the BMI ranged from 18.5 to 22.9 kg/m² were grouped in ideal category13. Subjects who had their systolic blood pressure (SBP) between 110 to 129 mmHg and/ diastolic blood pressure (DBP) between 70 to 79 mmHg were categorized as normal. Office workers with the blood pressure between 130 to 139 mmHg and/ 80 to 89 mmHg as SBP and DBP respectively were considered in pre-hypertension group16. Whilst focusing the subjective assessment of familial and behavioral history, subjects were not involved for a detailed report on smoking, alcohol and diet knowledge since it was beyond the scope of the current study12 and 18-20. The basic knowledge on food components and their gross calorie values (High/Low) were considered to categorize the subjects on diet knowledge (Yes/No). Subjects who are not participating in regular physical activity (more than two consecutive days) were considered as sedentary21. Subjects who were sleeping less than 6 hours and more than 9 hours/day were noted as high risk group22. Statistical Methods The data of current study were described using simple percentage. Moreover the confidence interval for a large sample proportion was calculated using the following formula with 95% of confidence level to estimate the proportionate values for population. Confidence Interval (CI) is p ± Zα/2 √ (pq/n).
RESULTS
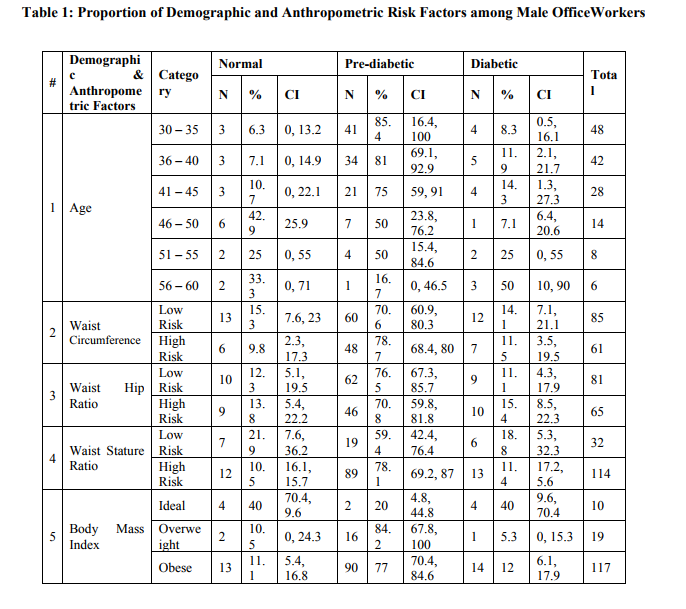
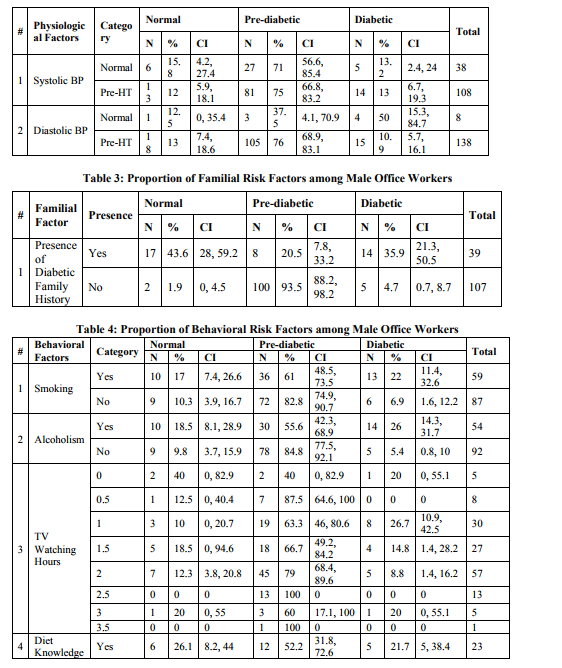
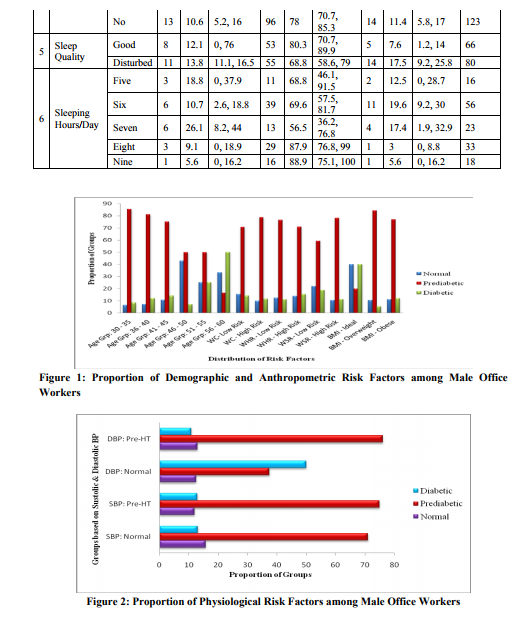
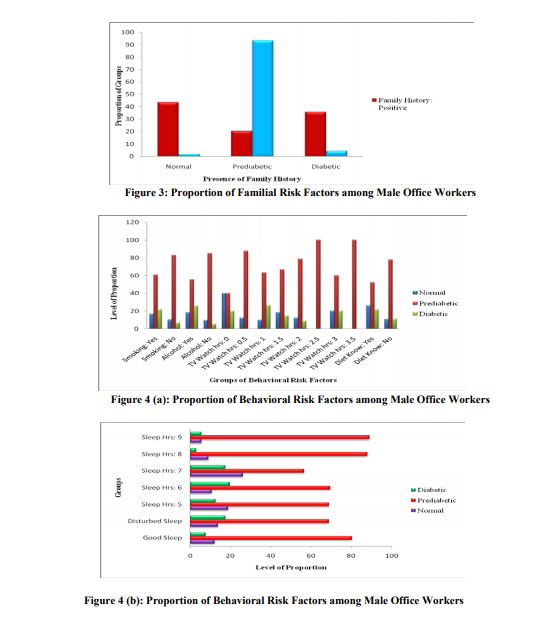
After grouping the subjects’ data based on their extent of risk factors, they were categorized under HbA1c level such as normal (13%), prediabetic (73.9%) and diabetic (13%) groups (Table 1 to 4). The high proportion of prediabetes (65.8%) in younger age group, i.e. 30 to 45 years than older adults, i.e. 46 to 60 years (8.2%) is an unusual startling finding (Table 1 and Figure 1). In the anthropometric factors, 41.8 % showed their waist circumference in high risk zone, 44.5% had risky waist hip ratio, 78.1% of subjects with abnormal waist stature ratio. 93.2% were observed under overweight and clinically obese categories ≥23 kg/m² (Table 1and Figure 1). The diagram shows the proportion of physiological factors such as systolic (73.9%) and diastolic blood pressure (94.5%) was also observed in risk zone, i.e., in prehypertensive state (Table 2 and Figure 2). Even though 73.3% of subjects showed negative family history, 73.9% of office workers were found in prediabetic category (Table 3 and Figure 3). Moreover there were 40.4% of smokers and subjects with the habit of alcohol consumption were about 36.9% (Table 4 and Figure 4(a)). The average time spent in watching television varied from half an hour to 3.5 hours per day. Among this, the subjects who spent half an hour to 3 hours time in front of television were found in prediabetic group (72.6%) (Table 4 and Figure 4(a)). In addition, 54.8% of office workers had disturbed sleep and 34.2% of subjects had had less than six hours of sleep/day where as 11% of subjects had ≥ 9 hours of sleep with prediabetes (Table 4 and Figure 4(b)).
DISCUSSION
While reviewing the findings of recent research, it is undeniably known that prediabetic subjects will develop T2DM within a decade time and specifically those who have their HbA1c level between 6 and 6.4 will develop diabetes in five years16. Moreover there are ample evidence which walk around the possibility of reversing or delaying the risk of T2DM16. Hence to reverse the prediabetic state to normal state, it is of paramount importance to explore the existence of T2DM risk factors. The current study cross matched all the possible risk factors of T2DM with three groups namely normal, prediabetic and diabetic subjects which is truly a novel approach in describing especially the sedentary male office worker population. By focusing on the demographic factor such as age, 65.8% of younger age group subjects (30 to 45 years) were found in prediabetes group, but there were only 8.6% of subjects seen between 46 and 60 years of age. The rising prevalence of T2DM risk in young age group of Tamilnadu had already been addressed by Ram Weiss et al, 200323. Out of 146 office workers, the WC of 61 subjects was found in high risk group. Further 48% of subjects who had abnormal WC were seen in prediabetic group. Likewise 46% with high risk WHR and 89% with abnormal WSR were observed in prediabetic group (Table 1 and Figure 1). Among the study group, 77% of prediabetic and 12% of diabetic group were found to be with obesity (Table 1 and Figure 1). Manisha Chandalia et al found that there was a strong association between obesity and development of type 2 diabetes24. While focusing physiological factors such as systolic and diastolic blood pressure, 75% of subjects’ SBP and 76% of subjects’ DBP were seen in prediabetic group25and26. The high proportion of prehypertension was observed by Alok K Gupta et al and also by Rekha Govindan in a different study while addressing the prevalence of prehypertension inTamilnadu. Evidence of relationship between positive family history and risk of diabetes are very obvious. In this study, 26.7% of subjects had positive family history. Aravindalochanan et al stated that subjects with positive family history were having three fold high risk of getting diabetes12. Kolappan Chockalingam stated that tobacco use prevalence was significantly higher in rural areas, slum dwellers and males18. It was observed that 17% of smokers in normal, 61% in prediabetic and 22% in diabetic category. In addition, table 4 showed that 37% of subjects with alcoholism, 19% with sedentary lifestyle, 54.8% with disturbed sleep and 11% with less than six hours and 12.3% with greater than or equal to nine hours sleep/day. The association between sleep hours, sleep quality and risk of developing type 2 diabetes had been observed by Peter M. Nilsson et al27 and also by Helaine E. Resnick et al28 in a separate study. Further Amy E. Mark et al concluded that there was an association between screen time (TV watching time) and metabolic risk factors29. The prevalence and association of BMI, decreased physical activity (sedentary lifestyle)21 and positive family history with glucose intolerance12 had been remarkably addressed.
CONCLUSION
In a nutshell, there are 73.97% of young prediabetic subjects among sedentary male office workers which has to be alerted as a critical health risk to the community. With a concomitant hike in sedentary lifestyle, younger adults are silently developing the debilitating lifestyle diseases such as type 2 diabetes, heart attack, stroke and so on. Many diabetic prevention studies have explored evidence that T2DM is reversible when serious steps are taken at the acute stage such as incorporating adequate physical activity in daily routine and behavioral modification. By highlighting the remarkable proportion of T2DM risk factors, the current study recommends a systematically designed, effective and economically feasible approach to reverse the risk factors and thereby to prevent or delay T2DM.
ACKNOWLEDGEMENT
The author is thankful for the irreplaceable mentorship and suggestions of Dr. T. Jayabal. The author is highly grateful to Mr. S. Ramesh (Chairman, Gowtham Medical Centerand Hospital, Dharapuram) who provided the study setting and helped a lot for gatheringstudy samples. In addition, the author extends his hearty gratitude to Prof. Amalraj Antony, Biostatistician and Dr. S. Arun Vijay, Director for their incredible guidance in the area of statistics. Moreover, the author acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The author is also grateful to authors, editors and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. World Health Organization and International Diabetes Federation. Diabetes Action Now: An Initiative of World Health Organization and the International Diabetic Federation. ISBN 924959151 X.
2. V. Mohan, S. Sandeep, R. Deepa, B. Shah and C. Varghese Epidemiology of type 2 diabetes: Indian scenario. Indian J Med Res 125, March 2007, pp 217-230.
3. Ambady Ramachandran, Simon Mary, Annasami Yamuna, Narayanasamy Murugesanand Chamukuttan Snehalatha. High prevalence of diabetes and Cardiovascular risk factors associated with urbanization in India. Diabetes Care 31:893–898, 2008.
4. Vipin Gupta. Type 2 Diabetes Mellitus in India. South Asian Network for Chronic Disease, New Delhi.
5. International Diabetes Federation, IDF Diabetes Atlas, Sixth Edition-2013, Page 11 – 13.
6. R. M. Anjana, R. Pradeepa, M. Deepa, M. Datta, V. Sudha, R. Unnikrishnan, A. Bhansali, S. R. Joshi, P. P. Joshi, C. S. Yajnik, V. K. Dhandhania, L. M. Nath, A. K. Das, P. V. Rao, S. V. Madhu, D. K. Shukla, T. Kaur, M. Priya, E. Nirmal, S. J. Parvathi, S. Subhashini, R. Subashini, M. K. Ali and V. Mohan. Prevalence of diabetes and prediabetes (impaired fasting glucose and/or impaired glucose tolerance) in urban and rural India: Phase I results of the Indian Council of Medical Research–INdiaDIABetes (ICMR– INDIAB) study. Diabetologia (2011) 54:3022–3027 DOI 10.1007/s00125-011- 2291-5
7. V. Mohan. Why are Indians more prone to diabetes? JAPI Vol. 52 June 2004.
8. Upendra Bhojani. The Hindu.And You Thought Diabetes is a Rich Man’s Disease. August 31 2013.
9. Steven AllenderBen Lacey, Premila Webster, Mike Rayner, Mohan Deepa, Peter Scarborough, CarukshiArambepola, ManjulaDattaandViswanathan Mohan. Level of urbanization and non-communicable disease riskfactors in Tamil Nadu, India.Bull World Health Organ 2010; 88:297–304, doi:10.2471/BLT.09.065847.
10. Sailesh Mohan, K. Srinath Reddy and D. Prabhakaran. Chronic Non Communicable Diseases in India: Reversing the Tide. September 2011
11. Pronk NP, Katz AS, Lowry M, Payfer JR. Reducing Occupational Sitting Time and Improving Worker Health: The Take-a-Stand Project, 2011. Prev Chronic Dis 2012;9:110323.
12. Aravindalochanan V, Kumpatla S, Rengarajan M, Rajan R, Viswanathan V.Risk of diabetes in subjects with sedentary profession and the synergistic effect of positive family history of diabetes.Diabetes TechnolTher. 2014 Jan;16(1):26-32. doi: 10.1089/dia.2013.0140. Epub 2013 Oct 11.
13. ICMR Guidelines for Management of Type 2 Diabetes. Section 2.Individuals for Screening, 2.1. Asymptomatic Individuals, page 5, 2005
14. Alex SF Doney, Bettina Fischer, Joanne E Cecil, Patricia TW Cohen, Douglas I Boyle, Graham Leese, Andrew D Morris and Colin NA Palmer. Male Preponderance in Early Diagnosed Type 2 Diabetes is associated with the ARE Insertion/Deletion Polymorphism in the PPP1R3A locus. BMC Genetics 2003, 4:11
15. JaykaranCharan and TamoghnaBiswas. How to calculate sample size for different study designs in medical research? Year: 2013, Volume: 35, Issue: 2, Page. 121-126.
16. American Diabetes Association. Standards of Medical Care in Diabetesd2014. Diabetes Care Volume 37, Supplement 1, January 2014
17. World Health Organization, Waist circumference and waist–hip ratio: report of a WHO expert consultation, Geneva, 8–1, December 2008, ISBN 978 92 4 150149.
18. Chockalingam K, Vedhachalam C, Rangasamy S, Sekar G, Adinarayanan S, et al. (2013) Prevalence of Tobacco Use in Urban, Semi Urban and Rural Areas in and around Chennai City, India. PLoS ONE 8(10): e76005. doi:10.1371/journal.pone.0076005
19. Vishal Khosla, K.R. Thankappan, G.K. Mini and P.S. Sarma.Prevalence and predictors of alcohol use among college students in Ludhiana, Punjab, India.Indian J Med Res 128, July 2008, pp 79-81.
20. Pratima Murthy, N. Manjunatha, B.N. Subodh, Prabhatkumar Chand and VivekBenegal. Substance Use and Addiction Research in India. Indian J Psychiatry 2010; 52:SI 89 - 99
21. American College of Sports Medicine (ACSM) Editorial, The Science of Sedentary Behavior: Too Much Sitting and Too Little Exercise
22. Jessica Goldsmith. Walla Walla UnionBulletin.Pre-diabetes a precursor, not a curse. February 2014
23. Ram Weiss, Sylvie Dufour, Sara E Taksali, WillViaTmamborlane, Kitt F Petersen, RiccardCoBonadonna, Linda Boselli,GinaBarbetta, Karin Allen, Francis Rife, Mary Savoye, James Dziura, Robert Sherwin, Gerald I Shulman and Sonia Caprio. Prediabetes in obese youth: a syndrome of impaired glucose tolerance, severe insulin resistance, and altered myocellular and abdominal fat partitioning. Lancet Vol 362 September 20, 2003; 362: 951–57
24. Manisha Chandalia, Nicola Abate, AbhimanyuGarg, James Stray-Gundersen Scott m. Grundy. Relationship between Generalized and Upper Body Obesity to Insulin Resistance in Asian Indian Men.J ClinEndocrinolMetab84: 2329–2335, 1999
25. Alok K Gupta and William D Johnson. Prediabetes and prehypertension in disease free
26. Obese adults correlate with an exacerbated systemic proinflammatory milieu. Journal of Inflammation 2010, 7:36
27. RekhaGovindan, Vikas Kumar, Dolly, Imran ShaikhGouseBasha, Rahul Kumar V and RanaRanvijay Singh.Prevalence of Prehypertension and Hypertension in Rural Tamil Nadu Populations – A Pilot Study Report from Pandithamedu of Paiyanoor Village of Kancheepuram, Tamil Nadu, India.International Journal of Emerging Trends and Technology in Computer Science (IJETTCS) -Special Issue, 2013.ISSN 2278- 6856.
28. Helaine E. Resnick, Susan Redline, EyalShahar, Adele Gilpin, Anne Newman, Robert Walter, Gordon A. Ewy, Barbara V. Howard and Naresh M. Punjabi. Diabetes and Sleep Disturbances.Diabetes care, volume 26, number 3, March 200328. Peter m. Nilsson, Mattias R, Gunnar Engstr, Bo Hedblad and 28. Goran Berglund. Incidence of Diabetes in middle-aged men is related to sleep disturbances. Diabetes Care 27:2464–2469, 2004.
29. Amy E. Mark and Ian Janssen. Relationship between screen time and metabolic syndrome in adolescents. Journal of Public Health, March 2008, Vol. 30, No. 2, pp. 153–160, doi:10.1093.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





