IJCRR - 6(19), October, 2014
Pages: 61-65
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
A RARE CASE OF GLOMANGIOPERICYTOMA OF THE NASAL CAVITY
Author: S. Vijayasundaram, P. Karthikeyan, V. Nirmal Coumare, Satvinder Singh Bakshi, Davis Thomas Pulimoottil
Category: Healthcare
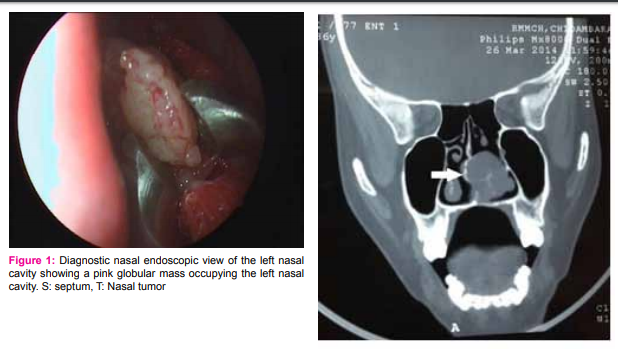
Abstract:Aim: Here we present a rare case of Glomangiopericytoma of the nasal cavity and review the recent literature. This case is presented because of its rarity. Case report: A 36-year-old woman presented to the Outpatient Department of ENT and Head and Neck Surgery in a tertiary care centre with complaints of progressive unilateral nasal obstruction and anosmia over a 6 month period. Anterior rhinoscopicex amination revealed a pinkish globular mass occupying the left nasal cavity. Computed tomography (CT) scan revealed an ill defined homogenous soft tissue density lesion involving the left nasal cavity, infiltrating the nasal septum posteriorly and extending upto the choana with a deviated nasal septum to the right side. The tumor was resected completely by endoscopic approach. Histopathologic examination with immunohistochemistry of the resected mass confirmed the diagnosis of glomangiopericytoma. Discussion: Glomangiopericytoma is a rare sinonasal neoplasm characterized by a perivascular myoid phenotype and is considered
as distinct from conventional soft tissue hemangiopericytoma. It accounts for less than 0.5% of all sinonasal tumors. It
is classified as a borderline low malignancy tumor.Conclusion: This tumour is associated with a very good prognosis following surgery and complete surgical resection with negative margins preferably via a transnasal endoscopic approach is the treatment of choice.
Keywords: Nasal mass, Glomangiopericytoma, Endonasal endoscopic resection
Full Text:
INTRODUCTION
Glomangiopericytoma belongs to a spectrum of lesions which include myofibromatosis, myofibroma, infantile haemangiopericytoma and myopericytoma.1 According to the World Health Organization 2005 Classification of Head and Neck tumors, Glomangiopericytoma is a recently proposed term describing the sinonasal tumors demonstrating a perivascular myoid differentiation.2 Glomangiopericytoma was initially reported as hemangiopericytoma,3 but this definition has been questioned.4 Otherwise known as sinonasal type hemangiopericytoma, glomangiopericytoma is a rare tumor of borderline low malignant potential, differing from conventional soft tissue hemangiopericytoma in terms of location and clinical and histopathological features.2 Glomangiopericytoma characteristically has a component of cells with glomus-type features including cuboidal cells, distinct IJCRR Section: Healthcare cell borders, clear to eosinophilic cytoplasm and central round nuclei. The etiology may involve past trauma, hypertension, pregnancy and use of corticosteroids.5
CASE REPORT:
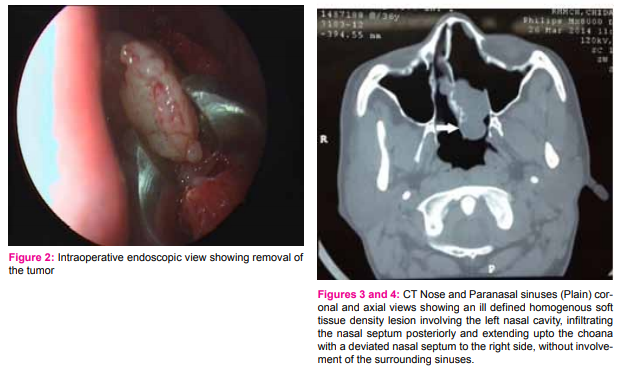
A 36 year old female presented to the outpatient Department of ENT and Head and Neck Surgery of a tertiary care centre with 6-month history of progressive left nasal airway obstruction and ipsilateral anosmia. The patient gave a history of one episode of left sided epistaxis . The patient had a history of previous nasal surgery 10 years prior, but no records were available. Anterior rhinoscopy revealed a pinkish globular mass occupying the left nasal cavity, sensitive to touch with minimal bleeding on probing and appeared to be sessile, arising from the nasal septum. The mass appeared to have pushed the septum to the opposite side. There was no enlargement of cervical lymph nodes. Diagnostic nasal endoscopy revealed a pink globular mass occupying the left nasal cavity and extending posteriorly up to the choana. The mass appeared to be attached to the septum, pushing it to the opposite side. Computed tomography (CT) scan showed an ill defined homogenous soft tissue density lesion involving the left nasal cavity, infiltrating the nasal septum posteriorly and extending upto the choana with a deviated nasal septum to the right side, without involvement of the surrounding sinuses. Biopsy from the mass was not realized due to the risk of bleeding. An endoscopic endonasal resection of the mass was performed, during which the tumour was found to arise from the nasal septum, and following complete excision, a defect was found in the posterior bony septum. Hemostasis was attained with the use of bipolar cautery and compression with pledgets soaked in diluted adrenaline. Histopathological examination of the specimen revealed tissue fragments lined by respiratory epithelium and underlying subepithelium consisting of well delineated diffuse growth of tumor cells arranged in the form of interlacing short fascicles and whorls. The tumor cells were round to elongated with vesicular to hyperchromatic nuclei and scanty eosinophilic cytoplasm. Dilated ectatic blood vessels with hyalinization were also seen. Necrosis and cytological atypia were absent. Immunohistochemically, the tumor was positive for vimentin and smooth muscle actin, and negative to CD34, S-100 protein and cytokeratin. These histopathologic findings were consistent with a diagnosis of glomangiopericytoma. Postoperatively, the patient was followed up regularly every two months. At 12 months follow up the patient does not have recurrence.
DISCUSSION
Glomangiopericytoma is defined as a sinonasal tumor showing perivascular myoid phenotype.6 Initially reported as hemangiopericytoma in 1942,3 this tumor arising from the sinonasal tract was later described by Compagno in 1976 as ‘‘hemangiopericytoma-like’’ because of the lower rates of metastasis and mortality.7 Most tumors formerly designated as soft tissue hemangiopericytomas are fibroblast-derived and represent the cellular variant of solitary fibrous tumors. As true hemangiopericytomas are related to glomus tumors, the designation ‘‘myopericytoma’’ or ‘‘glomangiopericytoma’’ is preferred by the WHO as the diagnostic category for these soft tissue tumors.6 Clinically and histologically, sinonasal hemangiopericytomas differ from hemangiopericytoma developing elsewhere in the body and thus is considered a distinct entity.4 The pathogenesis of glomangiopericytoma is unclear and previous trauma, hypertension and prolonged steroid use have been speculated to be possible causes.5 Our patient gave a history of previous nasal surgery ten years prior to presentation. Glomangiopericytoma represents less than 0.5% of all sinonasal neoplasms and develops in the nasal cavity and/or paranasal sinuses6 with a slight female preponderance and the peak age of incidence in the seventh decade.8 The most common mode of presentation is unilateral nasal obstruction with or without recurrent epistaxis. Less common complaints include difficulty in breathing, visual disturbance and headache.9 Gross examination of the tumor usually reveals a polypoid mass, beefy red to grayish pink in colour, soft or fleshy or friable in consistency and oedematous or hemorrhagic in appearance, and which bleeds on touch. Rarely there may be regional lymph node involvement.10 Computed tomography (CT) scan demonstrates a non calcified soft-tissue mass in a nasal fossa or a paranasal sinus and may be associated with sinusitis, displacement of adjacent structures and bone erosion. Contrast enhanced imaging demonstrates the vascular nature of the tumor.10 The diagnosis of a glomangiopericytoma is based on histopathology. Microscopically, glomangiopericytomas are submucosal polypoid tumors rimmed by a border of superficially spared stroma and respiratory epithelium with pushing and/or locally infiltrative borders. These tumors are composed of short, bland spindle cells forming fascicular, storiform, or whorled patterns. Tumor nuclei are uniform and evenly spaced and tumor cells have a moderate amount of eosinophilic cytoplasm with indistinct cell membranes imparting a syncytial appearance. A characteristic feature is perivascular hyalinization and tumor cells may be seen oriented perpendicular to these hyalinized vessel walls. Generally, there is a low mitotic rate and nuclear pleomorphism is absent or minimal.4 Malignant glomangiopericytoma is uncommon and usually presents with large size, bone invasion, profound nuclear pleomorphism, increased mitotic activity and necrosis.11 Immunohistochemically, glomangiopericytomas characteristically express vimentin, smooth muscle actin (SMA), muscle specific actin (MSA), and factor XIIIa and there is usually no expression of desmin, CD34, bcl-2, factor VIII or S100 protein. D2-40 stains vascular channels within all glomangiopericytomas to a variable degree which is in contrast to conventional soft tissue hemangiopericytoma/solitary fibrous tumors which reveal no intratumoral D2-40 vascular staining.12
Glomangiopericytomas are considered to be low malignant tumors with a low propensity to metastasize, a recurrence rate of 7% to 40%, and a 5-year survival of 88% or higher. Treatment for glomangiopericytomas is local excision with negative margins. Excellent overall survival was achieved with complete surgical excision and recurrence is often due to incomplete tumor resection. Metastatic disease and disease-related mortality is extremely rare (3%). Thus, a regular follow-up postoperatively is essential.1,12,13,14
CONCLUSION
Glomangiopericytoma is a rare sinonasal tumor demonstrating a perivascular myoid phenotype. It differs from usual soft-tissue hemangiopericytoma in location, biologic behavior and histopathologic characteristics and is categorized as a borderline low malignancy tumor. Complete surgical resection with negative margins is the treatment of choice. Regular post-operative follow- up is essential in view of the risk of local recurrence.
ACKNOWLEDGEMENT
The authors would like to thanks to Prof. Dhananjay S. Kotasthane, Professor and Head, Department of Pathology, MGMCRI, Pondicherry. The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors and editors of all those articles and journals from where the literature for this article has been reviewed and discussed.
References:
1. Sun Q, Zhang C, Chen W, He Y. The molecular mechanisms on glomangiopericytoma invasion. Orphanet J Rare Dis. 2013 Sep 29;8:152.
2. Chihani M, Aljalil A, Touati M, Zoubeir Y, Labraimi A, Ammar H, Bouaity B. Glomangiopericytoma: an uncommon sinonasal perivascular tumor with particular characteristics. EJENTAS (2011);12:167-170.
3. Stout AP, Murray MR: Hemangiopericytoma: a vascular tumor featuring Zimmermann’s pericytes. Ann Surg 1942, 116:26–33.
4. Thompson LD, Miettinen M, Wenig BM. Sinonasal-type hemangiopericytoma: a clinicopathologic and immunophenotypic analysis of 104 cases showing perivascular myoid differentiation. Am J Surg Pathol. 2003;27:737–749.
5. Angouridakis N, Zaraboukas T, Vital J, Vital V: Sinonasal hemangiopericytoma of the middle turbinate: a case report and brief review of the literature. B-ENT 2007, 3:139–143.
6. Thompson LDR, Fanburg-Smith JC, Wenig BM. Borderline and low malignant potential tumours of soft tissues. In: Barnes L, Eveson JW, Reichart P, Sidransky D, eds. World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005:43–45.
7. Compagno J, Hyams VJ. Hemangiopericytoma-like intranasal tumors: a clinicopathologic study of 23 cases. Am J Clin Pathol. 1976;66:672–683.
8. Lester D, Thompson M. Sinonasal tract glomangiopericytoma (hemangiopericytoma). Ear Nose Throat J. 2004;83:807. 9. Watanabe K, Saito A, Suzuki M, Yamanobe S, Suzuki T. True hemangiopericytoma of the nasal cavity. Arch Pathol Lab Med. 2001;125:686–690.
10. Gillman G, Pavlovich JB. Sinonasal hemangiopericytoma. Otolaryngol Head Neck Surg. 2004;131:1012–1013
11. Kowalski PJ, Paulino AF. Proliferation index as a prognostic marker in hemangiopericytoma of the head and neck. Head Neck. 2001;23:492–496.
12. Catalano PJ, Brandwein M, Shah DK, Urken ML, Lawson W, Biller HF. Sinonasal hemangiopericytomas: a clinicopathologic and immunohistochemical study of seven cases. Head Neck. 1996;18:42–53.
13. Billings KR, Fu YS, Calcaterra TC, Sercarz JA. Hemangiopericytoma of the head and neck. Am J Otolaryngol. 2000;21:238–243.
14. Castelnuovo P, Pagella F, Delu` G. Endoscopic resection of nasal haemangiopericytoma. Eur Arch Otorhinolaryngol. 2003;260: 244–247.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





