IJCRR - 6(11), June, 2014
Pages: 14-17
Date of Publication: 13-Jun-2014
Print Article
Download XML Download PDF
MATURE CYSTIC TERATOMA HARBOURING SQUAMOUS CELL CARCINOMA - A CASE REPORT
Author: Krishnendu Das, Arindam Karmakar, Debanjan Bhattacharjee
Category: Healthcare
Abstract:Aim: Squamous cell carcinoma arising in a mature cystic teratoma is an extremely rare event. This effort aims at adding authors' experience to the pool of knowledge of this very rare but ominous tumour. Case Report: Herein, we report a case of squamous cell carcinoma in mature cystic teratoma of right ovary in a 45-year-old woman presenting with abdominal mass which was diagnosed after surgery. The tumour was large and cystic. An exhaustive search was made to rule out the possibility of metastasis into the ovary. Discussion: Benign or malignant tumours that arise in a benign cystic teratoma are rare. Malignant transformation occurs in only 1-3% of benign cystic teratomas1, 2, 3. Preoperative diagnosis is difficult because of the lack of specific symptoms and signs to suggest malignancy 4. Factors such as age, tumour size, tumour markers and tumour imaging characteristics help in preoperative risk assessment. Better understanding of the pathology and prognostic factors of this group of tumours is required for early and proper management. Conclusion: This report emphasizes on the sinister nature of malignant transformation of mature teratoma and the importance of comprehensive investigations for early diagnosis and treatment.
Keywords: mature cystic teratoma, squamous cell carcinoma, ovary
Full Text:
INTRODUCTION
Benign cystic teratoma (Dermoid cyst) is the most common ovarian neoplasm, comprising 25% or more of all ovarian tumours. Secondary malignancies, which typically occur in postmenopausal woman, are extremely rate 1, 2, 3 . Presenting complaints are nonspecific and include abdominal or pelvic pain, abdominal distension, or a palpable mass. Secondary neoplasms are usually unilateral, but the contralateral ovary may contain a benign cystic teratoma. Nevi, sebaceous adenomas and other cutaneous adnexal neoplasms, benign salivary gland type tumours, meningioma, glomus tumour, and haemangiomatous vascular proliferations are among the benign neoplasms that arise in benign cystic teratoma5 . In situ malignant tumours that have been reported include squamous cell carcinoma in situ and Paget’s disease. Invasive squamous cell carcinoma comprises about 85% of secondary malignancies arising in benign cystic teratoma6 . The remainders are other types of cutaneous carcinoma, such as basal cell carcinoma or sebaceous carcinoma7 , melanoma, adenocarcinoma, various types of sarcoma, and other rare tumour types. Rare mucinous epithelial tumours that arise in a teratoma give rise to pseudomyxoma peritonei8
CASE REPORT
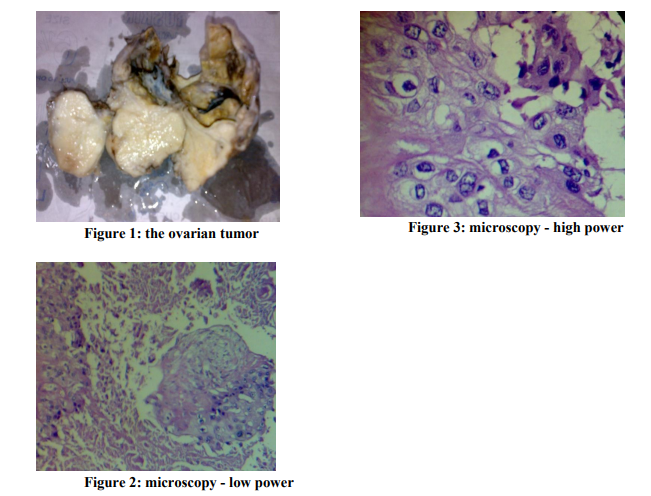
A 45-year-old multigravida presented with history of abdominal pain. She didn’t have any medical co morbidity. There were no complaints of alteredbowel and bladder habits. Per vaginum bimanual examination revealed unilateral adnexal mass. On pelvic ultrasonography, right sided ovarian cystic masses with solid component were demonstrated. Computed tomography scan of abdomen and pelvis showed a 10×7 cm right adnexal mass with ossified elements in ovary. Radiological impression favored a diagnosis of teratoma of right ovary with possible malignant transformation. There was no free fluid in the abdomen. The serum CA-125 level was found to be 885 IU/ml (normal 0-35 IU/ml). A tentative preoperative diagnosis of teratoma with possible malignant transformation was entertained, and the patient was counseled to undergo an exploratory laparotomy with total abdominal hysterectomy, bilateral salpingo-oophorectomy. At laparotomy, the right ovarian mass appeared to be partly cystic partly solid areas. The capsule was intact, and there were no significant pelvic or para-aortic lymph nodes. The omentum was grossly unremarkable. On gross examination, the right ovarian tumour measured 10×7×5 cm which on cut section showed approximately 50% solid area and 50% cystic. Cyst contained hair (Fig. 1). Microscopically, sections from the right ovarian tumour showed a moderately differentiated squamous cell carcinoma in mature cystic teratoma Fig. 2 and Fig. 3). The tumour was confined to right ovary. Uterus showed features of adenomyosis, hyperplastic endometrial polyp and cystic endometrial atrophy while cervix revealed chronic inflammation. Left ovary, both the right and left fallopian tubes and omentum were free of tumour.
DISCUSSION
Mature cystic teratomas make up almost 20% of all ovarian neoplasm and also constitute the most common ovarian tumour in childhood. Malignant transformation of this benign lesion is an extremely rare incidence 1, 2, 3 . Although mature cystic teratomas are frequently bilateral, malignant change has usually been reported on only one side. Squamous cell carcinoma (SCC) arising in mature cystic teratoma most probably develops from epidermal elements (80%), although an origin from bronchial epithelium is a possibility. In favour of former origin is finding of squamous cell carcinoma in situ adjacent to carcinoma. Alternatively, it can arise from endometriosis or Brenner tumour. S quamous cell carcinoma may also be seen as metastatic deposits from squamous cell carcinoma elsewhere especially cervix, even though that tumour may have occurred many years previously. Our patient however did not reveal such source. The carcinoma begin at or near dermoid protuberance, continue to grow without clinical evidence, eventually penetrating full thickness of the wall, developing direct extension and malignant adhesions to the neighbouring organs. In majority of the cases, invasion or metastases have occurred before diagnosis. Spread beyond the capsule can produce peritoneal seeding and symptoms such as pain, ascites and signs of peritoneal irritation, such cases being prognostically poor. Fortunately our case didn’t show any evidence of metastasis. Several authors pointed out the importance of intact capsule regarding good prognosis if confined to the cyst. Preoperative diagnosis of malignant change in benign teratoma is extremely difficult providing a substantial challenge and confusion regarding a need for surgical staging and adjuvant therapy. Risk factors for malignancy in mature teratoma include age of the patient, tumour size, imaging findings and serum tumour markers. It has been observed that in teratoma, malignant transformation occurs in relatively older patient population; the mean age range reported being 45-60 yrs. Frequency of malignant change, rises with increasing age, reaching up to 19% in women after menopause. Hence, the need for the thorough search for such malignant change, in dermoid cyst after the age of 45years.Larger tumours correlate with increased risk of malignant transformation. Kikkawa et al 9 , in their study found that tumour diameter >9.9cm was 86%
sensitive for malignant change. Relevance of tumour markers is studied in many studies. According to Kikkawa et al 9 it was found that CEA (Carcinoembryonic antigen) was the best screening marker followed by SCC (Squamous cell carcinoma) antigen, both of these being superior to CA-125 and CA-19-9. It was finally recommended that measurement of CEA and SCC Ag levels in patients aged 45years or older, who have mature teratoma like ovarian tumour larger than 9.9cm in its greater diameter would provide a effective clinical strategy for preoperative risk assessment and help in making differential diagnosis between mature teratoma and SCC in mature teratoma. In yet another study Mori et al 10 reported that age >40years and serum SCC Ag >2.5ng/ml were77% sensitive and 96% specific for malignant transformation which has also been useful in monitoring for recurrent disease. Tumor imaging characteristics which may aid preoperative risk assessment have also been studied. According to Lai et al 11 characteristic CT scan findings such as adnexal mass with fat, calcification, soft tissue component and areas of invasion through the teratoma wall are highly suggestive of associated malignancy. Kido et al 12 on Magnetic resonance imaging correlated malignancy with presence of solid component with contrast enhancement, transmural or trans-septal extension, evidence of adherence to the surrounding structures, necrosis and haemorrhage. Regarding optimal management careful gross inspection of the tumor and frozen section analysis are essential whenever there is a preoperative suspicion of malignant transformation complete tumor excision and proper staging are integral to prognosis. Whole pelvis radiation and concurrent weekly platinum based chemotherapy may be beneficial in patients with stage III disease. Patient with stage III disease have poor prognosis and should be offered platinum based chemotherapy regimens
CONCLUSION
This case emphasizes on the diagnosis of malignant transformation of mature cystic teratoma because the great difference of prognosis in tumors with and without malignant change. It also highlights the importance of finding the association between clinical, radiological, biochemical and pathological findings in a middle aged female with ovarian tumor.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature of this article has been reviewed and discussed.
References:
REFERENCES
1. Genadry R, Parmley T, Woodruff J D. Secondary malignancies in benign cystic teratoma. Gynecoloncol 1979;8:246-51.
2. Stamp G W H, McConnell E M. malignancy arising in cystic ovarian teratomas. A report of 24 cases. Br J ObstetGynaecol1983;90:671- 75.
3. Hirakawa T, Tsuneyoshi M, Enjoji M. Squamous cell carcinoma arising in mature cystic teratoma of the ovary. Clinicopathologic and topographic analysis. Am J Surg Pathol 1989;13:397-405.
4. Hurwitz JL, Fenton A, McCluggage WG, McKenn S. Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series. BJOG 2007 Oct; 114(10):1283-7.
5. Itoh H, Wada T, Michitaka K et al. Ovarian teratoma showing a predominant haemangiomatous element with stromal lutenization: report of a case and review of literature. Pathol Int 2004;54:279-84.
6. Tseng C J, Chou H H, Huang K G et al. Squamous cell carcinoma arising in mature cystic teratoma of the ovary. Gynecol oncol 1996;63:364-70.
7. Vartanian R K, McRae B, Hessler R B. Sebaceous carcinoma arising in a mature cystic teratoma of the ovary. Int J Gynecol Pathol 2002;21:418-21.
8. Ronnett B M, Seidman J D. Mucinous tumours arising in ovarian mature cystic teratomas: relationship to the clinical syndrome of pseudomyxomaperitonei. Am J Surg Pathol 2003;27:650-57.
9. Kikkawa F, Nawa A, Tamakoshi K, et al. Diagnosis of Squamous cell carcinoma arising from mature cystic teratoma of the ovary. Cancer 1998 ; 82(11):2249-55.
10. Mori Y, Nishii H, Takabe K, et al. Preoperative diagnosis of malignant transformation arising from mature cystic teratoma of the ovary. Gynecol Oncol 2003; 90(2):338-41.
11. Lai PF, Hsieh SC, Chien JC, Fang CL, Chan WP, Yu C. Malignant transformation of ovarian mature cystic teratoma: Computerized tomography findings. Arch Gynecol Obstet 2005;271(4):355-57.
12. Kido A, Togashi K, Konoshi I, et al. Dermoid cysts of the ovary with malignant transformation: MR appearance. Am J Roentgenol 1999;172(2):445-49.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





