IJCRR - 6(10), May, 2014
Pages: 33-36
Print Article
Download XML Download PDF
EFFECT OF HANDEDNESS AND SAMPLE COLLECTION TYPES ON BLOOD LACTATE MEASUREMENTS
Author: Brinnell Caszo, Vinod George Thykadavil, Justin Gnanou
Category: Healthcare
Abstract:Introduction: Blood (plasma) lactate levels estimated from samples collected from different body sites may vary. Lactic acid is produced by skeletal muscle, and since skeletal muscle mass has been shown to be higher on the dominant upper limb, we hypothesized that blood lactate levels from the \"dominant\" upper limb will be higher than that of the \"non-dominant\" side at rest. Hence this study was designed to assess the effect of handedness on blood lactate levels drawn from the right and left upper limb. Material and Method: We compared lactate levels in venous blood samples from the right and left antecubital vein and an arterial sample collected from the right upper limb from 14 men and 6 women. Results and Discussion: We found that blood lactate levels between the right and left upper limb sites were comparable. They were also comparable with the arterial blood lactate levels. These findings were observed in both male and female subjects. Thus we conclude that in our sample of subjects', handedness or site of collection of blood sample had no effect on the lactate levels and handedness was not influenced by the sex of the subjects.
Keywords: blood lactate, handedness, pre-analytical variation, dominant and nondominant hand, arterial and venous lactate
Full Text:
INTRODUCTION
Blood (plasma) lactate levels are used in the sports medicine to assess skeletal muscle function and aerobic capacity. Blood lactate levels are estimated from samples collected from different sites such as toe, ear and fingertip and studies have shown that blood lactate levels vary with different sites of blood collection (1). Variation in blood lactate levels may also be due to difference in activity in particular muscles/ muscle groups, the size of the muscle group, and also whether the blood sample is arterial, venous or mixed capillary blood (2). Literature comparing muscle mass and strength between the upper limbs of right and left handed individuals indicate the dominant hand has 10% greater power than the non dominant hand. Such differences have also been found on the lower limb and trunk of the “dominant side” (3, 4). Similarly arm muscle area was found higher in the dominant limb and this increase in muscle area contributed to increase in muscle strength and power. Thus muscle strength and area could contribute to differences in blood lactate level between dominant and non-dominant limbs. Total skeletal muscle mass is also increased in males compared to females and this can be one of the factors for the difference observed in blood lactate levels between male and female subjects under similar physiological conditions. We hypothesize that blood lactate levels from the “dominant” upper limb will be higher than that of the “non-dominant” side at rest. Also in an ideal
clinical set up, arterial blood samples are preferred, however, while collecting samples in the field, venous blood is often preferred for logistic reasons. Hence our secondary aim is to show that the difference between arterial and venous sampling would not be significant.
MATERIALS AND METHODS Subjects
Twenty healthy right-handed subjects (14 men and 6 women) consented to participate in this experiment. The subjects were between the age groups of 20-35 years. Informed consent was obtained from each subject after explaining the objective and protocol of the study and the potential risks involved. Approval for the study was obtained from the Institutional Ethical Review Board of St. John’s Medical College.
Experimental Design
The subjects were explained about the study and the procedures to be carried out prior to the collection. After a mandatory 30-minute rest period, three samples were collected from each subject, one arterial blood sample from the left radial artery at the wrist and two venous samples from the right and left antecubital vein as per the NCCLS (National Committee for Clinical Laboratory Standards) standard guidelines (5). All collections were made between 7.00am to 10 am. Samples were collected without the application of tourniquet and were kept on ice at 4°C. Both the arterial and venous blood was mixed with fluoride/EDTA (Ethylene Diamine Tetra Acetic acid) reagent in the ratio of 2 ml of blood with 0.08ml of the reagent. Samples were then immediately centrifuged at 4°C in a refrigerated centrifuge at 4000 rpm for 5 minutes. The plasma was separated and stored in duplicate aliquots and lactate was analysed immediately using a spectrophotometric method which uses the rabbit muscle lactate dehydrogenase to catalyze the oxidation of lactate to pyruvate with simultaneous production of NAD+ (Nicotinamide Adenine
Dinucleotide). The formation of NADH, which is proportional to lactate concentration, was monitored as the difference in absorbance at 340 nm (6). The results are presented as mean ? standard deviation. Student’s t test and Pearson’s regression analysis was performed to compare arterial lactate concentration and right and left arm venous lactate concentrations using software package SPSS 16.1.
RESULTS
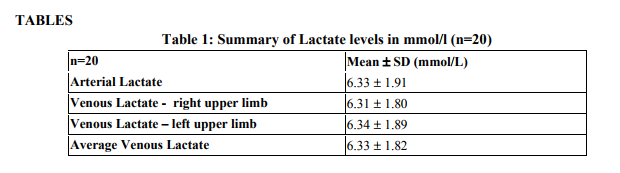
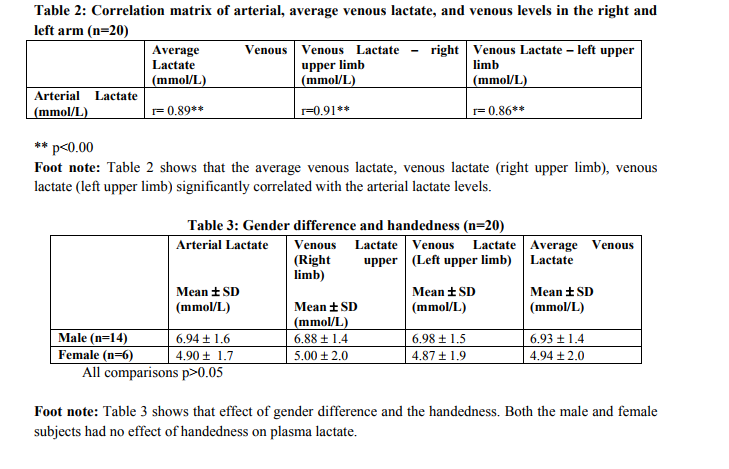
The mean arterial lactate level was 6.33 ± 1.91 mmol/l, while the average venous levels were 6.33 ± 1.82 mmol/l (Table 1). Lactate from blood sampled from the left arm was 6.35 ±1.89 mmol/l while from the right arm it was 6.31± 1.80 mmol/l. The values correlated very well with each other (Table 2) and when compared with a paired student’s t test showed no significant difference between the lactate levels from the 3 collection points. We also observed that though all our subjects were right-handed, venous lactate levels were on average greater on the left arm, when compared with both arterial and venous lactate levels from the right arm. We looked at the effect of gender, and found that though males had higher levels of lactate, they were comparable with the values obtained from the female subjects.
DISCUSSION
Lactate in the body is produced as an intermediary metabolite of carbohydrate metabolism, especially during anaerobic break down glucose. The brain, skin, renal medulla, red blood cells, skeletal muscles and liver all produce lactate; however the liver produces most it. It is metabolized by the liver and kidneys and its blood levels reflect a balance between these processes. Lactate measurements in blood require special blood collection precautions such as a 30 minute rest period for the subject prior to collection, avoiding the usage of tourniquet, and minimal manipulation while collection (5). Though these precautions can be standardized and followed to reduce the pre-
analytical variability, there are two other preanalytical variations to consider. The first factor is the type of blood sample (arterial or venous). In our study we found that lactate levels between arterial and venous collection showed a good positive correlation and were comparable. The data from our study shows that lactate levels from venous samples collected with proper precautions are comparable to the gold standard arterial blood lactate level. The second factor we investigated was handedness of the subjects. Lactate levels correlate with increasing muscle activity and muscle mass. Since muscle mass is increased on the “dominant” side (7), we felt that is may contribute to an increased lactate level on blood sampled from that side. However, data from our study showed no differences between right and left hand and both the value were comparable with the arterial measurements. Gender too appeared to have no effect on the lactate levels of the subjects. As we expected, males subjects tended to have a higher lactate level. This may correlate with the differences in body composition between males and females; since males tend to have higher percentage of body muscle mass compared to females. However, we acknowledge that the number of female participants in this study were fewer when compared to the males and may have influenced our results.
CONCLUSION
Thus muscle mass, strength or power does cause lactate measurement differences and this finding was consistent in both genders. Thus we conclude that lactate measurements are not influenced by type of collection (arterial or venous) as well as by the handedness.
ACKNOWLEDGMENTS
The authors acknowledge the immense help received from the scholars whose articles are citedand included in references of this manuscript. The authors are also grateful to authors / editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. The authors wish to acknowledge the staff of Special Diagnostic Laboratory at Department of Biochemistry, St.John’s Medical College, Bangalore, India for their efforts in performing the laboratory analysis.
References:
REFERENCES
1. Forsyth JJ, Farrally MR. A comparison of lactate concentration in plasma collected from the toe, ear, and fingertip after a simulated rowing exercise. Br J Sports Med 2000;34:35- 8.
2. Yoshida T. Effect of exercise duration during incremental exercise on the determination of anaerobic threshold and the onset of blood lactate accumulation. Eur J Appl Physiol 1984;53;196–9.
3. Ho RW, Chang SY, Wang CW, Hwang MH Grip and key pinch strength: norms for 15- to 22-year-old Chinese students. Zhonghua Yi Xue Za Zhi 2000;63:21-7.
4. Ayse Ozcan, Zeliha Tulum, Lamia PInar, Ferdi Baskurt. Comparison of Pressure Pain Threshold, Grip Strength, Dexterity and Touch Pressure of Dominant and Non-Dominant Hands within and between Right- and LeftHanded Subjects. J Korean Med Sci 2004;19: 874-8.
5. CLSI/NCCLS. Evaluation of precision performance of clinical chemistry devices; approved guideline. CLSI/NCCLS document EP5-A; 1999.
6. Toffaletti JG. Blood lactate: biochemistry, laboratory methods, and clinical interpretation. Crit Rev Clin Lab Sci 1991;28:253-68.
7. Petersen P, Petrick M, Connor H, Conklin D. Grip strength and hand dominance: challenging the 10% rule. Am J Occup Ther 1989;43:444-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





