IJCRR - 6(10), May, 2014
Pages: 90-95
Print Article
Download XML Download PDF
MALE BREAST LESION PROFILE IN A TERTIARY CARE HOSPITAL IN WESTERN INDIA ON FINE NEEDLE ASPIRATION
Author: Raajul Jain, Smita A. Shah, Tarang B. Kadam, R. N. Gonsai, Karan Vala
Category: Healthcare
Abstract:Background: Male breast lesions are not very common. Usually male breast lesions are benign and affect the young male. Most common lesion is gynaecomastia. Male breast cancer accounts for a small proportion of breast cancers.Male breast cancer usually presents at an advanced stage. Objective: The aim of the study is to find out the incidence of male breast lesion in our setup and knowing the various pathologies afflicting male breast. Research and methodology:This is a retrospective study in which the computerised records in the department of cytopathology were analysed between January 2013 and October 2013.All breast lesions were analysed and male breast lesions were evaluated further for size, cytological diagnosis and histopathology work-up where available. Result: Most male breast lesions were benign. The most common lesion was gynaecomastia. Pre-operative diagnosis of male breast lesion in males is as desirable as in females. Cytology provides a reliable methodology for differentiating between benign and malignant lesions.
Keywords: Male breast cancer, Fine Needle Aspiration Cytology (FNAC).
Full Text:
INTRODUCTION
Male breast develops like a female breast till puberty. Due to absence of per- pubertal estrogenic stimulation, the normal male breast development ceases at this stage. Thus normal male breast mimics immature female breast1 . Breast lesions in males is relatively uncommon. A wide variation in the incidence range is seen in different geographical areas varying from 3.4 cases per 100,000 man years to 0.1 per 100,0001 . This study was undertaken to observe the prevalence and spectrum of lesions afflicting the male breast. In men, breast cancer is very rare. There are about 370 men diagnosed each year in the UK, compared with around 48,400 cases of breast cancer in women. That's about one man for every 130 women diagnosed2 . Like all cells of the body, a man's breast duct cells can undergo cancerous changes. But breast cancer is less common in men because their breast duct cells are less developed than those of women and because they normally have lower levels of female hormones that affect the growth of breast cells. The Surveillance, Epidemiology, and End Results (SEER) registry contains a total of 5,494 cases of male breast cancer and 835,000 cases of female breast cancer diagnosed from 1973 through 2005 (Anderson WF, submitted for publication).
MATERIALS AND METHODS
A retrospective study was conducted in which the computer records were collected from January 2013 to October 2013 for the patients who came to the Cytology section of
the department of Pathology of B. J. Medical College, Civil hospital, Ahmedabad, Gujarat for breast lesions. Ours is a teaching post graduate institute which also serves as a referral centre for nearby states. Data was evaluated for male patients with respect to age,site of lesion, cytology report and follow upbiopsy reports where available. Follow up biopsy was not availablein all cases as many cases were conservatively managed or were operated at a different institute.Most of the malignant cases diagnosed in our centre are referred to the Gujarat Cancer Research Institute (GCRI) and were lost to follow up. Fine needle aspiration was done with the help of 22 or 23 gauge needle, fixed in absolute alcohol and stained with haematoxylin and Eosin and Pap smears were made.The biopsy specimens were fixed in 10 % buffered formalin and paraffin embedded sections were stained with routine haematoxylin and eosin stains. No special stain or imunohistochemistry was used.
RESULTS AND OBSERVATIONS
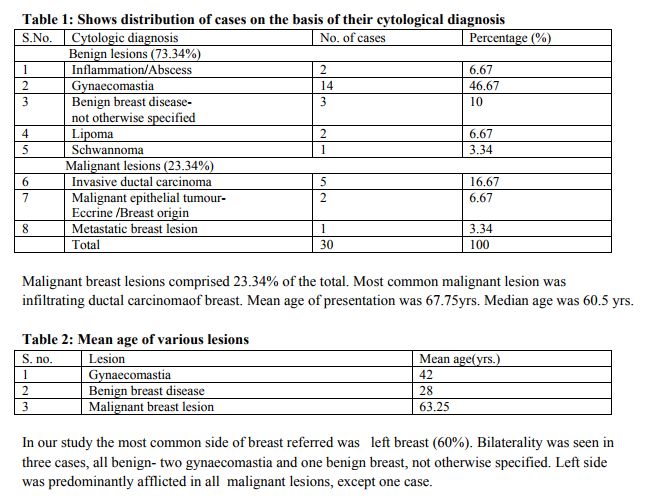
Of the total of 473 cases 30 were cases of male breast lesions. Male breast lesions comprised 6.34% of the total breast lesions. The age group of presentation was between 13-100 yrs. Most common age group is 30-50 yrs. Majority of lesions were benign.The most common lesion was gynaecomastia (46.67%). Mean age of presentation was 41.5yrs. Median age of presentation was 40 yrs.
 DISCUSSION
DISCUSSION
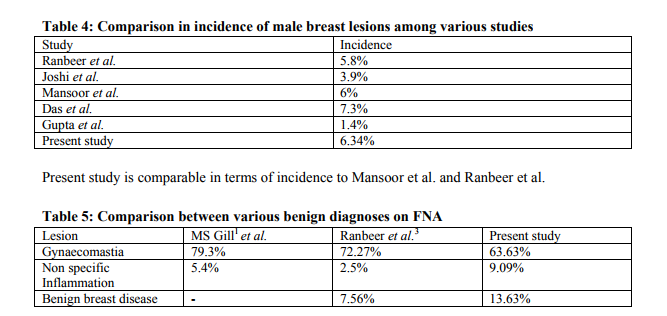
Diagnosis of breast lesions by fine needle aspiration cytology has gained worldwide recognition3 . The present study evaluated 30 male breast lesions. 6.34 % cases of breast lesions in our study were found to be in males. The incidence reported byRanbeer etal.3 is 5.8 %. In the study by Joshi et al. 4 incidence is 3.9%. Mansoor et al. 5 (Saudi Arabia) reported an incidence of 6%, Gupta et al. 6 reported an incidence of 1.4% while Das et al. 7 reported an incidence of 7.3%
Gynaecomastia is the predominant benign lesion in both the other studies and also in the studies by Joshi4 , Mansoor5 , Gupta6 , Das7 and Bannayan8 .The study by MS Gill et al. did not classify diseases as benign breast lesion which may be responsible for its such a high incidence. In our institute gynaecomastia was seen in the age group of 30-50 yrs. Gynaecomastia is caused by transitory hormone changes, as in puberty, often regresses after 1- 2 yrs. These factors share
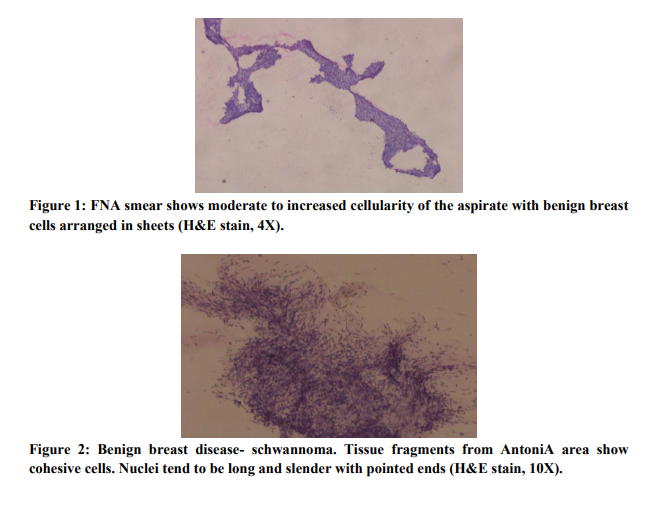
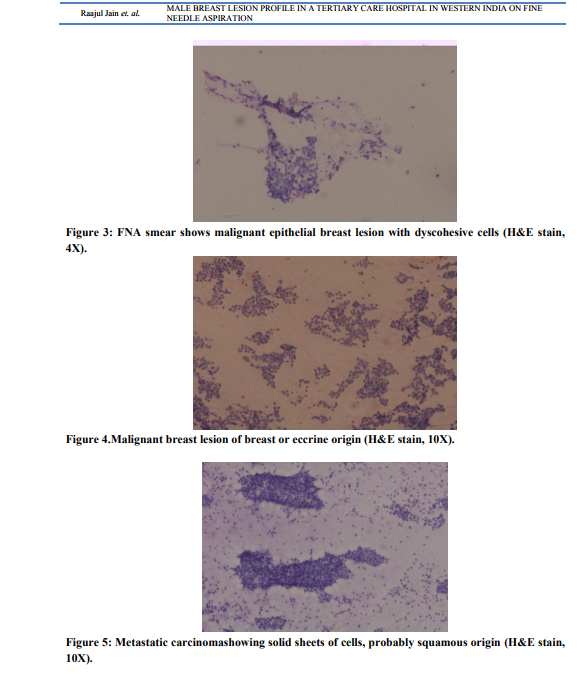
in common increased estrogenic activity or decreased testosterone activity or both8 . The aetiopathological factors causing the gynaecomastia in adolescents are weight gain and fat deposition in the breast area, estrogen androgen imbalance in puberty, psychological stress, hypogonadism or abnormalities of pituitary(loss of blood supply, infection, steroid producing tumours), systemic causes such as adrenal genital syndrome, cirrhosis, renalfailure, thyrotoxicosis(estrogen and testosterone binding changed) or congenital (Klinefelter syndrome, androgen resistance etc.) or idiopathic8 . Causes of gynaecomastia in later years may be hormonally active tumours(Leydig cell tumour of testes, hCGsecreting germ cell tumours, lung carcinoma or others), cirrhosis, medications (digitalis, reserpine, dilantin and others) or idiopathic9 . Fine needle aspirates of gynaecomastia can have variable cellularity ranging from virtually acellular to richly cellular smears. Virtually acellular smears were seen in more mature lesions, where sclerosis had over taken proliferation. Duct cell clusters, myoepithelial cells and stromal cells were the three main components found in the smears7 . One very important clue is epithelial cohesiveness in these clusters which differentiate highly cellular smears with atypia from malignant lesions10,11 . The lesions where only benign cells were seen in a dispersed manner were termed as benign breast disease not otherwise specified. Male breast or chest wall lipoma is also seen which is similar to lipoma at any other location with variably cellular smear with fat cells. Schwannoma in breast is rare, accounting for 2.6% of schwannomas12. There are less than 30 cases reported in literature. Male breast schwannoma is rarer. Schwannoma is characterized cytologically by Antoni A areas which are fragments of cohesive cells. Samples from Antoni B areas often show mainly dispersed cells and myxoid at times cystic background. The most typical characteristicis the fibrillary appearance of the intercellular stroma. Nuclei tend to be long andslender with pointed ends often with a curved appearance11 . The male breast cancer were easily distinguished on cytology from gynaecomastia on the basis of high cellularity, dyscohesive cell groups with nuclear piling and anisonucleosis10.The absence of bipolar nuclei is an important clue in diagnosis of malignant lesions. In our study the follow up could not be possible in all cases because of the patients being referred to the cancer hospital.
CONCLUSION
Cytology provides good pre operative methodology for diagnosis in male breast cancer. Judicious use of cytology can minimise biopsies and frozen sections in case of male breast lesions.
\
References:
REFERENCES
1. Gill MS, Kayani N, Khan MN, Hasan HS. Breast diseases in males- A morphological review of 150 cases.J Pak Med Assoc 2000;50;177-179.
2. “Breast Cancer in Men”. Cancer Research UK. 2007. Retrieved 2010-05-14.
3. RanbeerSingh, Anshu, Satish M. Sharma, NitinGangane. Spectrum of Male Breast lesions Diagnosed by Fine Needle aspiration Cytology: A 5- Year Experience at a Tertiary Care Rural Hospital in central India.DiagnCytopathol,Vol 40(2):113-117.
4. Joshi A, Kapila k, VermaK.Fine Needle Aspiration Cytology in the Management of Male breast Masses-Nineteen years of experience.ActaCytologica 1999;43:334-338.
5. MansoorI, Jamal A. The value of fine needle aspiration cytology in the diagnosis of male breast lesions. Kuwait Med J 2001;33:216- 219.
6. Gupta RK,Naran S, Dowle CS, Simpson JS. The diagnostic impact of needle aspiration cytology of the Breast on decision making with an emphasis on the aspiration diagnosisof male breast masses. DiagnCytopathol 1991; 7:637-639.
7. Das DK, Junaid TA, Mathews SB, Ajrawi TG, Ahmed MS, Madda JP. Fine needle aspiration cytology diagnosis of male breast lesions: A study of 185 cases. ActaCytol 1995; 39:871-876.
8. Bannayan GA, HajduSI.Gynaecomastia: Clinicopathologic study of 351 cases. Am J ClinPathol 1992; 57:431-437.
9. Coen P, Kulin H. Ballantine T, etal.An aromatase producing sex cord stromal tumour resulting in prepubertalgynaecomastia.NEngl J Med 1991; 324:317-322.
10. Bibbo M, Lang WR, Silverman JF.Breast. In: Bibbo M, editor.Text book of comprehensive cytopathology. 2nd ed. Philadelphia: W B Saunders Company; 1997.p 750-752.
11. Orell SR, Sterrett GF, Walter Max N-I, Whitaker D.Breast. In: Orell SR, Sterrett GF, Walters M N-I, Whitaker D, Lindholm K, editors. Manual and atlas of fine needle aspiration cytology.3rd ed. London: Churchill Livingstone; 1999.p 188-189.
12. VandanaDialani,Neely Hines, Yihong Wang, Priscilla Slanetz.Breast Schwannoma. Case Reports in Medicine;2011.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





