IJCRR - 6(13), July, 2014
Pages: 51-57
Date of Publication: 12-Jul-2014
Print Article
Download XML Download PDF
CLINICAL STUDY OF MUTLAZIMA QABL HAIZ (PREMENSTRUAL SYNDROME) AND ITS MANAGEMENT WITH UNANI FORMULATION - A RANDOMIZED CONTROLLED TRIAL
Author: Hafeeza, Wasia Naveed, Ismath Shameem, K. Tabassum
Category: Healthcare
Abstract:Background and Objectives: Mutlazima Qabl Haiz (Premenstrual Syndrome) is a group of menstruation related cyclical disorder manifested by emotional and physical symptoms in the second half of the menstrual cycle, which subsides after the beginning of menstruation. During the reproductive years, 80-90% of menstruating women experience symptoms like breast pain, bloating, acne, constipation, mood swings, irritability and depression that fore warns them of impending menstruation. The objective of the study was to evaluate the efficacy of Tukhme Sambhalu (Vitexagnuscastus) and Arq Pudina (Menthapiperita) in the management of Mutlazima Qabl Haiz. Methods: A single blind, randomized placebo controlled study was carried out in Gynaec OPD of the Institute?s Hospital, Bangalore. Patients were randomly allocated to test (n=30) and control (n=30) groups. Patients in the age group of 13-40 years with regular menstrual cycle were included in the study irrespective of marital status and parity. In test group, Tukhme Sambhalu1 gm and Arq Pudina 36 ml were administered orally twice daily, 10 days prior to menstruation in every cycle for 3 consecutive months. In control group placebo was given for the same duration. Severity of Premenstrual Syndrome was assessed by Premenstrual Tension Syndrome Scale and reduction in the Premenstrual Tension Syndrome Scale score was noted in each cycle. The data were analyzed using Analysis of variance - one way with Turkey Kramer Multiple pair comparison test and Premenstrual Tension Syndrome Scale scores of the two groups were compared by Chi Square test. Results: In test group, 70% patients were cured while 16.66% and 10% were relieved and partially relieved respectively, while 3.33% patients showed no response. In control group, the cured, relieved, and partially relieved patients were 23.33%, 23.33% and 20% respectively where as 33.33% patients showed no response. Significant reduction in the Premenstrual Tension Syndrome Scale scores was observed in test group than compared to control group (p< 0.01). Interpretation and Conclusion: The test drugs, Tukhme Sambhaluand Arq Pudina were effective in reducing the somatic and psychological symptoms of Mutlazima Qabl Haizas compared to placebo.vvv
Keywords: Premenstrual Syndrome; Premenstrual Tension Syndrome Scale; Vitexagnuscastus; Menthapiperita.
Full Text:
INTRODUCTION
Premenstrual Syndrome is the cyclic appearance of one or more of a large constellation of symptoms just prior to menstruation occurring to such a degree that life style or work is affected followed by a period of time entirely free of symptoms. 1 It is a functional disorder that affects the personal and emotional life of a woman irrespective of age, marital status and parity. The symptoms are variable that occur 7 10 days prior to menstruation, disrupts the life of a woman temporarily and subsides with the onset of menses to recur again in the next cycle. Approximately 40% of menstruating women experience luteal phase symptoms that are bothersome; for 25% these are annoying but do not impair functioning; for 10 15%, the symptoms are severe and report significant impairment of one or more areas of aily life. 2,3 Mutlazima Qabl Haiz is the term framed from the Arabic dictionary 4,5 in which syndrome is translated as „mutlazima’, pre stands for „qabl’ and menstrual is the word given for ‘haiz’. No such term was coined by ancient Unani Physicians but they had given a description on premenstrual features. The ancient physicians mentioned that, imtelayikaifiat exist in the premenstrual phase which leads to number of features. It is well studied that surge of akhlatmuharrika (hormones) are responsible for accumulation of body fluid in tissue spaces during premenstrual phase and this theory correlates with the concept given by IbnSina 6 and others. Premenstrual Syndrome may have an onset at any time during the reproductive years and once symptoms are established, they tend to remain fairly constant until menopause. It is a psychological and somatic disorder of unknown aetiology. The exact cause of PMS is not known, but it is thought to be related to changes in hormone levels related to the menstrual cycle 9. In 1931 Frank was credited with the first published description of the “Premenstrual Tension”. In 1953, Greene and Dalton called this conditionas “Premenstrual Syndrome” to allow the inclusion of both somatic and psychological complaints in the symptom complex 10 While there is no cure for PMS, the symptoms can be successfully managed with lifestyle changes, dietary modifications and supplements, hormone treatment and medications 11 . It has been reported that herbal medicine is useful in relieving the symptoms of PMS 12, 13. In addition clinical trials demonstrated that women taking chaste berry tree had significant improvements in irritability, depression, headaches, and breast tenderness. Theoretically, it may interact with hormones or drugs that affect the pituitary gland 14 . The main objective of the study was to evaluate the efficacy and safety of Tukhme Sambhalu and ArqPudina scientifically in the management of Mutlazima Qabl Haiz
MATERIALS AND METHODS
Study design: A placebo controlled randomized single blind study was undertaken in the Dept of Ilmul Qabalatwa Amraze Niswan, National Institute of Unani Medicine, Hospital, Bangalore. Study was completed within the duration of one and half year. Study was started after obtaining the ethical clearance from the Institutional Ethical Committee Participants: Patients were randomly allocated to test (n=30) and control (n=30) groups. Randomization was done by lottery method. Written informed consent was obtained from each participant before entering into the study. Selection criteria: Patients in the age group of 13 40 years with regular menstrual cycle were included in the study irrespective of marital status and parity. Exclusion criteria were pregnant and lactating women, irregular menstrual cycles, organic pelvic pathology, major psychiatric disorders, hormonalcontraceptives, medication for PMS in last 2 months and systemic diseasesetc. Procedure of the study: In each included patients, biochemical test such as LFT (SGOT, SGPT, Alkaline phosphatase) and RFT (Blood Urea, Sr. Creatinine) were carried out along with specific investigations like Serum Progesterone and Serum Prolactin to evaluate the safety and efficacy of the research drug apart from routine investigations. Diagnostic criteria: Premenstrual Syndrome can be diagnosed if the patient reports at least one of the following psychological and somatic symptoms during the first five days before menses in each of the three prior menstrual cycles: Psychological symptoms like Depression, Angry outbursts, Irritability, Anxiety, Confusion, Social withdrawal etc Somatic symptoms like Breasttenderness, Abdominal bloating, Headache, Swelling of extremities etc These symptoms are relieved within 4 days of the onset of menses without recurrence until at least day 13 of cycle. The symptoms are present in the absence of any pharmacologic therapy, hormone ingestion, drug or alcohol use. The symptoms occur reproducibly during two cycles of prospective recording. The patient suffers from identifiable dysfunction in social or economic performance.
INTERVENTION
Test Group: Research drug comprised of Tukhme Sambhalu VitexAgnusCastus 15 and Arq Pudina (Menthapiperita 15which possesses antispasmodic, analgesic and diuretic properties. Preparation, Administration & Dosage The seeds of Tukhm Sambhaluwere cleaned, finely powdered, sieved and filled in 500 mg capsules & administered orally in a dose of two capsules per day. Arq Pudina was purchased from the market (prepared as per the formula of Bayazekabir 13 ) and administered orally in a dose of 36mltwice daily. Control Group:Wheat flour was filled in same colourcapsules as that of research drug and given with plain water containing few drops of ArqBadiyan for change of flavour as placebo. Duration of treatment:In both the groups, drugs were given 10days prior to menstruation for 3 consecutive cycles. Assessment cum follow up: Patients were followed for three consecutive cycles during treatment and one cycle after treatment. During this period, improvement in PMTS score was assessed. Patients were also enquired for any adverse effect of drug during the trial. Repeat LFT, RFT, Serum Progesterone and Serum Prolactin was carried out after completion of treatment to evaluate the effect of drug. Parameters for Evaluation of Efficacy of Research Drug Subjective Parameters Breast tenderness, muscle cramps, nausea, anorexia, abdominal bloating, headache, depression, irritability, loss of concentration, sleep disturbances, altered libido, peripheral oedema etc. Objective Parameters: Premenstrual Tension Syndrome Scale (PMTS) 16, 17, 18 Serum Progesterone and Serum Prolactin PMTS scoring: The scale ranges from 0 to 36. “0” is given for no features and “36” are given for full features of the Syndrome. For statistical purpose, the scale was divided into 5 categories as follows: Severity of PMS o Normal (0 7) o Trivial (8 14) o Mild (15 21) o Moderate (22 28) o Severe (>28) Serum Progesterone and Serum Prolactin: The pre and post treatment basal levels of Sr. Progesterone and Sr. Prolactin were measured on nd day of menstrual cycle preferably in fasting condition. Sr. Progesterone: 0.20 1.50ng/ml 19 Sr. Prolactin: 2 29 ng/mL 20 Analysis of result: Results were analyzed on the basis of 4 categories:
Cured: When symptoms abolished completely and severity of PMTS score reduced to normal. Relieved: When PMTS score reduced from severe to mild. Partially relieved: When PMTS score reduced from severe to moderate or moderate to mild. No response: when PMTS score remains in the same category during the trial. Statistical Analysis: Effect of research drug on Serum Progesterone and Serum Prolactin was assessed by ANOVA one way with Dunn?s Multiple Comparison test. Effect of research drug on PMTS scoring was assessed by ANOVA one way with Turkey Kramer Multiple Comparison Test. Over all response of the research drug was assessed by χ² (chi square) test.
RESULTS AND DISCUSSION
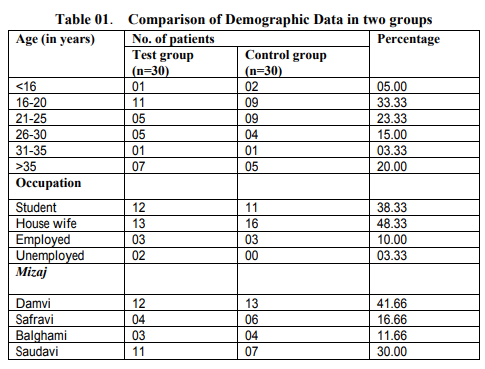
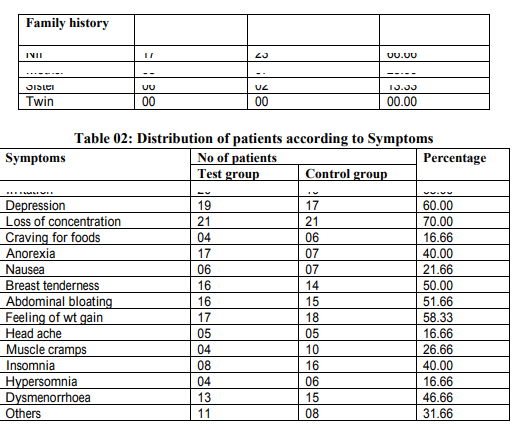
A placebo controlled randomized single blind study was carried out in the Dept. of IlmulQabalatWaAmrazeNiswan, NIUM, Hospital, Bangalore. The study was managed by Tukhme Sambhalu and Arq Pudina and its effect was assessed by using Premenstrual Tension Syndrome Scale (PMTS). In this studypatients between the age group of 13 40 years were included and the highest incidence of PMS was observed in the age group <20 years; this may be dueto the survey conducted among the students of schools and colleges. This observation is supported by the study conducted by Johnson SR (1987) who stated that PMS can begin at any time during the reproductive years and studies that include teenagers show approximately the same percentage of severe symptoms as among the older subjects. 21This study shows that PMS was common in patients with middle socio economic status, and it is a fact that patients attending the NIUM OPD are from low and middle income group. Positive family history of PMS was found in 38.33% patients and studies suggest that women whose mothers report PMS are more likely to develop PMS 22 . No relation was observed with fertility and parity among Premenstrual Syndrome. Highest incidence of PMS was found in patients with Damvimizaj (41.66%), when compared to Saudavi (30%) and Safravi (16.66%) and least in patients with Balghamimizaj (11.66%). This correlates well with the theory proposed by Unani physicians who states that imtelayikaifiat (plethora) exist in premenstrual phasewhich points towards the dominance of khilt Dam (Table 01) As there is no specific test or method to objectively measure the symptoms of the Premenstrual Syndrome, patient?s self report remains probably the sole criteria for its determination. As stated earlier, the commonest somatic symptoms are fatigue, breast tenderness, abdominal bloating, weight gain and head ache, less common being gastro intestinal symptoms like nausea, vomiting, diarrhoea or constipation. Among psychological symptoms irritability, anxiety, depression, loss of concentration, crying spells, feeling of isolation are common. In this study, the psychological symptoms were predominant over the somatic symptoms. This finding is in accordance with the study conducted by Ellen et al (1985) 23 Dysmenorrhoea was reported in 46.66% patient and it has been mentioned in the literature report that Patients who have PMS often have dysmenorrhoea as a major component of the symptom complex 22 .(Table 02) The research drugs consist of Tukhme Sambhalu which is a potent emmenagogue and antispasmodicdrug 15 . A study conducted at Germany (2001) on Tukhme Sambhalu shows that the fruit was effective and well tolerated remedy for the symptoms of PMS and it also states that the effect of Tukhme Sambhaluwere similar to those of corpus luteum 24 Further it was stated that Tukhme Sambhalu affects progesterone and prolactin level and it has got dopaminergic effect 25 but no significant changes were observed in Serum Progesterone and Serum Prolactin level in this study.(Table 03) Pudina posses emmenagogue and diuretic properties, expels out sauda and has mufarreh effect which reduces irritability and anxiety 15 Thus the combination of Tukhme Sambhalu and Arq Pudina had shown a good response in the relief of symptoms of PMS as both these drugs act as potent anti spasmodic, emmenagogue and diuretics, hence reduces the imtelayikaifiat responsible for PMS. The results derived from PMTS rating scale were considered as strongly significant with p< 0.001 (Table 04) Theoverall response of the research drugswas as follows: In test group 70% patients were cured while 16.66% and 10% patients were relieved and partially relieved respectively, while 3.33% patients showed no response. In control group, the cured, relieved, and partially relieved patients were 23.33%, 23.33% and 20%, respectively where as 33.33% patients showed no response. Significant reduction in the Premenstrual Tension Syndrome Scale scores was observed in test group than compared to control group with p<0.01. (Table 05) Therefore it can be inferred that the test drugs, Tukhme Sambhalu and Arq Pudina were safe and effective in reducing the somatic and psychological symptoms of Mutlazima Qabl Haizas compared to placebo; therefore it can be used as an alternate treatment for PMS. This study is the first of its kind in the treatment of PMS, so it is not possible to draw any comparison with other trials. The limitation of the study was small sample size, short period of follow up and fixed dose of research drugs. Future trial can be carried out on large sample size for longer duration.
ACKNOWLEDGEMENT
We are thankful to the Director, National Institute of Unani Medicine, Bangalore for providing all facilities to complete the research. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript.The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
1. Chanana C, Rehman SM. Premenstrual syndrome. Obs Gynae Today 2006; 9 (8): 452 4.
2. Johnson SR. Premenstrual Syndrome, Premenstrual Dysphoric Disorder and Beyond: A Clinical Primer for Practitioners. ObstetGynaecol 2004; 104 (4):845 59.
3. Sternfeld B, Swindle R, Chawla A, Long S, Kennedy S. Severity of Premenstrual Symptoms in a Health Maintenance Organization Population. ObstetGynaecol 2002;99:1014 24.
4. www.languagesource.com/acatolog/Arabic_Tr anslation_Software_Arabic_Al_Wafi.html. cited on27.11.06
5. Anonymous. The Unified Medical Dictionary. Eng Ara Fren.3 rd ed. Switzerland: Council of Arab ministers of health; 1983:642.
6. IbnSina. Al QanoonFilTib. Vol II. (Urdu Translation by Kantori GH). New Delhi: IdaraeKitabusShifa; 1981: 331.
7. Kapur A. Use of Evening Primrose Oil in Premenstrual Syndrome. ObstetGynaecol 2001; 6 (11):690 695.
8. Kessel B. Premenstrual Syndrome: Advances in Diagnosis and Treatment. ObstetGynaecol of North America 2000;27(3): 625 639.
9. http://www.webmd.Com/women/pharmacist 11/herbal treatments for pms. Cited on06/12/2013.
10. Copeland LJ, Jarrell JF, McGregor JA. Textbook of Gynaecology. Philadelphia: WB Saunders Company; 1993: 403 413.
11. http://www.betterhealth.vic.gov.au/bhcv2/bhc articles.nsf/pages/premenstrual_syndrome. Cited on 04.12.2013.
12. Zulkifle MD. Physiochemical Basis of Temperament. Thesis submitted to the Department of Kulliyat, AKTC, U. P: Aligarh, AMU; 1993.
13. Kabeeruddin. BayazeKabir. VolII. Hyderabad:Hikmat Book Depot;1921:96.
14. http://altmedicine.about.com/cs/womenshealth /a/PMS.htm. Cited on 07.12.2013.
15. Kabeeruddin M. MaghzanulMufradat. New Delhi: Aejaz Publication; YNM: 170, 171, 358, 359.
16. Critchlow DG, Bond AJ, Wingrove J. Mood Disorder: History and Personality Assessment in Premenstrual Dysphoric Disorder. J clinPsychiatry 2001; 66(9): 688 93.
17. Haskett SM, Caroll BJ. Premenstrual Tension Syndrome: The Development of Research Diagnostic Criteria and New Rating Scales: Acta Psychiatry Scand 1980; 62(2): 177 90.
18. Steiner M, Steiner DL, Stein Berg S et.al. TheMeasurement of Premenstrual Mood Symptoms. J Affect Disord 1999; 53(3): 269 273.
19. Ann Le´vesque, Marc Letellier, Paul W. Dillon, and Andrew Gran. Analytical Performance of Bayer ImmunoEstradioland Progesterone Assays. Clinical Chemistry 1997; 43 (9): 1601–9.
20. Melmed S, Kleinberg D. Anterior pituitary. In: Kronenberg HM, Melmed S, Polonsky KS, Larsen PR, eds.Williams Textbook of Endocrinology. 11 th ed. Philadelphia, PA: Saunders Elsevier; 2008: Chap 8.
21. Johnson SR. The Epidemiology and Social Impact of Premenstrual Symptoms. linObstetGynaecol 1987; 30 (2): 367 76.
22. Lawrence N. Adolescent Health Care: A Practical Guide. 5 th ed. Lippincott: Williams and Wilkins; 2008: 678 9.
23. Freeman EW, Sondheimer S, Wein PJ, Baum, Rickets K. Evaluating Premenstrual Symptoms in Medical Practice. ObstetGynaecol 1985; 65 (4): 500 5.
24. Schellenberg R. Treatment for Premenstrual Syndrome with AgnusCastus Fruit Extract: Prospective, Randomized, Placebo Controlled Study. BMJ 2001; 332: 134 7.
25. Girman A, Lee R, Kligler B. An Integrative Medicine Approach to Premenstrual Syndrome. AmJObstetGynecol 2003; 188(5):
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





