IJCRR - 6(9), May, 2014
Pages: 58-64
Print Article
Download XML Download PDF
SURGICAL MANAGEMENT OF CHRONIC SUPPURATIVE OSTEOMYELITIS OF MANDIBLE IN AN ELDERLY PATIENT - A CASE REPORT
Author: Meena Vora, Harshal Suryavanshi, Hemant Baonerkar, Chaitanya Hawaldar
Category: Healthcare
Abstract:Osteomyelitis is usually the inflammation of bone and its marrow contents. Osteomyelitis of jaw commonly occurs as a complication of dental sepsis, but it is also seen in various other situations. It is usually a polymicrobial infection. It has been associated with multiple systemic diseases including diabetes, autoimmune states, malignancies, malnutrition, and acquired immunodeficiency syndrome. Before confirmation of osteomyelitis, one should rule out tooth as source of infection. The medications linked to osteomyelitis are steroids, chemotherapeutic agents, and bisphosphonates. Different terminologies and classification systems are used, based on a variety of features such as clinical course, pathological\?anatomical or radiological features, etiology, and pathogenesis. It may be classified as acute, subacute or chronic, depending on the clinical presentation. Osteomyelitis of jaw is still a fairly common disease in maxillofacial clinics despite the introduction of new antibiotics and the improvement of dental care. The disease may occur at any age, with most common site being mandible. This is a case of an adult patient with chronic suppurative osteomyelitis (CSO), who reported to our department with pain and swelling in molar region of the mandible on right side. Here we report a case with detailed clinical, radiographical and histopathological features with differential diagnosis and treatment.
Keywords: Osteomyelitis of jaws , surgical treatment of osteomyelitis, decortication, sequestrectomy
Full Text:
INTRODUCTION
Osteomyelitis is one of the oldest diseases known to human being.(1) The word “Osteomyelitis” originates from the ancient Greek words osteon (bone) and muelinos (marrow) and means infection of medullary portion of the bone.(2) Osteomyelitis is an acute or chronic inflammatory process that can involve cortical and trabecular aspects of bone or bone marrow. The condition was originally described by Rees in 1947.(3) Osteomyelitis of jaw mainly caused by untreated odontogenic infection. Long standing infection in jaw can leads to the Chronicsuppurative osteomyelitis (CSO). It is an inflammatory reaction of bone to infection which originates from either decayed tooth, fracture site, soft tissue wound or surgical site.(4) Incidence can be aggravated with various systemic diseases. Chronic suppurative osteomyelitis is more common in mandible because of thick cortical bone and limited blood supply.(5) clinical presentation of CSO are with pain, swelling, trismus, localized pus discharge,paresthesia, warmth, erythema and tenderness.(2) CSO usually requires both medical and surgical treatment. The aim of surgery is to eliminate all of the infected and necrotic bony tissue.
CASE REPORT
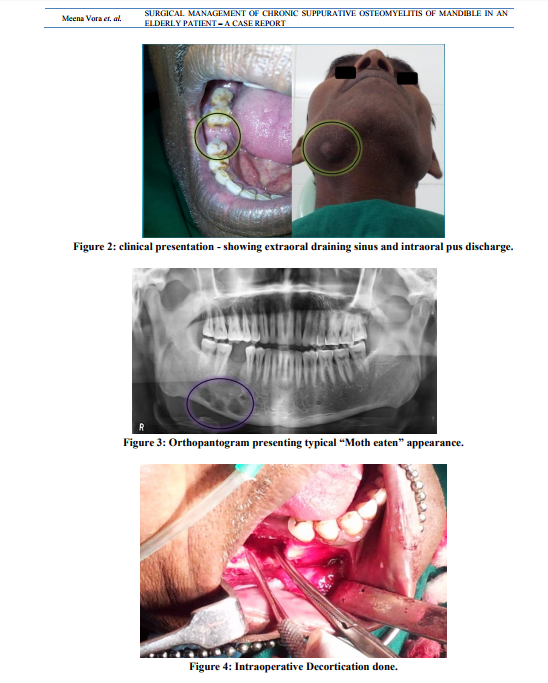
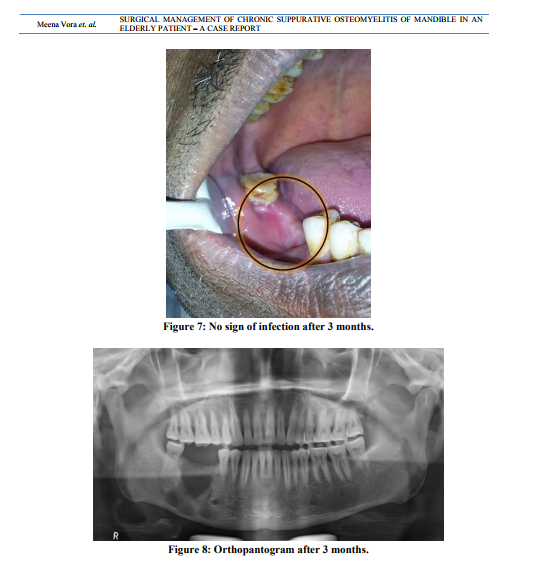
A male patient aged of 50 years was reported to our department of oral and maxillofacial surgery with chief complaint of pain and swelling in the lower right posterior region of jaw and face since past 2 months.(fig 1) He also gave the history of decreased sensory sensation over the same area. History also revealed that swelling was gradual in onset and slowly increased, but it was decreased after pus discharge. He also gave the history of extraction of lower right 1st molar 3 months back. Medical history was not contributory in this case. On extraoral clinical examination draining sinus was observed on right side of inferior border of mandible region. Cervical lymphadenopathy and regional paresthesia was also present.(fig 2) On intraoral clinical examination pus discharge was seen in extraction socket of right mandibular 1 st molar. There was mild appreciable swelling present on buccal aspect of right mandibular 2nd molar. This area was also slightly tender on palpation.(fig 2) Then patient was advised for radiological investigations. Onorthopantogram, multi locular radiolucency with ill defined borders was seen in right body of mandible, which gave presentation of typical “Moth eaten” appearance.(fig 3) Bone biopsy was also done under local anesthesia. It shows nonspecific inflammatory cell infiltration in bone. On the basis of case history, clinical and radiological finding, the provisional diagnosis as chronic suppurative osteomyelitis was made. Immediate treatment was started with empirical antibiotic (amoxicillin + potassium Clavulanic acid + metronidazole), than surgical treatment as sequestrectomy and decortication was planned. Surgery was planned under general anesthesia. Under proper surgical protocol , the pathology was exposed intra orally. Decortication was done with help of bone rongeurand rotary bone cutting instrument.(fig 4) At same time sequestrectomy and curettage was also done. Excised specimen was send to histopathology department.(fig 5) Extra orally the sinus tract was located and excised. Extra oral and intra oral suturing was done.(fig 6)Post operative antibiotic therapy was given for four weeks. Patient was well responded to both antibiotic and surgical treatment. After surgery healing over surgical area was uneventful. Histopathological report confirmed the final diagnosis as chronic suppurative osteomyelitis. Patient was kept under constant follow up. Clinically there was no sign of residual infection reported after 3 months.(fig 7)Orthopantogram was also taken after 3 months.(fig 8)
DISCUSSION
Osteomyelitis is unique jaw pathology with typical clinical and radiological presentation, but still it is challenging condition to diagnose and treat.Now a days it is less common condition due to improved nutrition, dental care and availability of newer antibiotics.Osteomyelitis may be defined as inflammatory condition of bone, that begins as an infection of medullary cavity and haversian system of the cortex and extends to involve the periosteum of affected bone.(6) It can be classify as acute, subacute, chronic, suppurative and non suppurative variant.(2)Odontogenic infection, traumatic injuries, radiations, these are main etiological factors of CSO.(4) The four primary factors which are responsible for deep bacterial invasion into the medullary cavity and cortical bone and hence establishment of the infection are number of pathogens, virulence of pathogens, local and systemic host immunity, local tissue perfusion. Pathological fracture and paresthesia are serious complications associated with osteomyelitis.(5) Our case report is typically demonstrate the features of CSO. The typical age of presentation is in the fifties to the sixties, with males more likely to be affected.(4) The commonest site is the posterior body of the mandible, because of poor blood supply and dense cortical bone.(2) Pain, fever, cheek swelling, pus discharge, exposed bone are common symptoms.(2) But progressive bone destruction and formation of sequestra are hallmark of osteomyelitis.(5) For understanding of accurate extent of bone destruction panoramic radiography, cone beam computed tomography and scintigraphy are preferred. In our case radiographic “moth eaten” appearance seen, And on histological study “inflammatory cells infiltrating in necrotic bone with loss of osteoblast” was reported which are typical presentation of CSO.(12)(6) The treatment of osteomyelitis is consider most difficult. Treatment of CSO includes antibiotic therapy, elimination of cause, incision and drainage, sequestrectomy, saucerisation, decortication, resection of jaw with reconstruction and hyperbaric oxygen.(7) Osteomyelitis is polymicrobial infection but Staphylococcus aureus and staphylococcus epidermidis are said to be primarily causative agent.(6)(8) Selecting antibiotics is based on identified bacteria from culture sensitivity test, but empirical antibiotics started as early as possible. Penicillin remain drug of choice for osteomyelitis,(2) but penicillinase resistant penicillin, clindamycin, cephalosporines are also used. Surgical management as an adjunct to medical treatment usually is necessary. The goal of surgical intervention is to disrupt the infectious foci and removal of necrotic bone or sequesra.(9) Treatment mainly involves decortication and sequestrectomy. Sequestrum is avascular, therefore poorly penetrated by antibiotics. Which leads to progression of bone destruction. Once the sequestrum has formed completely, it can be removed with a minimum of surgical trauma, which is known as sequestrectomy.(5)(6) Decortication refers to the removal of chronically infected cortex of bone. Which brings reflected buccalmucoperiostealflap closer to the medullary cavity , thus facilitate the healing process.(5)(6) Now a days medicinal and surgical treatment is combined with newer treatment such as hyperbaric oxygen (HBO) therapy, gentamycin/tobramycin beads, heaparin, streptokinase infusion, which leads to better result.(5)
CONCLUSION
We conclude our study and experience on following notes,
Early recognition of osteomyelitis and its treatment can reduce extensive loss ofbone, thereby preventing further spread of disease and possible loss of teeth. • If it is not treated can be resulting in discontinuity defect. • Associated Systemic disease should always be considered. • Culture sensitivity test plays vital role in selection of antibiotic therapy. • HBO (Hyperbaric oxygen) therapy provides better results in resistant osteomyelitis. • Risk of infection remaining in latent form should always be kept in mind.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. We also would like to thank our senior professor Late Dr.M.D.Shringarpure (MDS - oral surgery & oral radiology) for his valuable guidance during treatment of this case.

References:
REFERENCES
1. Klenerman L.A history of osteomyelitis from the Journal of Bone and Joint Surgery.J Bone Joint Surg [Br] 2007;89-B:667-70.
2. Mallikarjun K, Kohli A, Arvind K, Vatsala V, Bhayya DP, Shyagali TR.Chronic Suppurative Osteomyelitis of the mandible- A Case Report.J. Int Oral Health 2011;Volume 3 Issue 2.
3. Singh M, Singh S, Jain J, Singh KT. Chronic suppurative osteomyelitis of maxilla mimicking actinimycotic osteomyelitis: A rare case report.Natl J Maxillofac Surg. 2010 Jul;1(2):153-6
4. Yeoh SC, MacMahon S, Schifter M.Chronic suppurative osteomyelitis of the mandible: case report.Aust Dent J. 2005 Sep;50(3):200-3
5. Mamatha NS,Shah AK, Singh M, Pavan VN.Chronic suppurative osteomyelitis in a six year old boy.Journal of Health Sciences and Research,2011 Aug; Volume 2, Number 2.
6. Topazian RG, Golgberg MH, Hupp JR. Oral and maxillofacial infections. 4th ed. USA: Saunders company press; 2002 .p. 214-42.
7. Nezafati S,Ghavimi MA, Yavari AS.Localized Osteomyelitis of the Mandible Secondary to Dental Treatment: Report of a Case.J Dent Res Dent Clin Dent Prospect 2009; 3(2):67- 69.
8. Gaetti-Jardim, E. Jr. Ciesielski, F, I, N, Possagno, R, Castro, A. L,Marqueti AC, Gaetti-Jardim.Chronic osteomyelitis of the maxilla and mandible: microbiological and clinical aspects. Int. J. Odontostomat., 4(2):197-202, 2010.
9. Arunkumar JS, Naik AS, Prasad KC, Santhosh SG.Role of Nasal Endoscopy in Chronic Osteomyelitis of Maxilla and Zygoma: A Case Report.Case Reports in Medicine;Volume 2011, Article ID 802964.
10. Yanamoto S, Kawasaki G, Yoshitomi I, Mizuno A.Diffuse chronic sclerosing osteomyelitis of the mandible with synovitis, acne, pustulosis, hyperostosis, and osteitis: report of a long-term follow-up case.J Oral Maxillofac Surg. 2010 Jan;68(1):212-7.
11. Ali K, Akram A, Akhtar MU.An unusual case of chronic suppurative osteomyelitis of the mandible.Arch Orofac Sci (2012), 7(1): 37-41.
12. Shafer WG, Hine MK, Levy BM, A textbook of Oral Pathology. 4th ed. Philadelphia: Saunders; 1993: p. 498.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





