IJCRR - 6(11), June, 2014
Pages: 87-90
Print Article
Download XML Download PDF
COMPARATIVE CLINICAL EVALUATION OF REDUCTION IN TOOTH MOBILITY USING PERIOTEST\? IN LOWER ANTERIOR TEETH POST PHAS - I THERAPY IN PATIENTS WITH MILD TO MODERATE GINGIVITIS: A RANDOMIZED CONTROLLED TRIAL
Author: Kunal A. Banavali, Pradeep Chitnis, Ketaki Upadhye, Bhoomi Kotak
Category: Healthcare
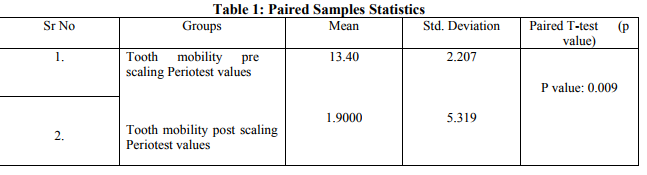
Abstract:Background: The Periotest\? method is a technique for the objective assessment of tooth mobility. The aim of this study was to determine the reduction in tooth mobility following phase I therapy (scaling and root planning) in individuals aged 18-30 years using Periotest\?. Materials and Methods: Initial scoring of tooth mobility was done using Periotest\? followed by phase-I therapy which included scaling and root planning using ultrasonic scalers and hand instruments. The second scoring was done 14 days following phase-I therapy and instructions in oral hygiene. Patients with presence of grade I mobility with lower anterior teeth, no bone loss radiographically, no periodontal pocket and absence of pulpal pathology and severe occlusal interferences in the teeth to be treated were included in the study. Result: A significant increase in the proportion of teeth with zero mobility was observed 14 days following completion of the nonsurgical phase-I therapy. The tooth mobility pre scaling and root planning was 10-18 Periotest value (13.40\?2.207) and tooth mobility post scaling and root planning after 14 days was -8-7 Periotest value (1.9000\?5.319). Statistical analysis was carried out using paired T-test; the p value was statistically significant (p?0.005). Conclusion: From the above study we can conclude that abnormal tooth mobility decreased following the hygienic phase of periodontal treatment (scaling, root planing, polishing and oral hygiene instruction) using Periotest\? method as objective method for measurement of tooth mobility.
Keywords: Periotest, gingivitis, oral hygiene
Full Text:
INTRODUCTION
The significance of presence tooth mobility as a manifestation of periodontal disease is controversial.1 However, decrease in mobility is generally considered to be a desirable outcome of periodontal therapy, while increasing mobility a year or more after the treatment has been suggested to indicate a need for further dental therapy.2 Thus in selection of a modality for periodontal treatment, a favorable mobility response is one of several considerations. Furthermore, mastication on firm teeth is more comfortable than biting on mobile teeth. A reduction in hypermobility after scaling and establishing good oral hygiene has been reported in several studies,3,4 while occlusal adjustment may further decrease the mobility.4 5 Studies have included patients with or without occlusal adjustment in addition to the scaling and hygienic therapy. Considerable reductions in mobility along with good results of the periodontal therapy have been seen with or without occlusal adjustment. 2, 6,7 Furthermore, presence of tooth mobility after treatment does not seem to influence the treatment outcome, as long as the oral hygiene is good and the mobility is not increasing.2 The aim of the following study was to clinically compare the reduction in tooth mobility after phase-I therapy using Periotest® as objective method for measurement of mobility.
MATERIALS AND METHODS
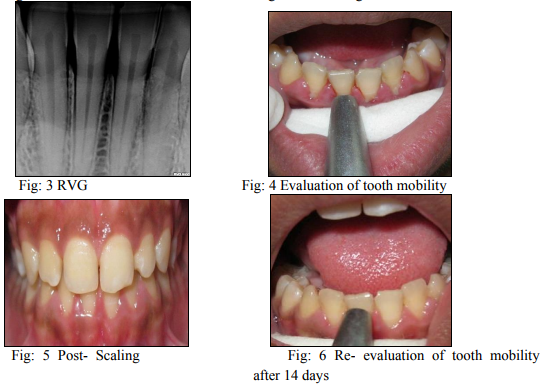
Thirty patients aged 18-30 years were selected from the OPD of department periodontics of Y.M.T. Dental College and Hospital for the randomized, controlled clinical trial. Informed consent was taken from all the patients who participated in the study. Initial scoring of tooth mobility was done using Periotest® (Fig.4) followed by phase-I therapy which included scaling and root planning using ultrasonic scalers and hand instruments. The second scoring was done 14 days following phase-I therapy and instructions in oral hygiene (Fig.6). Tooth mobility was scored on basis of following Periotest® values; -8 to +9: clinically firm teeth, 10-19: first distinguishable sign of movement, 20-29: crown deviates within 1 mm of its normal position, 30- 50: mobility is readily observed. Inclusion criteria included age group from 18 to 40 years, presence of grade I mobility with lower anteriors, no bone loss radiographically, no periodontal pocket and absence of pulpal pathology and severe occlusal interferences in the teeth to be treated (Fig.3) Exclusion criteria included trauma from occlusion with lower anteriors, localized periodontitis with lower anteriors, patient undergoing orthodontic treatment, pregnancy or lactating mothers, participants should not have systemic disease that could modify the periodontal disease. Results obtained were statistically analyzed using paired T-test.
RESULTS
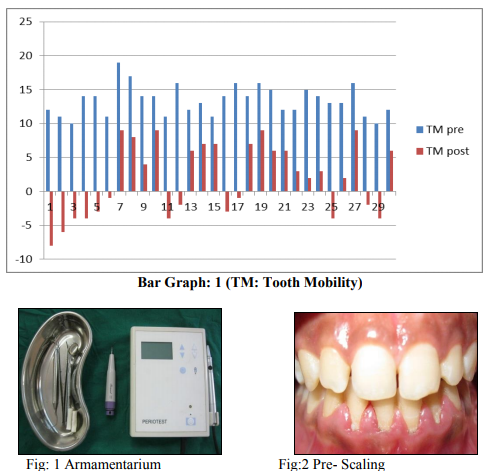
A significant increase in the proportion of teeth with zero mobility were observed 14 days following completion of the nonsurgical phase-I therapy (Bar graph: 1).This table illustrates an increase in the proportion of firm teeth after the phase-I therapy (initial scaling and root planning). The tooth mobility pre scaling and root planning was 10-18 Periotest value (13.40±2.207) and tooth mobility post scaling and root planning after 14 days was -8-7 Periotest value (1.9000±5.319). Statistical analysis was carried out using paired Ttest; the p value was statistically significant (p?0.005) (Statistics table: 1). Thus all patients recruited in the study showed reduction in tooth mobility.
DISCUSSION
The slight but gradual decrease in mobility after the initial treatment may be a manifestation of a slow reorganization of the periodontal supporting structures under good maintenance care. The specific structural and biological phenomena responsible for these changes are not known. It was also interesting to note that, as reported by Rateitschak in 1963, teeth with higher initial mobility values had a greater tendency to improve (get lower mobility) than teeth with initially low mobility values. He also found a gradual, slight decrease in mobility over 2 to 3 years using a mechanical measuring device.8 Wust indicated a 25.3% reduction in tooth mobility 559 days after local periodontal treatment. His subjects had generalized marginal periodontitis, and required soft tissue curettage, selective occlusal grinding, and surgical treatment.9 Persson demonstrated diminishing mobility following oral hygiene instruction and supra- and subgingival scaling in patients with moderate periodontal disease from a period of 3 months to 1 year.10
CONCLUSION
The most fundamental and widely used method of periodontal treatment is the removal of deposits from teeth. Although it has never been conclusively proven that dental accretions are a direct cause of periodontal disease, it has long been recognized that removal of these deposits initiates a return to health. From the above study we can conclude that abnormal tooth mobility decreased following the hygienic phase of periodontal treatment (scaling, root planing, polishing and oral hygiene instruction). Hence decrease in tooth mobility can be a method of assessment of the outcome of periodontal treatment procedures.
References:
1. Ramfjord, S. P., and Ash, M. M., Jr.: Significance of occlusion in the etiology and treatment of early, moderate and advanced Periodontitis. J Periodontol 52: 511, 1981.
2. Lindhe, J., and Nyman, S.: The role of occlusion in periodontal disease and the biological rationale for splinting in treatment of Periodontitis. Oral Sci Rev 10: 11, 1977.
3. Fehr, C, and Mühlemann, H. R.: Objective Erfassung der Wirkungeiner internen Parodontal Therapie ("Biostimulin"). Parodontologie 4: 152, 1956.
4. Wüst, B. P., Rateitschak, K. H., and Mühlemann, H. R.: Der Einfluss der lokalen parodontal Behandlung auf die Zahnlocherung und der Entzündungsgrad des Zahnfleisches. Helv Odontol Acta 4: 58, 1960.
5. Kegel, W., Selipsky, H., and Phillips, C: The effect of splinting on tooth mobility. I. During initial therapy. J Clin Periodontol. 6: 45, 1979.
6. Lindhe, J., and Nyman, S.: The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health. A longitudinal study of periodontal therapy in cases of advanced disease. J Clin Periodontol 2: 67, 1975.
7. Rosling, B., Nyman, S., and Lindhe, J.: The effect of systematic plaque control on bone regeneration in infrabony pockets. J Clin Periodontol 3: 38, 1976.
8. Rateitschak, K. H.: The therapeutic effect of local treatment on periodontal disease assessed upon evaluation of different diagnostic criteria. I. Changes in tooth mobility. J Periodontol 34: 540, 1963
9. Wust, B. P., Rateitschak, K. and Muhlemann, H. R.: Influence of local periodontal treatment on tooth mobility and gingival inflammation. D. Abs., 6:270, 1961.
10. Persson, R.: Assessment of tooth mobility using small loads. II. Effect of oral hygiene procedures. J Clin Periodontol 7: 506, 1980.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





