IJCRR - 6(9), May, 2014
Pages: 118-123
Print Article
Download XML Download PDF
STUDY OF JONE'S SPINAL INDEX AS AN INDICATOR OF NARROW LUMBAR SPINAL CANAL
Author: Rupali Sureshrao Shastrakar , Arun P. Kasote
Category: Healthcare
Abstract:The present study was carried out on 200 subjects with 100 asymptomatic control ( 50 male and 50 female) and 100 symptomatic cases( 50 male and 50 female). The symptomatic subjects were having complaints of low backache, sciatica and neurogenic claudication of more than 6 months duration. Their age group was between 30 -80 years. The aim of the study was to find out the Jone's spinal index on plain radiographs of the lumbar spine in normal and symptomatic subjects and to compare them. It was found that the lower normal limit of the Jone's spinal index was 1:2.21 which indicated a wider canal. The highest value observed in controls was 1:6.08. Jone's Spinal Index, when positive is suggestive of narrowing of the lumbar spinal canal but when negative does not exclude the possibility of narrow spinal canal
Keywords: Radiographs , Lumbar spine , Neurogenic claudication , Sciatica
Full Text:
INTRODUCTION
Low back pain resulting from degenerative diseases of the lumbosacral spine is a major cause of morbidity, disability and lost productivity. A ubiquitous and potentially disabling cause of osteoarthritic pain of the lower back and legs is stenosis of the lumbar spinal canal (Alvarez J. A., Hardy R. H.,1998). Jones R. A. C. , Salford, Thomson J. L. G. (1968), Janjua M. Z., Muhammad F. (Oct 1989) stated that Jone’s spinal index is a useful parameter in narrow spinal canal. In this study dimensions of the lumbar spinal canal were measured and Jone’s spinal index (ratio of product of transverse diameter of the canal (A) and anteroposterior diameter of the canal (B) to the product of transverse diameter of the body (C) and anteroposterior diameter of body (D) that is, AB:CD) was determined in normal and symptomatic subjects presenting with symptoms supposed to be related to narrow spinal canal by simple investigation like plain radiograph of the lumbar spine.
MATERIAL AND METHODS
The present study was carried out in the department of Anatomy at Government Medical College, Nagpur. The symptomatic subjects for the study were the patients attending the Orthopedic OPD for different complaints suggestive of narrow spinal canal. Their X-rays were taken in the Radiology department with their informed consent. Overall plain radiographs (both anteroposterior and lateral view ) of 200 subjects were included in this study
Control
Inclusion criteria:
1. Normal healthy subjects, 50 male and 50 female without any complaints suggestive of back pathology.
2. Age range between 30-80 years
.Exclusion criteria:
Subjects with significant skeletal anomalies, other problems likely to influence growth and development and younger age group (less than 19 years) were excluded to avoid lowering of the mean as lumbar spinal canal is distinctly narrower in them. ( Hink V. C., Clark W. M., Hopkins C. E. May 1966). Cases
Cases Inclusion criteria:
Symptomatic subjects aged between 30-80 years with symptoms supposed to be related to narrow lumbar spinal canal that is, 1. Chronic low back pain (more than 6 months duration), 2. Sciatica (which is defined as low back pain with radiation to one or both legs may be associated with numbness and paraesthesia) 3. Neurogenic claudication (as described by Gelderen V.,1948) and Ehni G.(Nov 1969), is characterized by leg pain, leg achiness, numbness and tingling as well as cramping and weakness, symptoms worsens with walking and distance reduces progressively
Exclusion criteria :
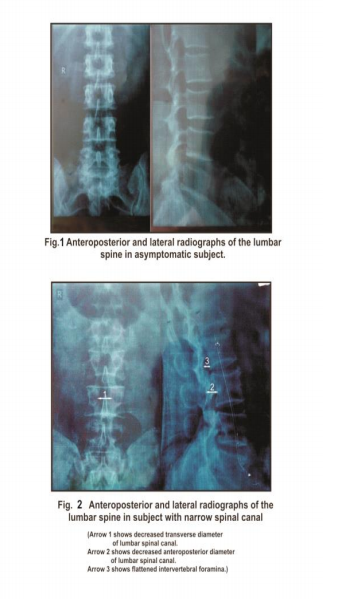
Those with short (acute) duration of complaints , absent peripheral pulses and any history of trauma or lifting heavy weight were excluded . The radiographs of the control and cases were taken in lying down position with an anode film distance of 110 cm. centered on L3 vertebra. Xrays were taken in anteroposterior and lateral views. All measurements were made by Vernier Calipers and were recorded in millimeters . Keeping in view the aims of the study ,following observations were made on x-rays: ? Transverse diameter of the lumbar spinal canal (TC) was measured as the minimum distance between the medial surfaces of the pedicles of a given vertebra (interpedicular distance). ? Antero-posterior (AP) diameter of the lumbar spinal canal (B) in lateral radiographs from middle of the back of the vertebral body to the base of the opposing spinous process, which can be recognized by tracing forwards its inferior margin. ? Transverse diameter of the vertebral body (C) was measured as the minimum distance across the waist of the vertebral body, which is between its upper and lower border. ? AP diameter of the vertebral body (D) at the level of inferior margin of spinous process. ? Canal to body ratio calculated i.e. Jone’s Spinal Index(ratio of product of transverse diameter of the canal (A) and anteroposterior diameter of the canal (B)to the product of transverse diameter of the body (C) and anteroposterior diameter of body (D) that is, AB:CD (Jones and Thomson ,1968). From above measurements mean values and standard deviation were calculated for each vertebral level.By calculating this ratio, it is possible to determine whether this individual measurements are within normal limits for respective vertebral body size or not.
OBSERVATION AND RESULTS
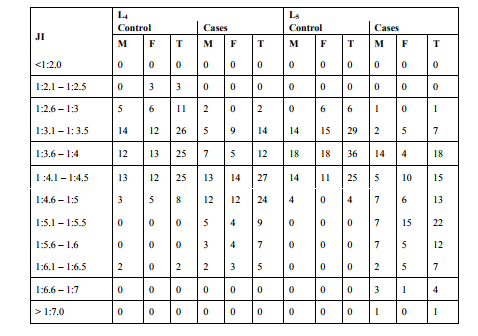
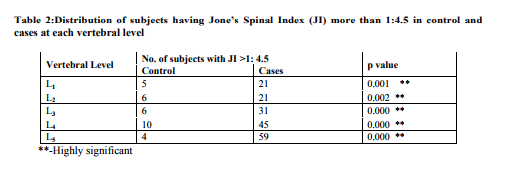
It was observed that value of Jone’s spinal index (JI) range between 1:2.0 at L4 and 1:2.5 at L5 to 1:5.5 in both male and female subjects of control and cases. .In cases the highest value observed at L4 was 1:6.5 and at L5 one value was greater than 1:7. The number of cases with value of Jone’s spinal index (JI) more than 1:4.5 when compared with number of subjects in control group were found to be highly significant at each vertebral level. Other observations on plain x rays includes varying severity of spondylotic changes in most of the symptomatic subjects. Spondylolisthesis was noted in 3 cases of symptomatic subjects.
DISCUSSION
Jone’s Spinal Index is also called as canal to body ratio(C:B)which is calculated as the ratio of product of transverse diameter of the canal (A) and anteroposterior diameter of the canal (B)to the product of transverse diameter of the body (C) and anteroposterior diameter of body(D) that is, AB:CD.

Jones R. A. C. , Salford , Thomson J. L. G. (1968), stated that, most of the normal lumbar spinal canal lie in the range of 1:2 to 1:4.5. The former ratio indicate a large canal,and the latter ratio a small canal. Janjua M. Z. , Muhammad F.(Oct 1989) stated that the normal values of the canal to vertebral body ratio (Jone’s Spinal Index) varies between 1:2 to1:5.The ratio 1:2 indicates a wider canal whereas any ratio beyond 1:5 would be conclusive of stenosis. The findings in this study were consistent with the studies of the above mentioned authors. In the study group 45 cases (45%) were having Jone’s Spinal Index more than 1:4.5 at L4 and in 59 cases (59%) at L5, suggesting a small bony canal. When spinal index was more than 1:4.5 it was suggestive of the canal stenosis, but when it was less than that, did not rule out the possibility of canal stenosis. This is because most common causes of canal stenosis includes degenerative changes in soft tissues not visualized by plain radiographs. According to Eisenstein S.( May 1977) and Naylor A. (1979) Jone’s Spinal Index is an unreliable test for assessing spinal stenosis.
CONCLUSION
Jone’s Spinal Index, when positive is suggestive of narrowing of the lumbar spinal canal but when negative does not exclude the possibility of narrow spinal canal (as narrowing of the canal in majority of cases is due to degenerative soft tissue changes)consistent with Eisenstein S.( May 1977) and Naylor A. (1979) . There are no significant differences between values of Jone’s Spinal Index of male and female cases. An advantage of Jone’s Spinal Index is that there is no need for correction regarding patients position and geometric magnification factors. These variables cancel out when the diameters of the lumbar spinal canal were related to the size of the vertebral body. Plain radiographs, it is true do not indicate the cross sectional shape of the canal, nor do they demonstrate the degree of soft tissue thickening, but various parameters used in this study can be used as an inexpensive, easy screening methods for narrow spinal canal.
ACKNOWLEDGEMENTS
We are indebted to our revered teacher and guide Dr. A. P. Kasote, associate professor , department of anatomy, government medical college , Nagpur, for his priceless guidance. We are specially obliged and thankful to our parents, family. We are grateful to technical staff in radiology department. Last but not the least, we would like to thank the almighty, who gave us the opportunity and all patients without whom, the study would not have been possible.
References:
REFERENCES
1. Alvarez J. A., Hardy R. H .( 1998) : Lumbar Spine Stenosis : A CommonCause of Back and Leg Pain. Am fam physician. Vol 15 ,57 (8), pp 1825-34, 1839-40.
2. Ehni G. (Nov 1969): Significance of the small lumbar spinal canal : Cauda equine compression syndromes due to spondylosis. J. Neurosurgery Vol 31. pp 490-494.
3. Eisenstein S. ( May 1977):The morphometry and pathological anatomy of the lumbar spine in South African Negroes and Caucasoids with specific reference to spinal stenosis. J Bone Joint Surg. Vol 59 B.2, pp 173-180.
4. Gelderen V. (1948): Ein Orthotisches (Lordotisches) Kauda –syndrome.Acta Psychiatr. Neurol.Vol 23., pp 57-68 (Quoted by reference no.19).
5. Hink V. C., Clark W. M., Hopkins C. E. ( May 1966): Normal interpediculate distances (minimum and maximum) in children and adults. American Journal of Roentgenology. Vol 97, no 1., pp 141- 153.
6. Janjua M. Z., Muhammad F. (Oct1989): Measurement of the normal adult lumbar spinal canal. J Pak Med Assoc. Vol 39 (10)., pp 264-8.
7. Jones R. A. C., Salford, Thomson J. L. G.(1968): The narrow lumbar canal. J Bone Joint Surg. Vol, 50B 3., pp 595-605.
8. Naylor A;J Bone Joint Surg. Vol 61B. 1979, pp306-309.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





