IJCRR - 6(10), May, 2014
Pages: 120-125
Print Article
Download XML Download PDF
MALIGNANT PHYLLODES TUMOUR OF BREAST WITH LIPOSARCOMATOUS DIFFERENTIATION PRESENTING CLINICALLY AS FIBROADENOMA - REPORT OF A RARE CASE
Author: Vimal Chander R., Sonti Sulochana, Madhavan M., Karuna Kumar K., Chitra S.
Category: Healthcare
Abstract:Introduction: Malignant phyllodes tumor accounts for less than 1% of breast tumors and 2 to 3% of fibroepithelial tumors of the breast. They are derived from intralobular or periductal stroma and most of them are benign. The stromal component of phyllodes tumor has the potential to undergo metaplasia to cartilage, bone, smooth muscle and striated muscle as well as their respective malignant neoplasms. The liposarcomatous differentiation of the stromal elements of phyllodes tumor is extremely rare. Case Report: We report a 27 year old female with a history of a mobile lump in the left breast presenting clinically and cytologically similar to a fibroadenoma. Histopathological examination revealed features of Malignant phyllodes tumour with liposarcomatous differentiation. Conclusion: Malignant phyllodes tumour is very rare and represents less than 1% of breast malignancies. It presents in females more than 40 years of age as a large mass. Malignant transformation is rare and heterologous liposarcomatous differentiation is unusual. This case is presented to illustrate that in a small mobile nodule of the breast presenting in young women clinically as a fibroadenoma, the possibility of a malignant phyllodes tumour should also be considered. Hence a thorough histopathological examination is necessary to rule out a malignant component. A regular follow up is needed in such cases to monitor for recurrence.
Keywords: Phyllodes tumour, Malignant, Breast tumour, Liposarcomatous
Full Text:
INTRODUCTION
Phyllodes tumour of the breast is an uncommon biphasic fibroepithelial neoplasm accounting for less than 1% of all breast tumours, the median age at the time of diagnosis being 45 years.[1,2] Phyllodes tumours are thought to be derived from intralobular or periductal stroma and may develop de novo or from fibroadenoma. Though most of them are benign, they display a morphological spectrum lying between fibroadenomas and pure stromal sarcomas. The distinction between benign, borderline and malignant phyllodes tumour is based on the assessment of a number of histological features including stromal overgrowth and atypia, cellularity, mitotic activity and infiltrative margins. Malignant transformation is seen in about 6% of phyllodes tumours, usually in the form of malignant transformation of the stroma, often showing fibrosarcomatous differentiation and rarely heterologous sarcomatous elements.[3] We present a case of malignant phyllodes tumour with stroma showing an unusual heterologous liposarcomatous differentiation in a 27 year old female.
CASE REPORT
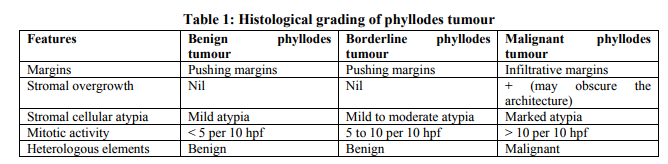
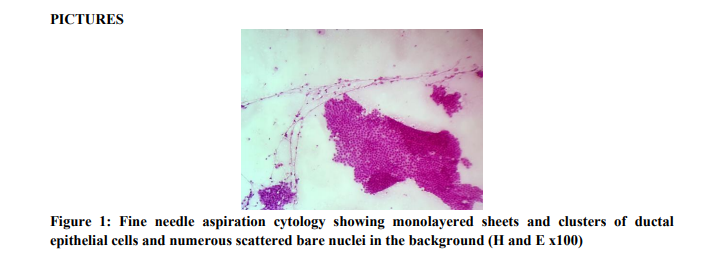
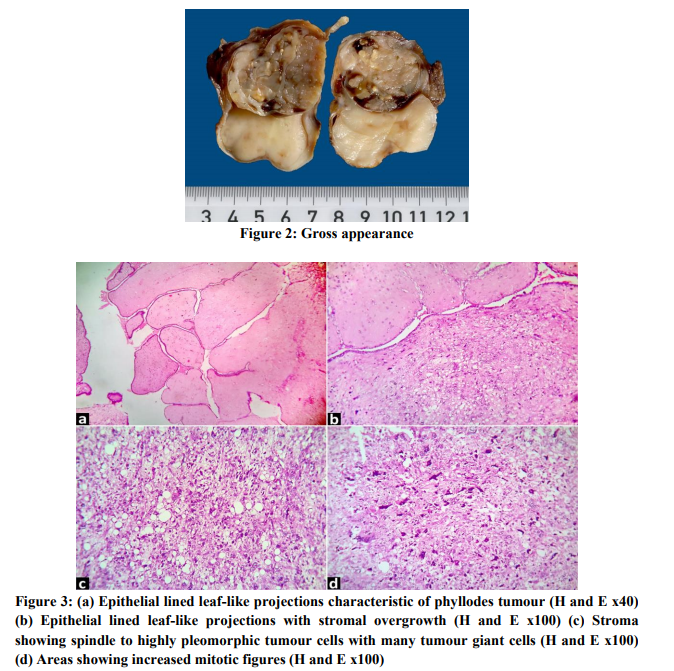
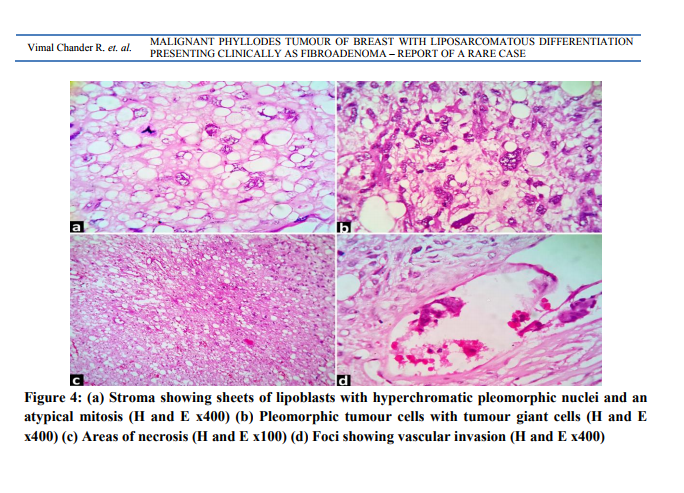
A 27 year old female presented with a palpable lump in the left breast 1 month duration. On examination, a firm mobile lump measuring 4x4 cm in the upper outer quadrant of left breast and moving freely within the breast. The overlying skin was normal. No axillary nodes were felt. A clinical diagnosis of fibroadenoma was made. Fine needle aspiration cytology showed cellular smears with benign ductal epithelial cells in monolayered sheets and clusters with interspersed myoepithelial cells and numerous scattered bare bipolar nuclei in a clean background. Occassional clusters showed cells with apocrine changes. An impression of fibroadenoma was given. [Figure 1] Later, excision biopsy was done and the specimen was sent for histopathologic examination. Macroscopic examination revealed an irregular globular soft tissue mass measuring 4x4x3 cm with cut surface showing a well circumscribed capsulated nodule which was gray white with numerous slit-like spaces. One area appeared solid and yellowish white in colour. [Figure 2] Microscopic examination showed a malignant tumour composed of both epithelial and mesenchymal components. The tumor had both solid and cystic areas with many leaf like projections lined by two layers of cells, the secretory epithelial cells and myoepithelial cells. The underlying stromal cells were spindled to highly pleomorphic containing many tumour giant cells. In some areas the tumour cells showed myxoid background with thin capillaries. Sections from the solid yellowish white areas showed few epithelial lined clefts with stromal overgrowth with sheets of univacuolated and multivacuolated lipoblasts with hyperchromatic, pleomorphic and scalloped nuclei and occassional wreath-like tumour giant cells. Mitosis was increased (more than 10 per 10 high power fields). Atypical mitoses were also seen. [Figures 3 and 4] A diagnosis of malignant phyllodes tumour with heterologous liposarcomatous component was then made. The patient is doing well and is on regular follow up for recurrence.
DISCUSSION
Malignant phyllodes tumours of the breast are rare fibroepithelial neoplasms with a potential for recurrence and metastases. They represent 1% of all breast malignancies and occur in middle aged and elderly and are relatively rare below the age of 40 years.[4] They form lobulated firm masses which may grow rapidly and cause breast enlargement with stretching of the overlying skin. In fine needle aspiration cytology, usually epithelial and stromal elements are seen. Occasionally only the epithelial component is represented in the smears, especially when there is tumour heterogeneity and hence may be mistaken for a fibroadenoma as in the present case.[5] Grossly, phyllodes tumours are relatively well circumscribed lobulated and firm with the cut surface showing a characteristic whorled pattern resembling a compressed leaf bud with visible clefts. Microscopically, they typically exhibit an enhanced intracanalicular growth pattern with leaf-like projections into dilated lumens. The epithelial element consists of clefts lined by secretory epithelial cells and myoepithelial cells. Focal epithelial hyperplasia and occasional apocrine or squamous metaplasia are known to occur in the epithelial elements, though malignant change is extremely rare. The stromal element is more cellular than a fibroadenoma and consists of spindle cells with infrequent mitosis. Occassional cases may show admixture of adipose tissue foci. It is graded into benign, borderline and malignant categories based on the histological characteristics given in Table 1.[6]
 The stromal elements in malignant phyllodes tumours usually exhibit a fibrosarcomatous differentiation. Heterologous differentiation such as chondrosarcoma, osteosarcoma, angiosarcoma, leiomyosarcoma, rhabdomyosarcoma and liposarcima are rarely encountered in malignant phyllodes tumours.[7] Liposarcomatous differentiation is extremely rare and consist of well differentiated round cell, myxoid and pleomorphic liposarcomatous components. The finding of a malignant heterologous element places the tumour into a malignant category. The finding of tumour necrosis is associated with a worse prognosis.[8,9] The clinical behaviour of malignant phyllodes tumour is difficult to predict. Liposarcomatous differentiation of the stromal component, however, does not appear to correlate with aggressive clinical behaviour. Phyllodes tumour with liposarcomatous differentiation requires complete surgical excision to prevent local tumour recurrence.[10] Hence a thorough histologic sampling of the stromal tissue is necessary for a diagnosis of malignant phyllodes tumour.
The stromal elements in malignant phyllodes tumours usually exhibit a fibrosarcomatous differentiation. Heterologous differentiation such as chondrosarcoma, osteosarcoma, angiosarcoma, leiomyosarcoma, rhabdomyosarcoma and liposarcima are rarely encountered in malignant phyllodes tumours.[7] Liposarcomatous differentiation is extremely rare and consist of well differentiated round cell, myxoid and pleomorphic liposarcomatous components. The finding of a malignant heterologous element places the tumour into a malignant category. The finding of tumour necrosis is associated with a worse prognosis.[8,9] The clinical behaviour of malignant phyllodes tumour is difficult to predict. Liposarcomatous differentiation of the stromal component, however, does not appear to correlate with aggressive clinical behaviour. Phyllodes tumour with liposarcomatous differentiation requires complete surgical excision to prevent local tumour recurrence.[10] Hence a thorough histologic sampling of the stromal tissue is necessary for a diagnosis of malignant phyllodes tumour.
CONCLUSION
Malignant phyllodes tumour is very rare and represents less than 1% of breast malignancies. It presents in females more than 40 years of age as a large mass. Malignant transformation is rare and heterologous liposarcomatous differentiation is unusual. In the present case, the age of the patient is of 27 years, the tumour size is small and the overlying skin was normal and microscopically showed features of malignant phyllodes tumourwith unusual liposarcomatous component. This case is presented to illustrate that in a small mobile nodule of the breast presenting in young women clinically similar to a fibroadenoma, a possibility of a malignant phyllodes tumour should also be considered. Hence a thorough histopathological examination is necessary to rule out a malignant component. A regular follow up is needed in such cases to monitor for recurrence.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. Argáez Cimé NL, Gutiérrez Vega P, López Cruz J. Malignant phyllodes tumor with differentiation to liposarcoma. A report of a case and bibliographic review. Ginecol Obstet Mex 2005;73:145-50.
2. Taira N, Takabatake D, Aogi K, Ohsumi S, Takashima S, Nishimura R, Teramoto N. Phyllodes tumor of the breast: stromal overgrowth and histological classification are useful prognosis-predictive factors for local recurrence in patients with a positive surgical margin. Jpn J Clin Oncol 2007;37:730-6.
3. Guerrero MA, Ballard BR, Grau AM. Malignant phyllodes tumor of the breast: review of the literature and case report ofstromal overgrowth. Surg Oncol 2003;12:27- 37.
4. Mohammed Al-Zoubaidi, Suimin Qiu, Mark Bonnen, Melissa Joyner, Kendall Roehl, Colleen Silva and Celia Chao. Malignant Phyllodes Tumor of the Breast: A Case Report. The Open Breast Cancer Journal 2011;3:45-48.
5. Mohammed Al-Zoubaidi, Suimin Qiu, Mark Bonnen, Melissa Joyner, Kendall Roehl, Colleen Silva and Celia Chao. Malignant Phyllodes Tumor of the Breast: A Case Report. The Open Breast Cancer Journal 2011;3:45-48.
6. Tan PH, Jayabaskar T, Chuan KL et al. Phyllodes tumors of the breast: the role of pathologic parameters. Am J Clin Pathol 2005;123:529-40.
7. Isotalo PA, George RL, Walker R, Sengupta SK. Malignant Phyllodes Tumor With Liposarcomatous Differentiation. Arch Pathol Lab Med 2005;129:421-2.
8. Uriev L, Maslovsky I, Vainshtein P, Yoffe B, Ben-Dor D. Malignant phyllodes tumor with heterologous liposarcomatous differentiation and tubular adenoma-like epithelial component. Int J Med Sci 2006;3:130-4.
9. Abdul Aziz M, Sullivan F, Kerin MJ, Callagy G. Malignant phyllodes tumour with liposarcomatous differentiation, invasive tubular carcinoma, and ductal and lobular carcinoma in situ: case report and review of the literature. Patholog Res Int 2010:501274.
10. Chen WH, Cheng SP, Tzen CY, Yang TL, Jeng KS, Liu CL, Liu TP. Surgical treatment of phyllodes tumors of the breast: retrospective review of 172 cases. J Surg Oncol 2005;91:185-94.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





