IJCRR - 6(12), June, 2014
Pages: 43-48
Date of Publication: 23-Jun-2014
Print Article
Download XML Download PDF
CULTURAL PRACTICES ASSOCIATED WITH FEEDING AMONG UNDERFIVECHILDREN IN A RURAL AREA: A CROSS SECTIONAL STUDY
Author: Vijayashree Mathad, Shivprasad S
Category: Healthcare
Abstract:Introduction: Cultural practices associated with faulty feedingamong underfive is one of the major problems, which is exaggerated by discarding of colostrums, giving of prelacteal feeds and wrong weaning practices. Objective: To assess the cultural practices associated with feeding among under fives. Material and Method: This cross sectional study was conducted in Kakati-A sub centre, under Primary Health Centre Vantamuri of Belgaum district. The sample size was 290. Data collection was done using pre-designed and pre-tested questionnaire.
Keywords: Under fivechildren, Culturalpractices, Rural area, Breast feeding, Weaning.
Full Text:
INTRODUCTION
Cultural practices regarding rearing of underfive children plays a vital role in the growth and development of underfive children. Various myths associated with culture like discarding of colostrums, giving prelacteal feeds, improper weaning foods has serious implecation on the health status of underfive children. Proper feeding practices which includes early initiation of breast feed, avoiding prelacteal feeds and exclusive breast feeding for 6 months and timely weaning are important determinants of growth and development of under five children.1 Exclusive breast feeding protects the child from various infections like gastrointestinal and respiratory tract and also promotes Cognitive and immunological growth. Weaning prior to 6 months may lead to infectious diseases like diarrhea due to inadequate hygiene and the food introduced in developing countries are of concern due to its low energy and nutrient intake.2 Breast-feeding lowers thefrequency and duration of acute respiratory infection and diarrhea ininfants under six months of ageand delayed weaning leads to growth deficiency.3, 4, 5 Optimal under five child feeding practices and appropriate complementary feeding prevents 6% of mortality among under five children.6 According to World Health Organisation (WHO) and systematic review from the Bellagio Child Survival Study Group about1.3 million child deaths could be prevented by 6 months of exclusive breast feeding and continued breast feeding for 1 year and improved complementary feeding. Consequences of faulty feeding practices are poverty reduction and poor socioeconomic development.7, 8 According to the United Nations declaration “the child shall enjoy special protection and shall be given opportunities and facilities by law and order and by means to enable him to develop physically and mentally in a healthy and normal manner and in a condition of freedom and dignity”. In the millennium declaration of September 2000, member states of the United Nations made a most passionate commitment to address the crippling and multiplying misery that grip many areas of the world. Governments set a date of 2015 by which they would meet the Millennium Development Goals. Among this, the first goal is to eradicate extreme poverty and hunger, which is measured by the prevalence of underweight children. The target is to halve the burden of under nutrition. The next important goal with regards to children is to achieve two third reduction in under 5 mortality and infant mortality by 20159 Proper feeding practices constitute an important component of child rearing along with socio demographic and cultural practices. There is an urgent need for education and promotion of proper feeding practices and child care among mothers of under five children.10 Meager amount of information is available regarding the cuktural practices associated with rearingof under five children in this part of the nation and in our field practice area. Hence the present study was undertaken to evaluate the cultural practices and the socio demographic factors associated among children aged under five in Kakati-A sub centre.
MATERIAL AND METHODS
Source of data The present study was conducted in Kakati-A sub centre, under Primary Health Centre Vantamuri of Belgaum district. It was a cross-sectional study conducted over a period of 10 months from March to December 2010. Eleven Anganwadicentres were providing non-formal pre-school education and rendering other services under Integrated Child Development Service Scheme in the village. A total of 290 underfive children were included in the study. The data was collected by interviewing the caretaker after obtaining the informed consent. Information was collected on socio-demographic variables and feeding practices using pre-designed and pre-tested questionnaire.
DATA ANALYSIS
Data was analyzed and expressed as percentages. Chi-square test was used to evaluate association between socio- demographic variables and cultural practices.
ET The study was approved by the institutional HICAL CONSIDERATIONSethics committee and written informed consent was taken from the parents or caregivers of the child.
RESULTS
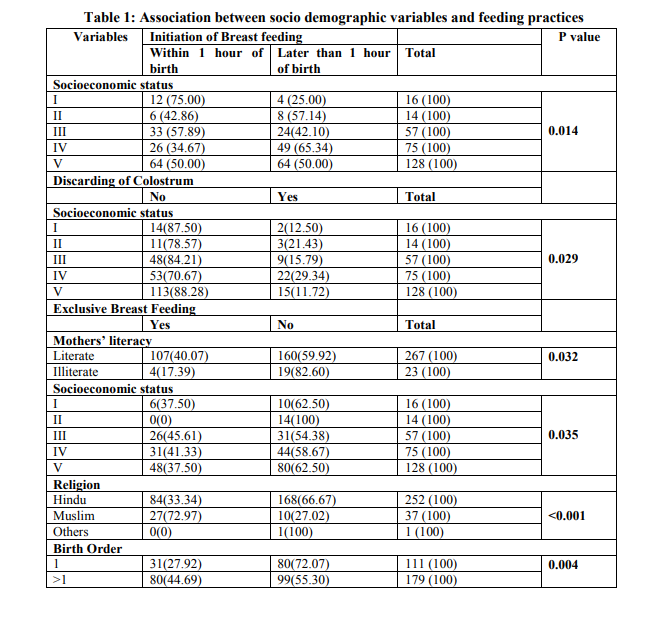
Basic information was obtained from290 householdsresiding in rural area of south India aged 0-5 years, 155(53.44%) were male and 135(46.55%) were female children. With regards to age distribution it was observed that in 0-12 months age group 19 (6.55%), in 13-24 months age group were 63 (21.73%), in 25-36 months 62 (21.38%), similarly in 37-48 months 59 (20.34%) and 49-60 months age group were 87 (30.00%). Majority 252 (86.90%) children were Hindus and with regards to socio-economic status, 203 (70.00%) belonged to Classes IV and V according to modified B.G. Prasad’s classification. Maximum 179 (61.94%) of underfive children fathers occupation was coolie and 260 (89.96%) of mothers were housewives. The literacy rate of underfive children fathers and mothers was 95.17% and 92.07% respectively.In context to birth order, 127(43.79%) of the children were of 2nd Birth order, 111(38.27%) of 1st Birth order, and 52 (17.94%) where of 3rd, 4th and 5th Birth order.With regard to type of family 149 (51.38%) of the children belonged to the nuclear family, 98 (33.79%) to three generation family, 38 (13.10%) to joint family and 5 (1.72%) belonged to problem family. Majority 168(58.13%) of the mothers got the information regarding breast feeding practices from health care provider, 61(21.10%) from their mother, 55(19.03%) from their mother in law and 5(1.73%) mothers were self informed or got information from sisters and neighbours. 50(17.30%) mothers discarded the colostrum. The reasons cited were: they felt the colostrum was dirty milk 21(42.00%), told by mother in law 12(24.00%), thought not good for baby 9(18.00%) and told by mother and sister, causes diarrhea, evil spirits milk and toxic for child. Most of them 245(84.78%) practiced demand feeding as compared to time bond feeding. According to feeding practices followed by mothers 141(48.79%) children were breast fed within one hour of birth, 53(18.34%) children were started within 1-6 hours, and others 95(32.76%) started later than 6 hours. Prelacteal feeds which is considered as a major wrong practices by WHO was given by 124 (42.76%) of mothers. The common Pre lacteal feeds given to newborn were honey, sugar water and plain water. Exclusive breastfeeding of 6 months as recommended was not practiced by most of the mother, which included early initiation of top feeding before 6 months by 179(61.72%) mother, mainly during 4th month the top feeds included 101(34.83%) buffalo’s milk, 55(18.97%) cow’s milk, 19(6.55%) cerelac and 4(0.79%) children were given goats milk. And delayed weaning later than 6 months was seen in 87(30.00%) children. Correct feeding practicesincluding initiation of breast feeding, feeding colostrumand not giving prelacteal feeds was significantly associated with socio economic status (p<0.05).Correct feeding practice of exclusive breast feeding of 6 months was significantly associated with mothers literacy (p=0.032), socioeconomic status (p=0.035), religion (p<0.001) and birth order (p=0.004). Correct weaning at 6 months was significantly associated with religion (p=0.022) of the child (Table 1,2)
DISCUSSION
According to a study done in of Delhi and Nepal regarding infant and child feeding practices, it was observed that only 16.7% mothers initiated breastfeeding within one hour, 48.3% mothers practiced complementary feeding during 6-9 months and exclusive breastfeeding rate (0-6 months) has been found to be 60.5% and 54.8% mothers discarded the colostrum which is comparable to the result of this study. And initiation of breastfeeding wasassociated with only two variables type and size of family, with smaller sized and nuclear families lesslikely to initiate early breastfeeding. Where as in this study there was association betweensocio economic status, mother’s literacy status and birth order. The main problems revealed from various studies were late initiation of breastfeeding, low rates of exclusive breastfeeding, and inappropriate complementary feeding practices.10,11,12,13 In a study conducted at Varanasi rural district, 1.19% of rural children were delayed of breast feeding by one day and the colostrums was discarded in 90% children, pre-lacteal feeds were commonly given, like goat’s milk and boiled water with honey and sugar water in 56.55% of the children which is similar to the data of this study which shows 42.76% were given prelacteal feeds. 14According to NFHS 3 the percentage of children who were given exclusive breast-feeding for 6 months was found to be 59% in Karnataka which is more than this study which revealed 38.28%.11 Our study has shown that the practice of discarding colostrum has declined from previous observation of 45% to 17.30%.7 Regarding pattern of breastfeeding, over 84.78%of the mothers reported breastfeeding on demand or used acombination of demand and regular feeding, which is recommended by the WHO for the childto have adequate nutrition.15 Only 38.28% of the mothers in our study started complementary feeding at 6 months which is the ideal age of starting. Almost 30% of the mothers started complementary feeds at a much earlier age than recommended by the WHO. At 4 months, 61.72% of mother had started complementary feeding for their babies which is less than other studies. By 7 months 38.3% ofthe mothers had still not started complementaryfeeding. This is an incorrect practice because delayed weaning effects the nutritional status of children.16
CONCLUSION
Majority of the mother’s incorrect cultural practicesin feeding was associated with socio economic status, literacy and birth order. Therefore the female literacy needs to be given more importance. The need for the family planning should be emphasized to the couples at individual basis. Hence appropriate feeding practices as per the guidelines of WHO is to be given importance. Healthy community will result in better contribution to Nations growth and prosperity.

References:
REFERENCES
1. Teresa G, Juan R, Hortensia M,3 Monterrubio E and Jaime S. Poor Compliance with Appropriate Feeding Practices in Children under 2 y in Mexico Cited from jn.nutrition.org by guest on July 26, 2012
2. Victora C, Smith PG, Vaughan JP, Nobre LC, Lombardi C, Teixeira AM et al. Evidence for protection by breast-feeding against infant deaths from infectious diseases in Brazil. Lancet. 1987 (2) 319–22.
3. Brown K, Black R, Roman G, Kanashiro H.Infantfeeding practices and their relationship with diarrheal and other diseases in Huascar (Lima) Peru. Pediatrics J Nutr. 1997 (127) 436–4.
4. Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S, Collet JP, Vanilovich I, Mezen I, et al. Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA. 2001 (285) 413–20
5. World Health Organization. Complementary feeding of younger children in developing countries: a review of current scientific knowledge. Geneva: WHO/NUT/98.1; 1998.
6. Apurba S, DiptaK,Mukhopadhyay, Tanmay K. Panja, Asit B. Saren, Nirmal K. Mandal, and Akhil B. BiswasInfant- and Young Childfeeding Practices in Bankura District, West Bengal, India J HEALTH POPUL NUTR 2010 Jun;28(3):294-299
7. National Family Health Survey. http://www.nfhsindia.org/data/ka-pre.pdf. (Cited on 24-12-2010).
8. Katiyar GP, Agarwal DK, Tripathi AM, Agarwal KN. Feeding practices in Varanasi district. Indian Pediatrics. 1981; 18(1): 65-70.
9. Bloss E, Wainaina F and Bailey RC. Prevalence and predictors of underweight, stunting and wasting among children aged 5 and under in western Kenya. Journal of Tropical Pediatrics. 2004; 50 (5): 260-270.
10. Dinesh K, N.K. Goel, Poonam C. Mittal and PurnimaMisra Influence of Infant-feeding Practices on Nutritional Status of Under-five Children Indian Journal of Pediatrics, 2006(73) 417-422.
11. . David O, Kirti M,Tumbahangphe,DejShrestha et al. Cross sectional, community based study of care of newborn infants in Nepal. BMJ 2002 (325) 10-63
12. Subba SH, TS Chandrashekhar, Binu VS, Joshi HS4, Rana MS, Dixit SB Infant feeding practices of mothers in an urban area in Nepal Kathmandu University Medical Journal 2007 (5) No. 1. 17, 42-47.
13. Apurba S, Dipta K, Mukhopadhyay, Tanmay K, Panja, Asit B et al. Infant- and Young Child-feeding Practices inBankura District, West Bengal, India.J HEALTH POPUL NUTR 2010 Jun;28(3):294-299
14. Katiyar GP, Agarwal DK, Tripathi AM, Agarwal KN. Feeding practices in Varanasi district. Indian Pediatrics. 1981; 18(1): 65-70.
15. Complementary feeding of young children in developing countries: A review of current scientific knowledge. WHO/NUT/98.1
16. Moffat T. A bio-cultural investigation of the weanling's dilemma in Kathmandu, Nepal: do universal recommendations for weaning practices make sense? - J Biosocial Sciences. 2001; 33(3): 321-38.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





