IJCRR - 6(10), May, 2014
Pages: 28-32
Print Article
Download XML Download PDF
BENIGN FIBROUS HISTIOCYTOMA OF CALCANEUM - A RARE CASE REPORT
Author: Jaya Ganesh P., Suresh Gandhi B., Vimal Chander R., Ganthimathy Sekhar
Category: Healthcare
Abstract:Introduction: Benign fibrous histiocytoma of the calcaneum is an extremely rare neoplasm and it is essential to differentiate it from other common giant cell lesions of bone particularly giant cell tumour of bone. Case Presentation: We present a case of a 38 year old female with an osteolytic lesion in the left calcaneum with a clinical and radiological diagnosis of giant cell tumour of the bone. The definitive diagnosis of benign fibrous histiocytoma was confirmed by histopathological examination and P63 immunomarker negativity. Conclusion: This case is presented due to the rarity of its occurrence in the calcaneum and to stress the significance of using p63 as an immunomarker in differentiating from giant cell tumour.
Keywords: Benign fibrous histiocytoma, Giant cell tumour, P63.
Full Text:
INTRODUCTION
Benign fibrous histiocytoma (BFH) is a soft tissue tumour of fibrous histiocytic type rarely occurring in the bones, especially the calcaneum. It is a spindle cell neoplasm of the bone and needs to be differentiated from non-ossifying fibroma and giant cell tumour of bone. [1] Very few cases of benign fibrous histiocytoma arising in the calcaneum have been reported in the literature. We report a case of benign fibrous histiocytoma in the calcaneum occurring in a middle aged female and the role of P63 in differentiating it from the giant cell tumour. [2]
CASE REPORT
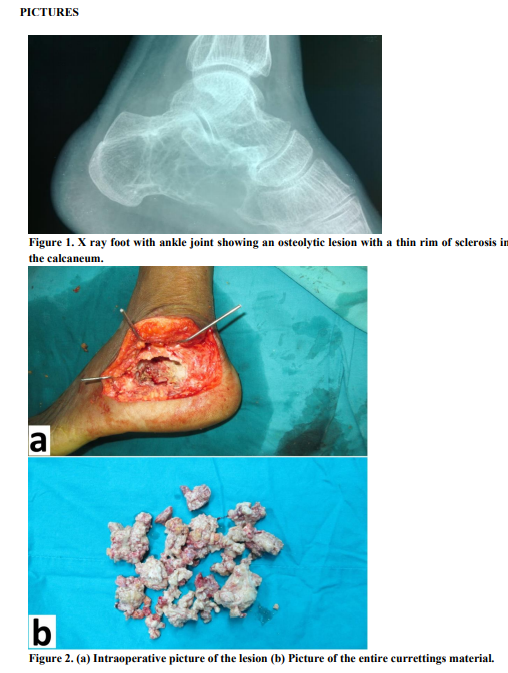
A 38 year old female presented with pain in the left foot mainly on weight bearing which gradually increased in intensity for the past six months. There was no significant swelling or other relevant history of injury noted. Clinical examination of the foot revealed bony tenderness with the X-rayshowing an osteolytic lesion in the left calcaneum. Haematological and biochemical parameters were within normal limits. In view of the radiological appearance, a diagnosis of giant cell tumour of bone / chondromyxoid fibroma was considered.
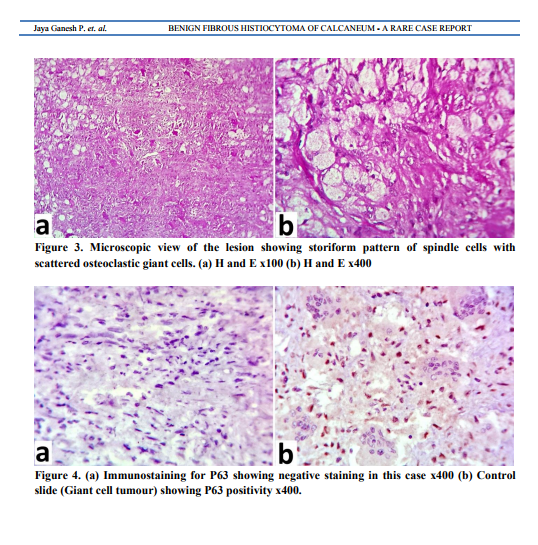
[Figure 1] Under spinal anaesthesia, curettage of the osteolytic lesion was done and sent for histopathological examination. Histopathology revealed only tiny fragments of bony tissue with sheets of foamy histiocytes. There were no osteoclastic giant cells to suggest giant cell tumour or chondromyxoid fibroma. Since the material was very minimal, a repeat curettage was advised and planned for a confirmatory diagnosis. Under spinal anaesthesia, repeat curettings of the entire lesion was done and sent for histopathological examination. The intraoperative and postoperative period was uneventful. Macroscopically, multiple yellowish and grey white bony and soft tissue fragments measuring 3x2x1.5 cm in aggregate were seen. [Figure 2] Microscopic examination revealed a lesion composed predominantly of foamy histiocytes and scattered spindle cells arranged in a storiform pattern. [Figure 3] There were osteoclastic giant cells scattered throughout but not seen uniformly in a spatial relationship as in a giant cell tumour of bone. A diagnosis of benign fibrous histiocytoma was made and confirmed by negative immunostaining for p63. [Figure 4] Patient came for follow up and is doing well.
DISCUSSION
Benign fibrous histiocytoma is a spindle cell neoplasm with varying degrees of spindle cells, foam cells and multinucleated giant cells. They occur very rarely within bones and approximately 86 cases have been reported in literature with this case being only the second case to be reported in the calcaneum, a very unusual site. [1] Benign fibrous histiocytoma, a tumour known to occur in the dermis and soft tissues, comprised about ten cases out of 11087 skeletal tumors studied by Dahlin and Unni. [3] The cases were adults between the ages of 23 to 60 years and the male: female ratio was 4:3. In a series reported by Grohs et al, a median age of 28 years and male: female ratio of 4:6 was noted.[4] Many authors actually suggest that it is a non ossifying fibroma, and the location of the lesion with clinical history of pain and the age group is essential in making a diagnosis of BFH. [2] Local pain is the main symptom in benign fibrous histiocytoma in contrast to nonossifying fibroma and the X-ray shows an osteolytic lesion with sharply defined sclerotic borders in a typical case of benign fibrous histiocytoma. In the present case reported there was no thick sclerotic rim. [5] Nonossifying fibroma is usually an incidental radiological finding and is seen in patients younger than 20 years. It is unusual after skeletal maturation. The most common site is the distal femur and proximal tibia. Benign fibrous
histiocytoma occurs in adults and usually in the long bones and pelvis. In a case series comprising ten benign fibrous histiocytomas of bone, the common sites were femur, pelvis, humerus, tibia, fibula, ribs and spine. [3] Benign fibrous histiocytoma also needs to be differentiated from the common clinical and radiological diagnosis of giant cell tumour of bone as in our case. Most neoplasms of the bone may contain giant cells but uniform spatial arrangement of osteoclastic giant cells with mononuclear stromal cells is critical in making a diagnosis of giant cell tumour. Lesions with osteoclastic giant cells and spindle cells if present in flat bones also need to be differentiated from hyperparathyroidism and aneurysmal bone cyst which have other distinctive histological features. [5] The diagnosis of giant cell tumour needs to be consisdered strongly as collections of foam cells dominate the picture and mononuclear cells may become spindled and have even a storiform pattern, in which case a mistaken diagnosis of benign fibrous histiocytoma can be made.[2] A lesion with all the clinical and radiological features of giant cell tumor has to be diagnosed as giant cell tumour even if the predominant pattern is of benign fibrous histiocytoma and only minor foci shows osteoclastic giant cells. [2] In such cases p63 immunostaining can be of immense help in differentiating benign fibrous histiocytoma (p63 negative) from giant cell tumour (p63 positive).[6] p63 is a p53 homolog expressed in normal epithelial tissues and in epithelial malignancies. It is mainly used as a marker for mammary myoepithelial cells and prostatic basal cells and recent studies have indicated moderate nuclear staining in the stromal cells of giant cell tumor of bone. Non ossifying fibroma shows less than 10% staining for p63 and generally most of the soft tissue tumors do not express p63.[7] The behaviour of benign fibrous histiocytoma is benign in contrast to the locally aggressive behaviour of giant cell tumor of the bone. [8]
CONCLUSION
Benign fibrous histiocytoma can occur in the calcaneum and the X-ray picture may be atypical as in our case and the significance of using p63 as an immunomarker in differentiating from the clinical and radiological diagnosis of giant cell tumour is stressed in doubtful cases where microscopic features are equivocal. This case is presented due to the rarity of its occurrence in the calcaneum, as to the best of our knowledge, this is the second case to be reported in the calcaneum in literature.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
REFERENCES
1. Keskinbora M, Kose O, Karsliogluy, Demiralp B, Basbozkurt M. Another cystic lesion in the calcaneus: Benign Fibrous Histiocytoma of bone. J Am Podiatr Med Assoc. 2013;103(2):141-4.
2. Inwards CY, Oliveira AM. Tumors of the Osteoarticular System. In: Fletcher DM, Diagnostic histopathology of tumors. 4th ed. Elsevier, Saunders. 2013. pp 1907-8.
3. Unni KK, Dahlin DC, Dahlins. Bone tumours, general aspects and data on 11087 cases. Fifth edition. Philadelphia, PA: Lippincott williams and wilkins: 1996: 211-216
4. Grohs JG, Nicolakis M, Kainberger F, Lang S, Kotz R. Benign fibrous histiocytoma of bone: a report of ten cases and review of literature. Wien Klin Wochenschr. 2002 Jan 15;114(1- 2):56-63.
5. Forrest M, Tomeno A, Vanel D. Orthopaedic surgical pathology. Diagnosis of tumours and pseudotumoral lesions of bone and joint. Edinburg churchill livingstone: 1997:317-21.
6. Gustavo de la Roza G. P 63 expression in giant cell containing lesions of bone and soft tissue. Arch Pathol Lab Med 2011;135(6):776- 9.
7. Wu CS, Pollack A, Czerniak B, Chyle V, Zagars GK, Dinney CP, Hu SX, Benedict WF. Prognostic value of p53 in muscle-invasive bladder cancer treated with preoperative radiotherapy. Urology. 1996 Mar;47(3):305- 10.
8. Clark BE, Xipell JM, Thomas DP 1985 Benign fibrous histiocytoma of bone. Am J Surg Pathol 1985;9:806-15.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





