IJCRR - 6(14), July, 2014
Pages: 54-57
Date of Publication: 22-Jul-2014
Print Article
Download XML Download PDF
CLINICO - MORPHOLOGICAL STUDY OF SKIN DISEASES
Author: R. Thamilselvi, K. Sivakami, Pammysinha, P.M. Subramaniam
Category: Healthcare
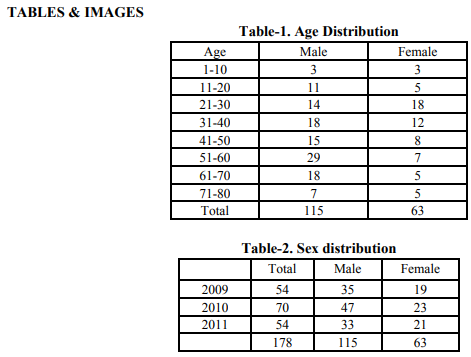
Abstract:Background: Skin diseases constitute a major public health problem. The pattern of skin diseases vary from one country to another country. Disease pattern also vary from tissue reactions to vesiculobullous lesions and malignant lesions. Aim: To analyze the clinico-morphological spectrum of skin lesions. Methods: A retrospective study was undertaken to determine the clinico-morphological spectrum of skin lesions from all the skin biopsies, received from Jan 2009 to Aug 2011 (2 and ½ years) in the Department of Pathology, Vinayaka Mission's KirubanandaVariyar Medical College, Salem. Results: A total of 178 cases were reviewed and analysed. The highest number of patients were in the age group of 51-60 years.The incidence of dermatological diseases was more in male patients than female patients. Cystic lesions (26%) were the commonest lesions followed by infectious diseases of skin (13.4%), malignant tumors of skin (13%), alteration in the dermal collagen (8%). Most common site for various skin lesions was extremities followed by scalp region. Clinically the lesionswerevarying from papule, macule, vesicles, nodules to ulcers. The two major tissue reaction patterns, the psoriasiform and the lichenoid reactions were commonly seen in this study. Conclusion: In our study, cystic lesions, infectious diseases and malignant tumors of skin were the most common disorders. The contribution of histopathology to the final diagnosis and there by treatment were significant.
Keywords: Dermatological diseases, Cystic lesions, Malignant tumors, Psoriasiform & Lichenoid reactions.
Full Text:
INTRODUCTION
Skin diseases constitute a major public health problem. The pattern of skin diseases vary from one country to another country. Disease pattern also varies from tissue reactions to vesiculobullous lesions and malignant diseases. The interpretation of skin biopsies requires the identification and integration of two different morphological features- the tissue reaction pattern, the lichenoid reactions and the psoriasiform reaction and other lesions with clinicomorphologicalpattern.
MATERIALS AND METHODS
A retrospective study was undertaken to determine the clinico-morphological spectrum of skin lesions from all the skin biopsies received from Jan2009 to Aug 2011 in the Department of Pathology, Vinayaka Mission’s KirubanandaVariyar Medical College, Salem. Specimens were received as punch biopsy or excision biopsy, in 10% formalin as fixative for histopathological examination. 2-3 μm sized sections were taken and stained with routine Hematoxylin and Eosin stain and special stains were used when necessary. All the cases were reviewed and analysed.
RESULTS
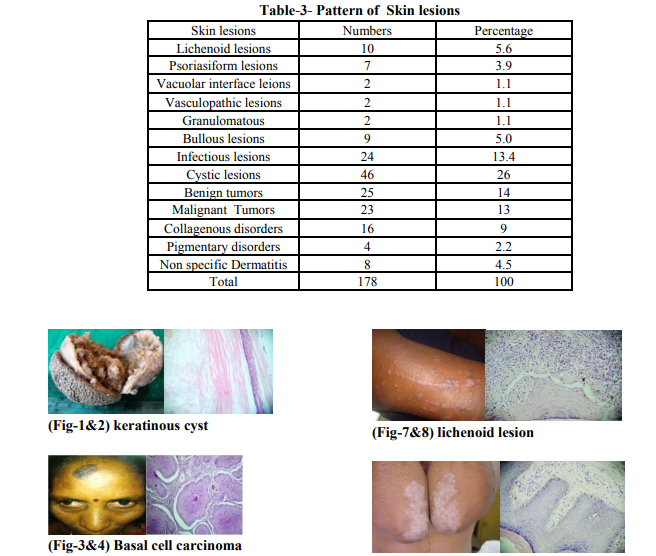
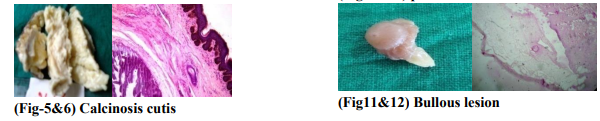
The age distribution pattern revealed that the maximum biopsies (20.2 %) were in the age range of 51-60 years. (Table-1) The incidence of dermatological diseases were more in males 115 cases (64.6%) than females. (Table-2) The anatomic distribution pattern showed that the upper & lower extremities were involved in the maximum number of cases (36.5%) followed by the scalp (13.4%) and neck (11.2%). Clinically the lesions varied from papule, macule, vesicles, nodules to ulcers & combination of all these. Cysts were the commonest skin lesions, among the cystic lesions, keratinous cyst (9.5%) (Fig-1&2) was the most common. In infectious diseases, Leprosy (10 cases 5.6%) was the commonest disease followed by Tuberculosis (6 cases 3.3%) and fungal infections (5 cases 3%). In neoplastic lesions, Basal cell Carcinoma (8 cases 4.4%) (Fig-3&4) was the commonest.In dermal collagenous diseases, calcinosis cutis (Fig 5&6) was the commonest (5 cases 3%) (Table-3) An analysis of the major tissue reaction patterns revealed that the most frequently encountered lesion was the lichenoid group (10 cases, 5.6%) (Fig 7&8) followed by psoriasiform lesion (7 cases 3.9%), (Fig-9&10) Bullous lesions 5%. (Fig11&12) Amongst the lichenoid group of lesions, lichen planus was the most frequentwhereas inpsoriasiform lesions, psoriasis vulgaris was the most common. DISCUSSION In the present study, maximum number of biopsies were seen in the 51-60 years of age, and the minimum number in the age range of 0-10 years. The sex distribution pattern of cases revealed that most of the patients were males ( 64.6%). Limbs were involved in the maximum number of cases (36.5%), followed by the Neck, face, eye (21.9%) and scalp (13.4%). Among the cystic lesions, keratinous cyst was the commonest as seen in literature. We found leprosy was the commonest disease as infectious lesion &majority of cases were presented as hypopigmented macules(1). Basal cell carcinoma (BCC) was themost common neoplasm and most frequently seen on the face (2) as in literature. In our study we had 5 cases of Idiopathic calcinosis cutis, which is cutaneous calcification of unknown cause with normal serum calcium.(3) Lichen planus was most frequently seen in the 20- 40 years of age, but the literature revealed the incidence is seenin 5 th - 6 th decades.(4 ) Lichen planus showed male preponderance in our series and is also described in the literature.Most of our cases of lichen planus occurred on the limbs as seen in the literature. (4,5)
The next most frequently seen lesion was psoriasis in the 40- 70 years of age range. Fry (6) mentioned that two-thirds occurred before the age of 30 years. Griffiths (7) and Bell et. al. (8). mentioned that classic psoriasis is seen in the older age. We found a male preponderance in psoriasis, however Bell et. al. (8) found a female preponderance and Fry found no sex predilection. Pemphigus vulgaris was the commonest lesion and seen in the 4th decade, as seen in literature Salmanpour et. al. (9) series and Aboobaker et. al. series.
CONCLUSION
In our study, cystic lesions were the commonest followed by infectious diseasesand malignant tumors of skin. Correlation of clinical diagnosis with the histopathological diagnosis was positive in 97.1% cases and negative in 2.8% cases. The contribution of histopathology to the final diagnosis and there by treatment were significant.
References:
1. Kar, P K. 1994. A clinic Pathological study of macular lesions in leprosy, Indian Journal of Leprosy, 66(4):435-442.
2. Erba P, Farhadi J, Wettstein R, Arnold A, Harr T, Pierer G. Morphoeic basal cell carcinoma of the face. Scand J PlastReconstrSurg Hand Surg. 2007;41(4):184-8
3. Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999; 106(4):746–50. 3.
4. James WD, Berger TG, Elston DM. Andrews' Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia (PA): Elsevier/Saunders; 2011. p. 516-8
5. Boyd AS, Neldner KH. Lichen planus. J Am AcadDermatol 1991;25:593-613.
6. Fry L. Psoriasis. Br J Dermatol 1988;119:445- 61.
7. Griffiths CE, Christophers E, Barker JN, Chalmers RJ, Chimenti S, Krueger GG, et. al. A classification of psoriasis vulgaris according to phenotype. Br J Dermatol 2007;156:258- 62.
8. Bell LM, Sedlack R, Beard CM, Perry HO, Michet CJ, Kurland LT. Incidence of psoriasis in Rochester, Minn, 1980-1983. Br J Dermatol 1991;127:1184-7.
9. Salmanpour R. Shalkar H, Namaki MR, Rahman-Shenar MR. Epidemiology of Pemphigus in south Western Iran- a
10 years Retrospective study(1991-2000) International Journal of Dermatology 2006, 45(2):23-5
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





