Introduction
Situsinversus anomaly is the mirror image transposition of the thoracic and abdominal organs around the midline with multiple variants[1]. Situsinversus totalis includes dextrocardia representing the complete extreme variant of the spectrum[1, 2].This spectrum could be associated to renal anomalies like horseshoe kidney which is the commonest renal fusion anomaly with an isthmus connecting the lower poles. However, situsinversus with levocardia or isolated levocardia is an extremely rare variant [1, 3]. The heart is seen in its normal levo position in the chest, while the abdominal viscera are in the dextro position [1, 4, 5]. It is mostly associated to congenital heart defects [1]. Few cases without major heart anomalies lived long [6, 7]. So, the diagnosis of the combination of situsinversus anomalies to horseshoe kidney and management of its overt cases are challenging[8]. This article describes a rare case of horseshoe kidney complicated by bilateral stones in a patient with situsinversus with levocardia and skeletal anomalies.
Case report
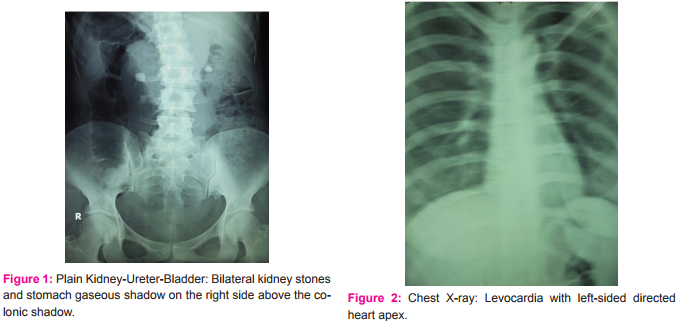
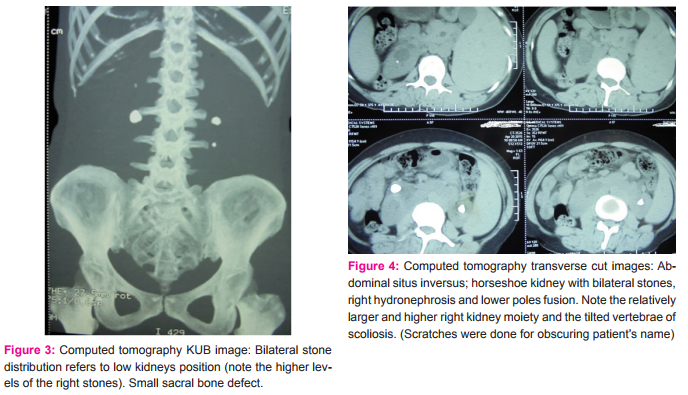
A 41-year-old female patient presented by right loin pain of many months duration. She was single with no previous significant medical or urological history. On examination, she was tall, and generally looked healthy. Abdominal ultrasound revealed liver and spleen transposition, bilateral kidney stones, mildly dilated right kidney pelvicalyceal system and malrotation. Also, Kidney-Ureter-Bladder imaging films showed bilateral dense kidney stones with right lumbar scoliosis and right-sided small sacral bone defect (Figs. 1 and 3). Chest X-ray showed the heart in the normal left-sided position and so its apex direction (Fig. 2). Transverse cuts of the non-contrast computed tomography of the abdomen confirmed the diagnosis of situsinversus of the abdominal organs, horseshoe kidney with its isthmus and mildly dilated right pelvicalyceal system, tilted vertebrae of scoliosis, and nephrolithiasis (Fig. 4). Both kidney moieties were low in position and the right one was relatively higher and larger than the left (Figs. 3 and 4). In the right moiety, computed tomography described two stones; pelvic (16 mm x 14.6 mm) and upper calyx (3 mm x 2 mm). Also, there were two left stones; pelvic (11.4 mm x 9.7 mm)and lower calyceal (3 mm x 3 mm) stones (Fig. 3 and4). The average Hounsfield Unit values of the right and left kidney stones were 604 and 610, respectively. Examination revealed no upper respiratory tract disorders. Also, she was virgin and the gynecological evaluation was irrelevant. Cardiac evaluation by electrocardiogram and echocardiography revealed normal findings.
The patient was counseled for the anomalies and the possible lines for stones treatment which were extracorporeal shock wave lithotripsy and percutaneous nephrolithotripsy. She preferred shock wave lithotripsy to percutaneous nephrolithotripsy. Considering the anatomical challenges of situsinversus, scoliosis and the mild degree of hydronephrosis, I agreed to this preference as an initial option. Unfortunately, two sessions of shock wave lithotripsy failed to affect right side stone topography. So, percutaneous nephrolithotripsy was scheduled. However, the patient seemed to be unconvinced with this decision and she did not fit for the date of operation.
Discussion
Etiology of situsinversus anomalies was attributed to the biological expression of a certain protein that affects the heart looping during embryogenesis. Mostly, it has an autosomal recessive inheritance pattern [2]. Organ situsanomalies represent a spectrum and classified into situssolitus (the normal variant), situsinversus totalis (the commonest), situsinversus with levocardia, isolated dextrocardia and situs ambiguous [1].
Horseshoe kidney is a fusion anomaly with a reported incidence of 0.25% [9]. It is attributed to the abnormal migration of the posterior nephrogenic cells. However, mechanical forces may have a role in the anatomical orientations of the horseshoe kidney including the relatively low position and malrotation[10]. The typical anatomical findings were described and illustrated in the present case.
The urologist may meet situsinversus anomalies as an association to one of the following genitourinary disorder categories; congenital disorders only[10, 11], acquired disorders only [8], combination of congenital and acquired disorders[12] or without any disorders like in living kidney donation[13].
The present case belonged to the combined disorders category. Coincident combination of the multiple unrelated rare anomalies is very rare medical situation [10]. Therefore, further congenital or acquired disease combinations usually attribute to extremely rare situations. This could be applied to the current combination of situsinversus with levocardia, skeletal anomalies, and horseshoe kidney which was complicated by nephrolithiasis and hydronephrosis. Moreover, an extremely rare feature in this case of situsinversus with levocardia is the absence of the congenital heart defects which were reported up to 100% ofcases [1]. Similarly, Imamura et al. [3] and Jo et al. [5]reported single cases of this variant without congenital heart defects in adults. Only, few cases of situsinversus with levocardia were reported with urological disorders including adrenal adenoma [7] and micropenis[3]. However, similar presentations to the current case included cases of horseshoe kidney and the common variant situsinversus totalis combined to cilia defects syndromes like Kartagener syndrome [12], or combined to Klippel-Feil syndrome. These syndromes consist of the heart anomalies, skeletal anomalies including scoliosis and renal anomalies including the horseshoe kidneys[14].
Association of situsinversus to nephrolithiasis is a rare finding[15]. Moreover, association of horseshoe kidney/situsinversus combination to nephrolithiasis could be detected very rarely in publications [2]. Accordingly and again, addition of a common congenital or acquired disorder to a rare anomaly, solely or in combinations, will create a rare situation too. The evidence evolves from the literature, where nephrolithiasis is common with horseshoe kidney reaching up to 60% [9], but it is rarely reported in combinations of situsinversus and horseshoe kidney[2].
Anatomical and metabolic abnormalities of horseshoe kidney predispose to nephrolithiasis[9]. In such cases, shock wave lithotripsy is the preferred treatment method for small stones (≤15 mm), while percutaneous nephrolithotripsy is the standard line of treatment for larger stones or after failed shock wave lithotripsy. However, anatomical challenges are considered in decision-making[9, 11]. Accordingly, relatively hard stones with multiple rare anatomical anomalies may indicate the non-invasive lines of treatment. So, in the current case, shock wave lithotripsy was tried firstly, although it failed, mostly, due to stone impaction or localization issues. Then, shift to percutaneous lithotripsy was the logic following step. However, missing of the patient at the scheduled dates might make the situation incomplete.
To the best of my knowledge, the current case is the first one to be reported with this constellation of congenital anomalies and presented by urological symptoms; situsinversus with levocardia(without congenital heart defects), skeletal deformities and horseshoe kidney complicatedby nephrolithiasis and hydronephrosis.
Conclusion
Association of situsinversus with levocardia(without congenital heart defects) and skeletal anomalies to a bilaterally nephrolithiasis-complicated horseshoe kidney is very rare entity and novel urological situation. Meticulous evaluation is indicated to exclude the high possibilities of congenital heart defects co-existence and choose the best line for treatment of complications.
Acknowledgement
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License