IJCRR - 6(19), October, 2014
Pages: 66-68
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
HISTOID HANSENS DISEASE - A RARE CASE REPORT
Author: Vimal Chander R., Jayaganesh P., Ganthimathy Sekhar, Chitra S.
Category: Healthcare
Abstract:Introduction: Histoid Hansens disease is a very rare variant of lepromatous leprosy with nodules and plaques over normal appearing skin with characteristic histopathological and bacterial morphology and clinically simulating dermatofibromas, xanthomas, neurofibromas or reticulohistiocytosis. Case report: We report a case of histoid Hansens disease in a 34 year old male presenting with multiple papulovesicular nodules in the skin of lower back, arms, elbow and abdomen which on microscopy showed features of Histoid Hansens disease witha bacillary index of 6+. Conclusion: A high index of suspicion is necessary especially when patients present with unusual skin lesions and estimation of bacterial index is highly indicated as was proven in our case.
Keywords: Hansens disease, Histoid leprosy, Histoid, Lepromatous
Full Text:
INTRODUCTION
Histoid Hansens disease is a very rare variant of lepromatous leprosy characterized by cutaneous and/or subcutaneous nodules and plaques present over normal appearing skin, with characteristic histopathological and bacterial morphology. The term ‘histoid leprosy’ was originally coined by Wade as a histological concept of acid fast bacilli-rich leproma composed of numerous spindle shaped cells with the absence of globus formation (which is so conspicuous in classical lepromatous leprosy). It exhibits fibromatoid features in the chronic form. Since then, there have been many reports, with variable findings. We report a case of histoid leprosy in a 34 year old male, presenting with multiple papulovesicular nodules in the skin in view of the rarity of the condition.
CASE REPORT
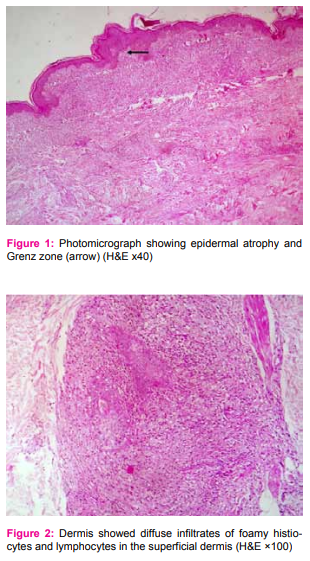
A 34 year old male, complained of multiple nodules all over the body since one year. The nodules were seen on his lower back, arms, elbows, and abdomen. On clinical IJCRR Section: Healthcare examination, there were multiple papulovesicular nodules, nontender, firm to soft in consistency, measuring 0.5 cm to 1.5 cm in diameter. Papules were also present over the extensor surface of the arm, abdomen and lower back. There was no impairment of touch, pain or thermal sensation. There was no nerve thickening or any lymph node enlargement. A clinical diagnosis of molluscum contagiosum was made. Punch biopsy of a nodule over the elbow was taken and sent for histopathological examination. The specimen received was a linear piece of skin with underlying soft tissue measuring 1.5x0.5x0.5cm. It was bisected and both the pieces were embedded. Microscopic examination showed skin with atrophic epidermis with a subepidermal Grenz zone. [Figure 1] The dermis showed diffuse infiltrates of foamy histiocytes and lymphocytes in the superficial dermis as well as mixture of spindle cells and foamy histiocytes surrounding the dermal appendages and nerves. [Figures 2, 3 and 4] The Fite-Faraco stain showed plenty of uniformly stained acid fast bacilli arranged singly and in globi with a bacterial index of 6+. [Figure 5]
An impression of Histoid leprosy was then given. The patient was put on multibacillary multidrug therapy and is on regular follow-up. DISCUSSION Histoid leprosy is an uncommon variant of lepromatous leprosy and its incidence among leprosy patients in India is estimated to be 2.79 to 3.60%. There is a male preponderance with average age at diagnosis between 21 and 40 years. The incidence of histoid leprosy was found to be 8.7% among lepromatous leprosy cases. Clinically, histoid leprosy is characterized by cutaneous and/or subcutaneous nodules or papules, which are usually painless, discrete, firm, smooth, globular and skin colored to yellowish brown, with normal appearing skin surrounding it. The lesions are usually found in the posterior and lateral aspects of the arms, thighs, buttocks, lower part of the back, dorsum of the hands, and over the bony prominences, especially over elbows and knees. Ears may be unaffected. Histoid lesions have also been reported to be present along the course of the peripheral nerve trunks and cutaneous nerves. The histoid leproma has also been reported to occur during the early stages of lepromatous leprosy or borderline lepromatous leprosy. In such cases, the lesion is transient and disappear as the lepromatous leprosy progresses Histoid leprosy clinically simulates dermatofibromas, xanthomas, reticulohistiocytosis, neurofibroma or cutaneous metastasis. They can be differentiated from histoid leprosy on the basis of their characteristic histopathology, the absence of the acid fast lepra bacilli on slit skin smear and absence of nerve thickening. There are three histological variants of histoid leprosy, namely the pure fusocellular, fusocellular with epithelioid component and fusocellular with vacuolated cells. The last pattern is most commonly observed. Slit skin smear from the lesions in histoid leprosy show abundant acid fast bacilli in singles, clusters, or tightly packed in macrophages (globi). These bacilli tend to be longer with tapering ends when compared to the ordinary lepra bacilli. The bacillary index may be 5+ to 6+ and the morphological index may also be very high. The high bacillary index in histoid leprosy is suggested to be due to focal loss of immunity. Classical histopathological findings include epidermal atrophy as a result of dermal expansion of the underlying leproma and a grenz zone located immediately below the epidermis. The macrophage reaction is unusual in that the cells frequently become spindle shaped or fusiform and oriented in a storiform or a whorled pattern, similar to those of a fibrohistiocytoma or a dermatofibroma. These histiocytes usually resemble fibroblasts and it has been suggested that fibroblast-like macrophages may have arisen from the tissue histiocytes rather than blood monocytes. Within these histiocytes, an abundance of acid-fast bacilli can be seen. The Histoid leprosy patients are usually treated with the World Health Organisation multibacillary multidrug therapy for one year. Among 17 cases of leprosy reported in our institution over the past 5 years, there were 5 cases of borderline tuberculoid, 1 mid borderline, 3 borderline lepromatous, 3 lepromatous, 4 indeterminate leprosy and this was the first case of histoid leprosy diagnosed in our institution.
CONCLUSION
Histoid leprosy is a distinctive type of lepromatous leprosy, clinically and histopathologically simulating a dermatofibroma. Due to endemicity of leprosy in our country, there should be a high index of suspicion of this disease for all unusual skin lesions and estimation of bacterial index is highly indicated as was proven in our case. Though many studies indicate that leprosy is not prevalent as before, time and again it has been proven that we require a high index of suspicion especially when patients present with unusual skin lesions. Hence it is essential to continue the surveillance for new and relapsed cases, rather than waiting for voluntary reporting to treat and eliminate leprosy.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Murthy SV, Rao SM, Thejaswini, and Mannan K. De-novo Histoid Leprosy. J Lab Physicians 2011;3:110–2.
2. Kaur I, Dogra S, De D, Saikia UN. Histoid leprosy: a retrospective study of 40 cases from India. Br J Dermatol 2009;160:305-10.
3. Nair SP, Kumar GN. A clinical and histopathological study of histoid leprosy. Int J Dermatol 2013;52:580-6.
4. Nair SP, Moorthy KP, Suprakasan S, Jayapalan S, Mini G. Histoid leprosy - unusual presentation. Int J Dermatol 2006;45:433-4.
5. Kamath H D, Sukumar D, Shetty NJ, NandaKishore B. Giant lesions in histoid leprosy - an unusual presentation. Indian J Lepr 2004;76:355-8.
6. Bakry OA, Attia AM. Histoid leprosy: case report. Acta Dermatovenerol Croat 2012;20:256-9.
7. Annigeri SR, Metgud SC, Patil JR. Lepromatous leprosy of histoid type. Ind J Med Microbiol 2007;25:70-1.


|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





