IJCRR - 6(11), June, 2014
Pages: 36-42
Date of Publication: 13-Jun-2014
Print Article
Download XML Download PDF
RESULTS OF EARLY EXCISION OF POST TRAUMATIC HETEROTROPHIC OSSIFICATION OF ELBOW -FOLLOW UP REPORTS ON 17 PATIENTS
Author: Ravichandran S., Surendher Kumar R., Ramesh Periyasamy, Krishnagopal R.
Category: Healthcare
Abstract:We review our results of 17 patients, who had early excision 5 months (3-8 months) of post traumaticHeterotrophic ossification (HO) of elbow,followed by medical treatment with indomethacin to prevent recurrence, in our study. The average age group of our patients is 24 years (15-38). There were 12 males and 5 females. The patients were followed up for average of 58 months (38-90 months). The mean preoperative Mayo Elbow Performance Score (MEPS) was 63(40-80), and the mean MEPS core at final follow up is 90(75-100). According to MEPS, 13 patients had excellent result and 4 patients had good result. All the patients were asymptomatic at the time of final follow up. One patient with intra operative ulnar nerve injury recovered partially, and remained with some disability at final follow up. Patient with pre operative median nerve palsy recovered completely at 3 months post operatively.
Keywords: Heterotrophic Ossification, MEPS, Early Excision
Full Text:
INTRODUCTION
Heterotrophic ossification of elbow occurs in approximately two to three percent of patients with the local trauma1 .The severity of the trauma can vary from soft tissue injury to fracture, and fracture dislocation of the elbow. The factor that increases soft tissue injury such as passive stretching2 is believed to predispose to the formation of heterotrophic ossification of elbow. The choice of treatment ofpre existingHO of elbow associated with functional disability is surgical excision3,4,5,6,7. The timing of surgical excision4,5,6,7,8,9,10,11 , the method of prevention of recurrence9,11, and the actual risk of recurrence9,11,12,however, remains a controversial subject of debate mainly due to unpredictable outcome reported in the literature. In our study, we retrospectively reviewed our results of early excision of heterotrophic ossification of elbow in patients with trauma in young age.
PATIENTS AND METHODS
From 2006 to 2012, we encountered 47 patients with ankylosis of elbow in our hospital. Nine patients had complete osseous ankylosis of elbow.Fifteen patients had fibrous ankylosis of elbow without HO. Twenty three patients had ankylosis with HO. All the patients were less than 40 years of age, with history of local trauma, either soft tissue or bony injury, who presented to us early, (arbitrarily within 8 months)were included in our study. Patients with associated head injury, more than 40 years of age and with duration more than eight months were excluded from our study. Eighteen patients met our selection criteria. Adequate clinical data and radiographs were collected from the medical records. One patient lost to follow up. Thus, we report our results of 17 patients in our study. The average age of the patients was 24 years (15-38).
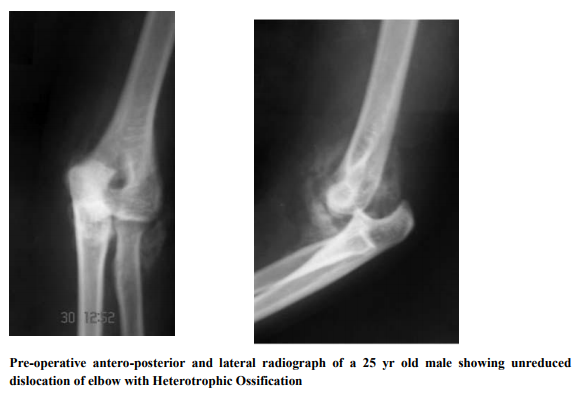
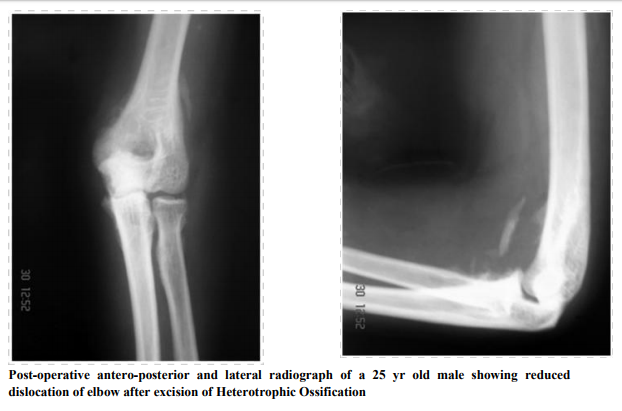
Twelvepatients were male and five females. The right hand was involved in ten patients and all were dominant on the same side, left hand was involved in seven patients, with one patient dominant on the injured side.Fifteen patients had native treatment, which includes massage of affected area using oil, eggs and bandage, which are commonly practiced in developing countries. Three patients had untreated posterior dislocation of elbow. One patient underwent open reduction and internal fixation for intercondylar fracture of humerus, and another patient had conservative treatment in the form of above elbow slab application for three weeks.The patients had functional disability as the main complaint, and showed no improvement in arc of motion after 4 weeks of supervised physiotherapy.Pre operativeanteroposterior and lateral radiograph of the affected elbow were taken.The heterotrophic ossification was predominantly postero medial in five patients, posteromedial and lateral in ninepatients,and anterolateral in three patients. All patients were treated with excision of heterotrophic ossificationand soft tissue contracture release. One patient had displaced fracture distal shaft of humerus, and underwent simultaneous internal fixation with DCP and autogenous bone grafting. Three patients had unreduced posterior dislocation. All of them were reduced after adequate soft tissue release by both medial and lateral approach. No patient required triceps lengthening. The approach was selected appropriate to the site of heterotrophic ossification. Thus onepatient had medial approach, ten patients required bothmedial and lateral, five patients lateral, and one patient posterior approach. Post operatively patients were treated with oral Indomethacin 25 mg three times a day for 6 weeks,along with Pantoprazole 40 mg once a day in empty stomach.Three doses of first generation of cephalosporin, preoperatively one dose and two doses postoperatively at 8 hours interval, was given prophylactically for all the patients. The active and active assisted motion was started from the nextday of surgery and continued approximately for 12-18 months to consolidate the gain in arc of motion.The patients with untreated posterior dislocation were immobilized for two weeks in cast and mobilization started thereafter. The clinical evaluation was done with MEPS pre operatively, and at final follow up. Radiographs in antero posterior and lateral views taken pre operatively, post operatively, and at final follow up, for the assessment.
RESULTS
The mean duration from the time of injury and time of surgical excision is 5 months (3-8 months). The mean duration of follow up was 58 months (38-90 months).The average mean preoperative arc of motion is 41deg(0-110deg). The mean post operative value of extensionis 17 deg (0-40 deg),flexion of 124deg(100-140),and the arc of motion is 104deg(60-140). The mean pre operative rotation is 91deg (40-140)and the mean post operative arc of rotation is 132deg(100-160). The mean post operative MEPS increased to 90(75-100) at final follow up, from the pre operative value of 63(40-80). Three patients developed grade 1 mild laxity on the medial side, but remained unaffected on their routine activities at final follow up.According to MEPS, 13 patients had excellent result and 4 patients had good result. The three patients who underwent bony procedure had complete union.
There was no evidence of recurrence of heterotrophic ossification. One patient with intra operative ulnar nerve injury recovered partially, and remained with some disability at final follow up. Patient with pre operative median nerve palsy recovered completely at 3 months post operatively. Seven patients had mild abdominal discomfort initially at one week of Indomethacin treatment, but were able to complete the course without any further complaints. All the patients remained satisfied with the procedure at final follow up.
DISCUSSION
The causes for heterotrophic ossification are varied13,14,15. They include local injury, head injury, spinal cord injury, surgery to the elbow,neurological conditions such as stroke, poliomyelitis, thermal and electrical burns. The hip, elbow, knee, and shoulder are commonly involved in heterotrophic ossification3 . The clinical course is usually progressive initially, and then remains static17, and may spontaneously resolve in some case 16. The choice of treatment in patient withpre existing HOwith functional disability is surgical excision. The timing of surgical treatment is still a matter of debate. The earlier studies have largely reported delayed surgical exciosion of HO, approximately 18-20 months, after maturation of HO3,4,5,6. The maturation of the bone was decided based on serum alkaline phosphatase, radiographs, bone scans, which were subsequently found to be unreliable indicators. Moreover, the status of maturity of bone, levels of alkaline phosphatase, and positive bone scans were not predictive of recurrence risk of HO after surgical excision3,9 . Several authors have favored early excision as it makes the procedure easier, less traumatic and decrease the period of functional disability and provides equally good functional results with low rate of recurrence 8,9,12,18,19,20.The reported number of patients in the literature treated with early excision is less, and the etiologies are varied in those papers. Our series had young patients with only trauma as single etiology. The early surgical intervention in our series also helped us to reconstruct the fracture in one patient, and relocate the elbow in three cases with unreduced dislocation of elbow.The functional outcome is significantly improved as assessed by MEPS score.The complication was also comparable with other series, with one patient developing ulnar nerve palsy,which recovered partially.Thus the early excision, apart from making surgery easier and limiting soft tissue contracture8,9,10, provides good functional results compared to delayed excision of HO3,12 . Regarding the method of prophylaxis, despite the proven success of radiotherapy, or indomethacin, or combination of both in the hip following primary arthroplasty, acetabular fracture reconstruction, and post surgical excision of HO21,22,23,24,25, the evidence in case of elbow is inadequate. The risk of recurrence of HO of elbow in patients with head injury is postulated to be substantial than due to trauma3 . Though theoretically the risk of recurrence is high, except for one series in which patients with head injuries were included3 , the other series have reported low recurrence rate without prophylaxis7, 12, or with radiotherapy9,11. The high recurrence rate in DE Garland series 3 have been attributed to the severity of the neurological status of the patient. Also, the risk of wound complications, and the theoretical risks of sarcoma due to radiation in young patients with longevity of life have been also debated in the literature 9,12. Since the risk of recurrence contemplated to be low for the patients with trauma18,19,20, ease and low cost of administration of Indomethacin despite its gastrointestinal side effects, and cost of radiotherapy, we treated our patients with early excision, and prophylaxis with Indomethacin.There was no case of recurrence of HO in our patients at final follow up. The major problem associated with Indomethacin is its gastrointestinal side effects.
CONCLUSION
Our series is unique in the way that it consist 17 patients, one of the large series to have undergone early excisionin a single etiology group. The drawback in our study is nature of the study, retrospective, and the limited number of cohorts to provide a statistical significance. Despite these limitations, we favor early excision of Heterotrophic Ossificationof elbow in post traumatic patients, along with prophylactic oral Indomethacin and early ROM exercise, which is evident with our encouraging results.
References:
1. Thompson, H. C., III; and Garcia, A.: Myositis ossificans: aftermath of elbow injuries. Clin.Orthop. 1967; 50: 129-134.
2. Evans EB. Orthopedic measures in the treatment of severe burns. J Bone Joint Surg Am. 1966;48:643-69.
3. Garland, D. E.; Hanscom, D. A.; Keenan, M.A.; Smith, C.; and Moore, T.: Resection of heterotopic ossification in the adult with head trauma. J. Bone and Joint Surg. Oct. 1985; 67- A:1261-1269.
4. Hoffer, M. M.; Brody, G.; and Ferlic, F.:Excision of heterotopic ossification aboutelbows in patients with thermal injury. J.Trauma1978; 18:667-670.
5. Peterson, S. L.; Mani, M. M.; Crawford, C.M.; Neff, J. R.; and Hiebert, J. M.:Postburn heterotopic ossification: insights for management decision making. J. Trauma 1989; 29:365-369.
6. Roberts, J. B.; and Pankratz, D. G.: The surgical treatment of heterotopic ossification at the elbow following long-term coma. J.Bone and Joint Surg. July 1979; 61-A:760- 763.
7. David Ring, Jesse B. Jupiter. Operative Release of Complete Ankylosis of the Elbow Due to Heterotopic Bone in Patients without Severe Injury of the Central Nervous System.J Bone Joint Surg Am. 2003;85:849-857
8. Beingessner DM, Patterson SD, King GJ.Early excision of Heterotopic bone in the forearm. J Hand Surg [Am]. 2000;25:483-8.
9. McAuliffe JA, WolfsonAH.Early excision of heterotopic ossification about the elbow followed by radiation therapy. J Bone Joint Surg Am. 1997;79:749-55.
10. Viola RW, HanelDP.Early “simple” release of posttraumatic elbow contracture associatd with heterotopic ossification. J Hand Surg [Am]. 1999;24:370-80.
11. GARLAND. D. E., and RHOADES, M. E.: Orthopaedic Management of Brain-Injured Adults. Part II. Clin.Orthop., 131: 111-122, 1982.
12. Alok Gaur, Marc Sinclair, Enzo Caruso, Giuseppe Peretti and David Zaleske. Heterotopic Ossification Around the Elbow Following Burns in Children: Results After Excision .J Bone Joint Surg Am. 2003;85:1538-1543.
13. DE Garland, CE Blum and RL Waters.Periarticular heterotopic ossification in head-injured adults.Incidence and location.J Bone Joint Surg Am. 1980;62:1143-1146
14. R. H. Wittenberg, U. Peschke, U. B?tel;Heterotopic Ossification After Spinal Cord Injury Epidemiology And Risk Factors,Bone Joint Surg [Br] 1992; 74-B :215- 8.
15. T. W. Axelrad,B. Steen,D. W. Lowenberg,W. R. Creevy;T. A. Einhorn. Heterotopic ossification after the use ofcommercially available recombinant human bone morphogenetic proteins in four patients,J Bone Joint Surg [Br] 2008;90-B:1617-22
16. Munster AM, Bruck HM, Johns LA, Von Prince K, Kirkman EM, RemigRL.Heterotopic calcification following burns: a prospective study. J Trauma.1972;12:1071-4.
17. L. Sazbon, T. Najenson, M. Tartakovsky, E. Becker, Z. Grosswasser. Widespread Periarticular New-Bone Formation In LongTerm Comatose Patients. British Editorial Society Of Bone And Joint Surgery 1981; Vol. 63-B, No. 1, 1981, 120-125
18. Garland, D. E.: A clinical perspective on common forms of acquired heterotopic ossification. Clin.Orthop.1991; 263:13-29.
19. Hastings, H., II; and Graham, T. J.: The classification and treatment of heterotopic ossification about the elbow and forearm.HandClin. 1994; 10:417-437.
20. Jupiter, J. B.: Heterotopic ossification about the elbow. In Instructional Course Lectures,The American Academy of Orthopaedic Surgeons. Vol. 40, pp. 41-44. Park Ridge,Illinois, The American Academy of Orthopaedic surgeons, 1991.
21. T. N. Board,A. Karva,R. E. Board,A. K. Gambhir,M. L. Porter.The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty.J Bone Joint Surg [Br]2007;89-B:434-40.
22. Ahrengart L, Lindgren U, Reinholt FP. Comparative study of the effects of radiation,indomethacin, prednisilone and ethane-1-hydroxy-1, 1-disphonate (EHDP) in the prevention of ectopic bone formation. ClinOrthop 1988;229:265-73.
23. Burd TA, Lowry KJ, Anglen JO. Indomethacin compared with localized irradiation for the prevention of heterotopic ossification following surgical treatment of acetabular fractures. J Bone Joint Surg [Am] 2001;83-:1783-8.
24. Matta JM, Siebenrock KA. Does indomethacin reduce heterotopic bone formation after operations for acetabular fractures?: a prospective randomised study. J Bone Joint Surg [Br] 1997;79-B:959-63.
25. McLaren AC. Prophylaxis with indomethacin for heterotopic bone after open reduction of fractures of the acetabulum. J Bone Joint Surg [Am] 1990;72-A:245-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





