IJCRR - 6(14), July, 2014
Pages: 38-48
Date of Publication: 22-Jul-2014
Print Article
Download XML Download PDF
FEASIBILITY OF POST PARTUM INSERTION OFINTRAUTERINE CONTRACEPTIVE DEVICE- EXPANDING THE USE OF INTRAUTERINE CONTRACEPTIVE DEVICE IN POST PARTUM PERIOD - A CROSS SECTIONAL STUDY IN DEVELOPING COUNTRY, INDIA
Author: Sudha T. R. Banapurmath, Girija B. S. Dotrad, Nirmala Doreswamy, Shyamala
Category: Healthcare
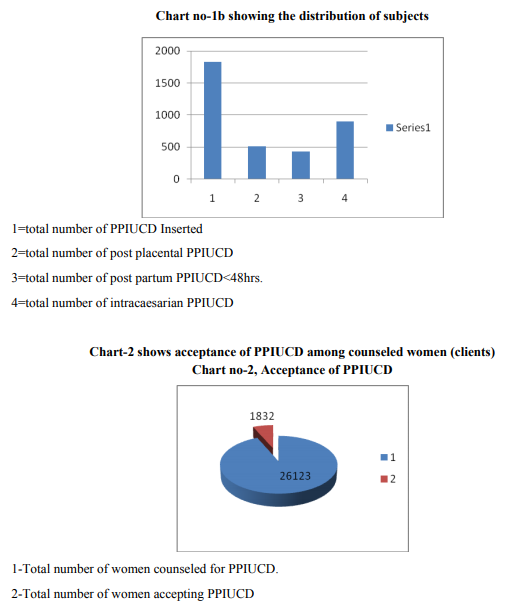
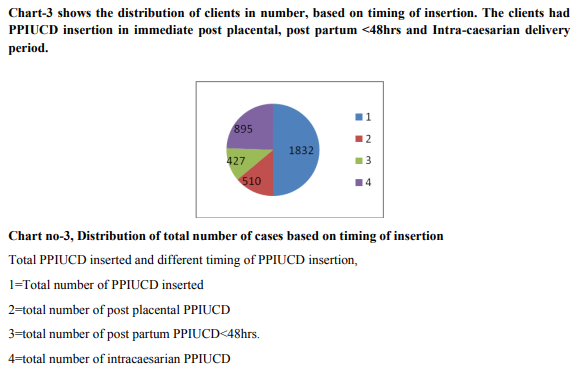
Abstract:Aim: Post partum contraception is the best evidence based intervention in prevention of pregnancy and abortion related maternal morbidity and mortality in the developing countries. The unmet need for contraception among women in the postpartum period can be effectively fulfilled by post partum insertion of IUCD, in a single visit under the Government scheme of providing free maternity services during institutional delivery. PPIUCD is an effective, safe, reversible method of long term contraception with high reported expulsion and low perforation rate, compared to interval insertion. Objective: To evaluate the acceptability, safety, efficacy and feasibility of PPIUCD as a method of post partum contraception. Study design: This is a prospective cross sectional study conducted between October 2011 to December 2013 at Sri Chamarajendra Government Hospital, Hassan, Karnataka, India. 26,123 pregnant women were counseled (clients) for Post partum IUCD insertion as a method of contraception in pregnancy, early in labor and in the immediate post partum period (< 48 hours). Among the clients, 1832(7%) accepted and had PPIUCD inserted under asepsis by skilled Obstetricians. The timing of PPIUCD insertion were- 510(27.8 %) post placental, 427(23.3 %) in immediate post partum period< 48hrs, and 895(49 %) Intra caesarian insertions. The side effects were minimal, Infection and perforation were 00%, pregnancy reported were 0%, Expulsion rate was 0.32 %( o6/1832), and Removal rate was 0.76% %( 14/1832). IUCD retention rate was 98.90% (1812/1832) at 14weeks post partum. Conclusion: PPIUCD is a feasible, safe and effective method of immediate postpartum contraception that may be practiced during a single visit for institutional delivery which may be continued as a long term reversible contraception.
Keywords: Post-partum intrauterine contraceptive Device (PPIUCD), Post placental, Client, Caesarian Delivery, Expulsion, Contraception, Counseling.
Full Text:
INTRODUCTION
The maternal health is one of the health indicators of the country. The antenatal, labor and postpartum period is the crucial period of optimal maternal care that influences the outcome of pregnancy. Poor spacing between pregnancies, the unmet need for post partum contraception may lead to intervention in an unwanted subsequent pregnancy. Postpartum insertion of IUCD (PPIUCD) is a method of post partum contraception that may be utilized to overcome the unmet need of contraception, in a single hospital visit during institutional delivery. The postpartum period following three months after delivery, weaning from breast feeding and resuming sexual activity among married couple, is the risk period for unintended pregnancy. This necessitates the use of some postpartum reversible contraception which is met by PPIUCD insertion. Approximately 27% of women in India practice birth to birth interval of <24 months and 34% between 24-35 months, a total of 61% women practice birth to birth to interval of < 36 months, 40% of women are not using any contraceptives for spacing. IUD-1.6%, natural method (LAM)- 5.4%, condom use-5.3%, and female sterilization34.2%, male sterilization 1.9% are the methods of contraception among the married couple in India1, 2 . Unmet need in India, in the first year after delivery is 65%6 . Postpartum LAM method is not reliable after three months following delivery2 . The introduction of GOI- JSY scheme for improvising implementation of Institutional delivery (GOI 2009) also provides adequate opportunity to generate clients for introduction of postpartum contraceptive services, thereby providing the women an access to immediate PPIUCD services. Provision of quality contraceptive services during the postpartum period by utilizing the opportunities of increased institutional deliveries is a critical intervention for ensuring maternal and child health besides population stabilization. To achieve this objective, postpartum IUCD has been introduced in the National Family Welfare Programme since March 2010 in several states. An evidence based practice of post partum IUCD insertion as post partum contraception suggests that it is a safe, easy and effective, long term method that can be provided immediately post placental, during caesarian delivery or in the immediate post partum period within 48 hours after delivery3, 5,6,9,10,11,14,18 . The postpartum period of stay at the hospital provides adequate time for motivation, counseling and convenience of easy insertion, implementation of postpartum contraceptive services during a period of high motivation, with few side effects. The woman goes home with a contraceptive method of her choice which also ensures in fulfilling her unmet need of contraception, in a single visit at the hospital5 .Several studies among women in China, Egypt, Mexico, Turkey, and Peru reveal PPIUCD as a popular, acceptable, and feasible method of contraception but they have reported high expulsion rates. This study is conducted, to evaluate the feasibility, acceptability, efficacy and safety of PPIUCD as an optional method of post partum contraception among women in India, where the IUCD acceptance is very low, due to non medical reasons. This study also is intended to evaluate PPIUCD as a method of intervention in reducing maternal mortality in developing countries.
MATERIAL AND METHODS
This is a prospective, cross sectional, cohort, study conducted between Oct 2011- Oct 2013 at Sri Chamarajendra Government Hospital, Hassan District, Karnataka, India to evaluate the acceptability, feasibility, safety, expulsion, and retention rate of PPIUCD among 1832 women in the postpartum period.
METHODOLOGY
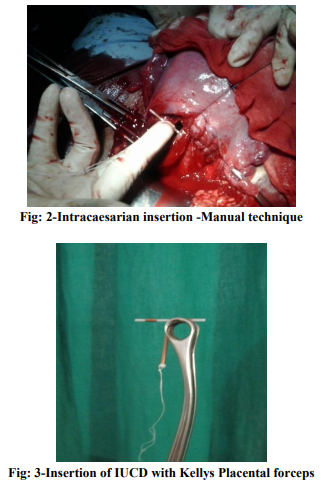
All the pregnant women attending the antenatal clinic at Sri Chamarajendra government hospital, Hassan, Karnataka, India. (population-1721669) were counseled during their antenatal visit regarding the benefits of birth spacing, advantages of choosing and availing postpartum contraception during their stay at hospital, child care, various methods available for post partum contraception and post partum sterilization, advantages of choosing long term temporary, reversible contraceptive methods, and PPIUCD. The method chosen for contraception was marked on their Antenatal records, andcalled as clients. Women in Early labor and in the post natal ward were counseled for PPIUCD. The insertion was done by skilled obstetricians under asepsis after informed consent (fig-2, 3). The standard infection prevention protocols were followed. The quality of PPIUCD services provided at the hospital were assessed and monitored as per the performance standards for immediate PPIUCD counseling and services, April 20113, 4.
The women after PPIUCD insertion were advised routine post partum care, and to report for follow up at 6, 10, and 14 weeks or earlier when necessary. A record of follow up was maintained at the post partum clinic. A telephonic follow up was done when a clinic visit was not feasible or to report symptoms, expulsion of IUCD or at the convenience of the client. The inclusion criteria in this study were as per Medical eligibility criteria(M.E.C)- 1and 2 that included all clients accepting for IUCD insertion in post partum period. Exclusion criteria (MEC criteria 3and 4) arechorioamnionitis, premature rupture of membranes of >18 hours, intractable post partum hemorrhage (atonic or traumatic) and abnormal uterine cavity.
However contraindications are few. This expands the client number for PPIUCD insertion. Limitations of PPIUCD as a method of post partum contraception are: High expulsion rate compared to interval insertion. The expulsion rate is 5-10%which means retention rate of 90-95%. Post placental and intra caesarian insertions have low expulsion rate. Expulsion rates may be reduced by appropriate fundal placement of IUCD which is acquired through skill training in PPIUCD insertion3, 5 .
RESULTS
The data of PPIUCD services provided, observations during follow up of clients were as shown in Observations (charts1a, b-chart 5).
Acceptibility
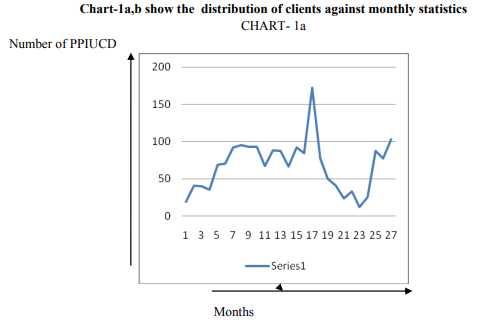
Acceptability for PPIUCD among women was 7.0%. The observation are as shown in charts 1and 2
Total number of monthly PPIUCD inserted as shown in chart-1
Observations:
1. Client characteristics
All the clients who accepted for PPIUCD insertion were in the reproductive age group (20-40yrs).
Follow up of clients: follow up of clients were conducted at 6, 10, and 14 weeks or earlier when necessary.During follow up, the observations were made regarding removal, expulsion and safety of PPIUCD. The Results were as followsEfficacy of PPIUCD as a contraceptive Efficacy of PPIUCD as contraceptive were assessed by pregnancy rate, Expulsion rate, removal and retention rate of IUCD. Pregnancy rate :- There were no pregnancies observed among clients in the study period. Hence the failure rate was 00% that shows that PPIUCD is efficient in prevention of pregnancy among the clients who continued to retain it. Expulsion of IUCD : 06/1832(0.32%) of clients reported spontaneous, expulsion within 10 weeks of insertion which was confirmed by clinical and Ultrasound examination. These clients were offered reinsertion but all of them refused. They were counseled for alternate methods of contraception. Missing strings Missing string was termed when the string was not seen at 6 weeks, at the external os of cervix, during per speculum vaginal examination of clients in the post partum clinic. Among the 289 clients followed for 14 wks post partum, missing strings during the follow up in the clinic was observed in 39 clients (13.5%). An ultrasound examination confirmed the presence of IUCD in the uterine cavity. Many clients who were examined clinically had the string curled in vagina or cervical canal. They were reassured and re-examined at 10 and 14 weeks. They continued with IUCD as a long term contraceptive. Safety of PPIUCD Safety of IUCD was assessed by the clients Reported Side effects and complications of IUCD such as infection, menstrual abnormality, perforation ,and expulsion. The complications were few and were managed symptomatically. They are shown in chart-5.
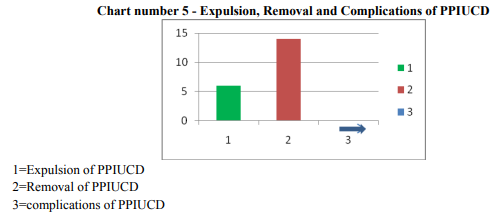
Rate of infection
None of the clients reported nor had infection (00%) in the present study. Menstrual abnormality There were no reports of menorrhagia nor any abnormal vaginal bleeding among the clients followed in the study period. Perforation of uterus No perforation of uterus by IUCD has been observed in the present study. Client reported symptoms Many clients reported to post partum clinic with lower abdominal pain and pricking sensation. They had urinary infection, constipation or non specific symptoms, and were reassured and treated accordingly. All these women continued to retain IUCD. Removal of PPIUCD 14/ 1832 clients requested for removal of IUCD due to personal and social reasons, but none got it removed for side effects such as infection, Menorrhagia and abdominal pain. Increase in awareness of advantages of PPIUCD, and reassurance by the attending health care worker later reduced the removal rate. Retention of IUCD 1812(98.90%) clients were willing to continue IUCD by 14 wks, 14 (0.76%) were not willing to get reinsertion of IUCD and preferred an alternate method of contraception. The Retention rate was 98.9%, which showed that PPIUCD was effective in meeting the unmet need of contraception in the post partum period.
DISCUSSION
Many studies have been published regarding the efficacy, safety of PPIUCD .This was a cross sectional study, at Sri Chamarajendra Government Hospital, Hassan District, Karnataka, India to evaluate the acceptability, feasibility, safety and efficacy of PPIUCD. Lara Ricalde R et. al. has reported an acceptance rate of 28.9% (1,024 /3,541) 6. In this study the acceptance rate was lower, probably due to low IUCD insertion rates in low resource settings in India. Mohammed et. al. observed that Acceptance rate was the same during antenatal and postpartum counseling, 26.4 and 31.8%, respectively10.. Indian experience 0f 2 years, PPIUCD services have been established in over 50 facilities across 19 states of India, with the Government of India undertaking more than 22,000 PPIUCD insertions in the target facilities, with 5% of women delivering in these institutions accepting PPIUCD as their choice of contraception17. In the present study the acceptance rate was higher (7%). The acceptability of intracaesarian placement of IUCD was highest followed by post placental IUCD insertion.
Among clients who accepted for PPIUCD, many refused for PPIUCD insertion due to demotivation by relatives and friends. This was observed as a major barrier for implementation of PPIUCD in this study. The rate of return for follow-up visit were 221 (94%), 210 (89%) and 183 (78%) at 6 weeks, 6 months and 12 months, respectively. Timing of IUCD insertion after vaginal and cesarean delivery were 74% and 26%. Continuation rates of IUCD were relatively high, 87.6% and 76.3%, at 6 and 12 months, respectively. The 1-year cumulative expulsion rate with CuT 380A device was 12.3%11. . In the present study the follow up was very low. Modifications of existing devices, such as adding absorbable sutures or additional appendages did not appear beneficial. Efficacy of interval insertion of IUCD was comparable with PPIUCD13. Most studies showed no differences between insertions done by hand or by instruments8, 16. The RHL review 2010, shows a total of nine trials with 7660 subjects, One trial (102 women) had compared immediate postpartum versus delayed insertion (6–8 weeks postpartum) of the levonorgestrelreleasing intrauterine system. A trial directly compared immediate versus delayed insertion reported that at 6 months the two groups were similar in terms of pregnancy prevention.21 FHI data show a significantly higher (p0.05) expulsion rate associated with insertions performed within the period of >10 minutes to 36 hours as compared to the immediate post placental period (within 10 minutes)8..we found no such relation regarding timing of insertion and expulsion rate. Complications observed were more in delayed post partum insertion than immediate post placental insertion6 . Other trials did not have uniform interventions; hence we were unable to aggregate them in this analysis. Advantages of immediate post-partum insertion include high motivation, assurance that the woman is not pregnant, and provider and client convenience6 , 1821,22,23. Lara Ricalde R et. al., observed no infection among clients. The expulsion rates were 10.4, removal rates for bleeding and pain were 4.9 and 4.8, for non medical reasons were 3.7 and 4.9 respectively for the Multiload Cu 375 and 7.7 for the CuT 380A by 10 weeks. There were no pregnancies, nor uterine perforation that is similar in this study. Xu J. et. al. observed a gross cumulative expulsion rate for the manual insertion group after 6, 12, 24, and 36 months were 8.61, 13.55, 15.78, and 16.90 %, respectively with gross expulsion rates for the ring forceps insertion group were 12.99, 17.23, 17.77, and 18.34 %, respectively. The differences between the two groups were not statistically significant12 . . In studies by Family Health International (FHI), expulsion rates varied widely between centers using similar devices. Expulsion rates ranged from 6-37/100 women at 6 months after insertion13.Sahajakittur and Kabade reported expulsion of 5.23%. No major complications and. perforation were observed in this series22. The expulsion rate in present study was very low (0.32%) in comparison with other studies, probably due to skilled training in fundal placement of IUCD. Thiersh et. al. reported that there were no pregnancies and use continuation was 77%.18 Indian experience showed that at 6 weeks postpartum, 90% of women have continued with the same IUCD. Infection rate was of 4.5% and 7% got the IUCD removed within the first 6 weeks of insertion due to bleeding and abdominal pain17.In the present study 0.76% were removed for non medical reasons, and 98.90% IUCD were retained at 14 weeks follow up.
CONCLUSION
PPIUCD is a feasible, safe and effective method of postpartum contraception among women in low resource settings, during a single visit for institutional delivery, to empower women to meet their unmet need of contraception that may be continued as a long term reversible contraception Limitation of the study In the present study 1) Sample size is small and further study with larger sample size is recommended. 2) Follow up rate is inadequate - hence there is a need to increase the follow up of clients for an analysis of data regarding safety and efficacy of PPIUCD. 3) Duration of follow up is short. Hence retention rate, safety and efficacy of IUCD as a long term reversible method of contraception could not be assessed.
IMPLICATIONS FOR RESEARCH
There is a need for long term follow up, retention rates and short- and long-term risk of pelvic infections associated with the high incidence of reproductive tract infections in low resource settings.
Recommendations
PPIUCD is a feasible method of contraception in post partum period that can be retained as a long term reversible contraception.Adequate training and supervision of delivery roomhealth providers/ staff in insertion of IUDs is Feasible. Midwives / staff nurses can be trained to insert the IUD after delivery through realistic demonstrations on Zo-E models (fig-1). Repeated PPIUCD sensitization and awareness programmes, client monitoring at Primary care centres, improvised accessibility of PPIUCD services by integrating post partum contraceptive services with Institutional maternity services, are recommended to upscale the PPIUCD services in low resource settings to prevent unintended pregnancy. This may be considered as an important evidence based intervention in averting maternal mortality in low resource settings.
ACKNOWLEDGEMENTS
We sincerely thank -The Ministry of Health and Family welfare, Government of India, and Karnataka state, and Our Mentors – JPIEGO, for training and providing technical assistance to start, implement, maintain the PPIUCD services.and in training other service providers. We thank all the women who accepted and participated in the study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles. Journals, manuals and books from where literature for this article has been reviewed and discussed. Funding The study was conducted in a government funded hospital under the provision of free maternity services. No special funding was obtained for this study.
References:
1. National Rural Health Mission Ministry of Health and Family Welfare Government of India. JSY. Available at http://www.mohfw.nic.in/layout_09- 06;.pdf.Accessed;19September;2012
2. India Reproductive health surveyNFHS, 2003,2010- Family planning Fact sheets of India
3. A global hand book for providers and PPIUCD training materials, JPIEGO.
4. The Population Council and the Program for Appropriate Technology in Health (PATH). The Copper T 380A IUCD: A Manual for Clinicians. 2nd ed. Seattle, Washington: PATH, 1989. Consensus 2011, provisional population totals; office of the Registrar General and census commissioner, India Ministry of home affairs, 31st March2011
5. Post Partum IUCD Reference Manual,November 2010:Family planning division,ministry of Health and Family welfare.
6. Grimes.D,SchulzK,VlietH,Stanwood.N;,Imme diatepost partum insertion of IUCD;TheCochranesystemicdatabase of systemic Reviews;2003;1,Art no.CD003036, DOI:1002/14651858.CD003036. PMID: 11406064 [PubMed - indexed for MEDLINE]
7. Performance standards for immediate PPIUCD counseling and services,April,20113;(NRHM,GOI);The USAID/WHO manual family planning.
8. Lara Ricalde R, Menocal Tobías G, Ramos Pérez C, Velázquez Ramírez N;-Random comparative study between intrauterine device Multiload Cu375 and TCu 380a inserted in the postpartum period,Departamento de planificación familiar del InstitutoNaciónal de Perinatología. Lomas Virreyes, México. lararoger@yahoo.com.mx pub med.
9. Morrison C, Waszak C, Katz K, Diabate F, Mate EM; Clinical out-comes of two early postpartum IUCD insertion programs in Africa. Contraception 1996;53:17-21.
10. Mohamed SA, Kamel MA, Shaaban OM, Salem HT;Acceptability for the use of postpartum intrauterine contraceptive devices: Assiutexperience.,Medprinc pract.2003,julsep;12(3):170-5
11. Celen S, Möröy P, Sucak A, Aktulay A, Dani?man N; Clinical outcomes of early postplacental insertion of intrauterine contraceptive devices.;Contraception,2004 Apr:69(4):279-82.
12. Xu J, Yang X, Gu X, Xu S, Zhou X, Chen Y, Xiao Z, Zhuang L Comparison between two techniques used in immediate postplacental insertion of TCu 380A intrauterine device: 36- month follow-up.; ReproductiveContraception.1999; 10(3):156- 62
13. Ero?lu K, Akkuzu G, Vural G, Dilbaz B, Akin A, Ta?kin L, HaberalAComparison of efficacy and complications of IUD insertion in immediate postplacental/early postpartum period with interval period: 1 year follow-up.; Cochrane Database Syst Rev. 2001;(2):CD003036. Update in: Cochrane Database Syst Rev. 2003;(1):CD003036.
14. Cole LP, Edelman DA, Potts DM, Wheeler RG, Laufe LE. Postpartum insertion of modified intrauterine devices;J Reprod Med. 1984 Sep;29(9):677-82
15. O'Hanley K, Huber DH;Postpartum IUDS: keys for success;.;Contraception. 1992 Apr;45(4):351-61.
16. Erika Levi, Evelyn Cantillo,Veronica Ades, Erika Banks, AmitasrigowriMurthy; Immediate postplacental IUD insertion at cesarean delivery: a prospective cohort study;Contraception;VVolume 86, Issue 2 , August ,Pages 102-105,
17. B.Sood et. al.,Jhpiego/India, New Delhi, IndiaR. Asif, E. Charurat, S. Das, S. Kumar, C.McKaig,,M.Rath,,S.Saha,R.Sethi,V. Srivastava,V.Yadav ;Revitalization of postpartum IUCD (PPIUCD) services: experience from India, http://dx.doi.org/10.1016/j. Contraception;Volume 86, Issue 2, August 2012, Pages 184–185,
18. Thiery M, Van Kets H, Van Der Pas H. Immediate postplacental IUD insertion: the expulsion problems. Contraception 1985;31;331-349
19. Hayes JL, Cwiak C, Goedken P, Zieman M;A pilot clinical trial of ultrasound-guided postplacental insertion of a levonorgestrel intrauterine device. Department of Gynecology and Obstetrics, Grady Memorial Hospital, Emory University, Atlanta, GA 30303, USA. jhayes@mail.magee.edu
20. Global Health Observatory; Unmet need for family planning. Geneva: World Health Organization:www.who.int/entity/gho/mdg/m aternal_health/situation_trends_family_planni ng/en.
21. Muthal-Rathore A. Immediate postpartum insertion for intrauterine devices: RHL commentary (last revised: 1 September 2010). The WHO Reproductive Health Library; Geneva: World Health Organization
22. Sahaja Kittur, Y. M. Kabadi; Enhancing contraceptive usage by post-placental intrauterine contraceptive devices (PPIUCD) insertion with evaluation of safety, efficacy, and expulsion;. Int J Reprod Contracept Obstet Gynecol. 2012; 1(1): 26-32
23. Xu JX, Reusche C, Burdan A. Immediate postplacental insertion of the intrauterine device: a review of Chinese and the world's experiences. Adv Contracept 1994; 10:71-82.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





