IJCRR - 6(14), July, 2014
Pages: 17-24
Date of Publication: 22-Jul-2014
Print Article
Download XML Download PDF
CLINICAL PROFILE OF REFERRED OTALGIA IN A TERTIARY HEALTH CENTRE - A RETROSPECTIVE STUDY
Author: Geetha K. Siddapur, Kishan R. Siddapur
Category: Healthcare
Abstract:Objectives: Assessment of age and gender distribution amongst otalgia cases, identification and categorization of referred nerve pathways, etiological factors, and analysis of significance by statistically correlating occurrence of cervical spine degenerative disease (CSDD) with respect to age and gender factors. Methods: The study conducted is retrospective, which included otalgia cases examined between April 2010 and April 2014. A total of 693 cases of otalgia were identified by ENT (Ear Nose Throat) and head and neck examination, dental and orthopedic data from the respective in and out patient departments. Radiographic records were referred wherever relevant. Patients were separated into two cohorts. Group I included Cervical Spine Degenerative Disease cases (CSDD) and Group II, Non- cervical spine degenerative disease cases. The data collected was tabulated and statistically analyzed. Results: Of total 693 otalgia cases, referred otalgia (n=169 cases) accounted for 24.4%. Females outnumbered males, accounting for 66.9% of the cases. Age group 20-40 years was affected the most (48.5%), followed by 40-60years age group (29.6%). Dental pathology outnumbered the etiological factors (30.8%), followed by cervical spine degenerative disease (CSDD) [26.6%] and Temporo Mandibular joint dysfunction (TMJD) [19.5%]. Conclusion: Middle age group involvement in Group I (cervical spine degenerative disease cases) was in contrast to most other studies, where, elderly age group was most commonly affected. Therefore, high index of suspicion should be borne in mind to diagnose referred otalgia due to cervical spine degenerative disease in younger to middle age groups, without which, many such cases could be misdiagnosed or undiagnosed.
Keywords: Retrospective, Primary, Referred otalgia, Auriculotemporal nerve, cervical spondylosis
Full Text:
INTRODUCTION
Otalgia is a complaintofall ages, which is due to complex neuroanatomic innervation of the ear, head, and neck and can be classified as otogenic (primary) or nonotogenic (referred).1, 2 External and middle ear infections are associated with primary otogenic pain, which most otolaryngologists and primary care physicians are trained to diagnose.3 Common disease processes resulting in primary otalgia include otomastoiditis, cholesteatoma, and foreign bodies lodged within the ear canal. In close to 50% of cases, however, the source of the pain does not reside within the ear. Rather, originates from sources distant from the ear, so called “referred otalgia”4 .A negative otologic examination and persistent otalgia should suggest the possibility of referred otalgia. Otalgiaoriginating from a non-otologic source, poses difficult diagnostic challenge to even the most experienced otolaryngologist. Referred pain is an unpleasant sensation localized to an area separate from the site of the causative injury or other noxious stimulation. Often, referred pain is caused by nerve compression or irritation. In this circumstance, the sensation of pain will generally be felt in the territory that the nerve serves (i.e., somatic dermatone) even though the damage originates elsewhere (i.e., visceral tissue).5 Ear is unique in that no other structure in the body of comparable size has such unique sensory nerve supply. The sensory nerve supply of the ear is through a combination of four cranial nerves (Cranial nerves V, VII, IX, and X) and two superior cervical plexus nerves (C2 and C3). Presumably, this complex innervation is anexcellent survival tool, and any pain perceived in that area causes a heightened sense of alarm. The differential diagnosis is specifically related to the sensory innervations of the ear, and therefore it is required that otolaryngologists have therelevant knowledge of the complex neuroanatomic innervation of the external and middle ear. Among all causes of referred otalgia, dental pathology, which transmits referred pain via a branch of the trigeminal nerve, is the most common source of non-otogenic pain.6 Furthermore, the cause of referred otalgia can also be referred pain from the mouth, teeth, larynx, or thyroid gland; neural, vascular, or lymphatic structures of neck; or the esophagus.[7,8] However, with the aging population, physicians must also consider cervical spine degenerative disease (CSDD) as an increasingly common cause of referred otalgia involving the upper cervical plexus (greater auricular and lesser occipital nerve). Cervical spine degenerative disease (CSDD) includes osteoarthritis, cervical facet syndrome, spondylosis, disc herniation, and stenosis. In this retrospective study; age and gender distribution amongst otalgiacases, referred nerve pathway and etiological factors wereidentified and categorized. Strength of significance by statistically correlating occurrence of cervical spine degenerative disease with respect to age and gender factors has also been analyzed.
MATERIALS AND METHODS
The study conducted is retrospective, and included otalgia cases examined between April 2010 and April 2014 in Karpaga Vinayaga Institute of Medical Sciences & Research Centre, Tamil Nadu. A total of 693 cases of otalgia were identified by ENT (Ear Nose Throat) and head & neck examination, dental and orthopedic data from the respective in and out patient departments. Radiographic records were referred wherever relevant. Primary cases (524 otogenic cases), which also included those patients who had undergone previous ear surgery, were excluded. Patients with unspecified otalgia (169 referred otalgiacases) were selected. Patients were separated into two cohorts. Group I consisted referred otalgia caseswith clinical and/or radiographic evidence of Cervical Spine Degenerative Disease (CSDD), and Group II included referred otalgia cases with other etiological factors (Non- CSDD). There were 45 cases in Group I, and 124 in Group II. A positive imaging study showing cervical spine degenerative disease at or above C4 was assumed to be positive but did not exclude its diagnosis based on clinical evidence. Age and gender were also statistically analyzed between the two cohorts. Referred nerve pathway involvement was ascertained. The distributions of all diagnosed etiologic factors for referred otalgia (169cases) with their respective nerve pathways were categorized. The data thus collected was tabulated and statistically analyzed. Chi-square test was used wherever applicable. Significance level was assessed with P value<0.05.
RESULTS
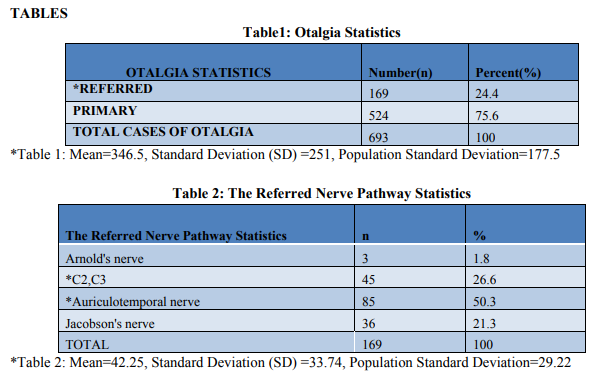
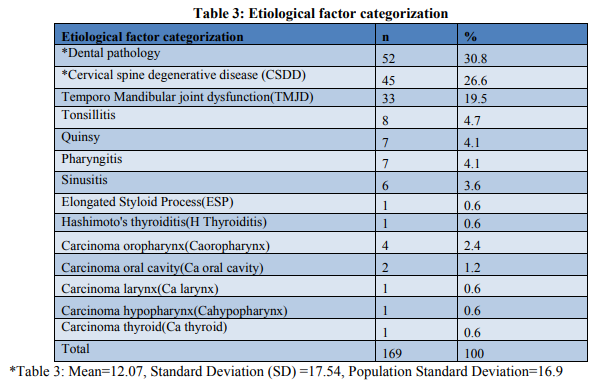
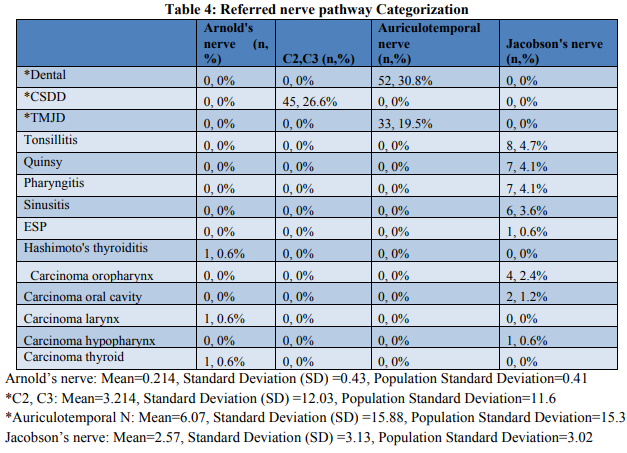
Of total 693 otalgia cases, referred otalgia (n=169 cases) accounted for 24.4% (Table1). Females outnumbered males, accounting for 66.9% of the cases. Age group 20-40 years was affected the most (48.5%), followed by 40-60 years age group (29.6%) and more than 60 years age group (8.3%). Auriculotemporal nervepathway was involved in majority of the cases (50.3%), followed by Greater auricular and lesser occipital nerve pathway (26.6%) [Table2]. Dental pathology outnumbered the etiological factors (30.8%), followed by cervical spine degenerative disease (CSDD) [26.6%] and Temporo Mandibular joint dysfunction (TMJD) [19.5%] as shown in Table3. Auriculotemporal nervepathway was found responsible for dental pathology and Temporo Mandibular joint dysfunction, and C2, C3 pathway for CSDD (Table 4). Two cohorts were categorized in this study, Group I (CSDD) and Group II (non-CSDD). The groups were correlated with the age and gender factors and tested for significance with P Value < 0.05 using Chi-Square test (Table5, table6, Figure1 & Figure2). The result was assessed as either significant, or not-significant. Chi Square test was applied to the Two Groups and the Two Genders (Table5). The Chi-square statistic was 6.5294. The P value was 0.010611. This result was highly significant at p < 0.05. Chi Square test was also applied to the Two Groups and the two age groups (Table6). The Chi-square statistic was 17.6726. The P value was 2.6E-05. This result was significant at p < 0.05. Thus, both the statistical correlation tests were significant.
DISCUSSION
Despite awareness regarding potential causes of referred otalgia, diagnosis often eludes the most experienced physician. The incidence of referred otalgiain our study was 24.4% of total otalgia cases. We documented many causes of referred otalgia representing all five nerve pathways, with women accounting 67% of the referred otalgia cases; similar to most other studies like Chen et. al. 9 and Vedasalam et. al. 10 . Higher incidence in females, in our study, could be due their hectic life style. Most females in the local population around the hospital are hard core workers, working as laborers and construction workers. Maybe cervical spine of females isn’t meant to handle this kind of stress. In most studies, elderly age groups have had an increased incidence of cervical spine degenerative disease, but in our study, less than 50 years age groupwas also equally affected. Yet again, this may be because of the life style of the local population, amongst whom; many are laborers (construction workers) and farmers. Most of these people belong to less than 50 years age group. These people tend to get severe stress in neck region while lifting heavy goods, loads, and thus are more prone for Cervical Spine Degenerative Diseases. Nerve pathways most commonly involved were Auriculotemporal nerve (50.3%) and Greater auricular lesser occipital nerve (C2C3) [26.6%]. Due to length and extensive distribution of the trigeminal nerve, it is not surprising that this nerve is most commonly involved in referred otalgia. 11The mechanism of how cervical spine disease is referred to the ear is controversial. One possible mechanism is via an interconnection between the cervical afferents with the spinal tract of the trigeminal nerve, which is thought to descend as far down as C4. Sensory information from the upper cervical roots is subsequently relayed to the trigeminal dermatomes (namely Cranial nerve V3), which in turn can be referred to the ear.12 This type of non-otogenic ear pain, especially involving disorders of the tempomandibular joint, is well documented by Seedorf et. al. 13 and James et. al. 14 . Dental caries has the capacity to produce constant boring ear pain, whereas laryngeal cancer may result in a much less intense earache.Within the subset of processes affecting V3, dental diseases account for most pathology causing referred otalgia15. This was parallel to our study which indicated that dental problems form the major cause (30.8%) in both genders followed by cervical spine lesions (26.6%) then TMJ dysfunction (19.5%). In our study, cervical spondylosis was the only cervical spine lesion detected.
Two cohorts were categorized in this study, Group I (CSDD) and Group II (non-CSDD). The most common etiology in Group II was Dental pathology. Surprisingly, one group of patients with non-otogenicotalgia are those diagnosed with cervical spine disorders, in particular cervical spine degenerative disease.16 Referred otalgia due to cervical spine disease usually is described as retroauricular or infra-auricular pain, which is constant and often related to changes in neck position. In this current study we have shown that cervical spine degenerative diseases, diagnosed either through radiographic or clinical evidence, is an important contributor to referred otalgia. Cervical spine degenerative disease referred otalgia represented 26.6% of referred otalgia cases. Kuttila et. al. also reported that women presented with otalgia more often than men17. The two groups were correlated with the age and gender factors and tested for significance with P Value < 0.05 using Chi-Square test. The result was significant, which meant, age and gender factors were significant in the occurrence of cervical spine degenerative disease, leading to rejection of null hypothesis. Referred otalgia has been a well-documented phenomenon in the ear, nose, and throat (ENT) and neurosurgical literature. An understanding of the various sensorineural pathways that dually innervate the ear and other sites and ongoing dialogue with our clinical colleagues will ensure that patients with referred otalgia will receive the best care. Cervical spine degenerative diseasereferred otalgia is propagated through disease of the cervical vertebrae and therefore is postural. This ear pain can be ameliorated with physical therapy, and most studies support conservative treatment, such as cervicothoracic stabilization programs, combined with aerobic conditioning in treating cervical spine disorders.18 Keeping this in mind, we recommended outpatient physical therapy to all our patients with cervical spine degenerative disease referred otalgia. Though dental pathology was the major etiological factor for referred otalgia in our study, we preferred to analyze the occurance of cervical spine degenerative disease, because, the early age group involvement in Group Iwas in contrast to most other studies, where, elderly age group was most commonly affected.
CONCLUSION
We, the authors of this study, conclude by quoting that high index of suspicion should be borne in mind to diagnose referred otalgia due to cervical spine degenerative disease in younger to middle age groups, without which, many such cases could be misdiagnosed or undiagnosed. It now seems that occupational and life style factors have an equally important role to play in comparison to aging factor, in determining the occurrence of cervical spine degenerative disease. Therefore, more research needs to be done in analyzing the significance of these factors.
ACKNOWLEDGEMENTS
We thank Dr. T. Rathinam, Professor & head, for sharing his valuable advice whenever required. We also thank Dr. B. Sundararajan, Professor, for his moral support during the study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Shah RK, Blevins NH. Otalgia. OtolaryngolClin North Am 2003;36:1137–51.
2. Thaller SR. Otalgia with a normal ear. Am Fam Physician 1987;36:129–36.
3. SiddiqM, Samra M. Otalgia. BMJ 2008;336:276-77.
4. Jaber J, Leonetti P, Lawrason A and Feustel P. Cervical spine causes for referred otalgia.Otolaryngol Head Neck Surg 2008;138:479- 85.
5. Powers WH, Britton BH. Nonotogenicotalgia: diagnosis and treatment. Am J Otol 1980;2:97–104.
6. Kreisberg MK, Turner J. Dental causes of referred otalgia. Ear Nose Throat J 1987 Oct;66:398–408.
7. Scarbrough TJ, Day TA, Williams TE, et. al. Referred otalgia in head and neck cancer: a unifying schema. Am J ClinOncol 2003;26:e157– 62.
8. Yanagisawa K, Kveton JF. Referred otalgia. Am J Otolaryngol 1992;13:323–7.
9. Chen R,khorsandi S,Shatzkes D, Holliday R.The radiology of referred otalgia.American Society of Neuroradiology 2009.
10. Vedasalam S, Sipaul F, Porter G. Internal laryngocoele and referred otalgia. BMJ Case Reports2010;10.
11. Tuz H, Onder EM, Kisnisci RS. Prevalence of otologic complaints in patients with temporomandibular disorder. Am J OrthodDentof Orthopedic 2003;123:620-23.
12. van der Meulen M, Ohrbach R, Aartman I, Naeije M, Lobbezoo F. "Temporomandibular disorder patients' illness beliefs and selfefficacy related to bruxism". J Orofac Pain 2010;24:367–72.
13. Seedorf H, Jude H.Otalgia in patients with temporomandibular joint disorders. NCPI Laryngorhinootologie 2006;85:327-32.
14. James J, John P, Amy E, Paul J. Cervicalspinecauses for referredotalgia. Otolaryngology - Head and Neck Surgery 2008;138:479–85.
15. Kim D, Cheang P, Dover S, et. al. Dental otalgia. J LaryngolOtol 2007;121:1129– 34.
16. Danish SF, Zager EL. Cervical spine meningioma presenting as otalgia: case report. Neurosurgery 2005;56(3):E621
17. Kuttila SJ, Kuttila MH, Niemi PM, et. al. Arch.Otolaryngol Head Neck Surg 2001;127:401–5.
18. Saal JS, Saal JA, Yurth EF. Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877–83.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





