IJCRR - 6(19), October, 2014
Pages: 59-60
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
CONGENITAL DIAPHRAGMATIC HERNIA IN POST NEONATAL PERIOD
Author: Nitin Pandey, Krishna Kumar Yadav
Category: Healthcare
Abstract:Background: Late presentation of right sided congenital diaphragmatic hernia can present with recurrent cough in postneonatal period. Case characteristics: A 1 - year male child presented to outpatient with complain of recurrent cough since birth. Observation: Child was malnourished and had respiratory distress. There was no cyanosis and pallor was present. Auscultatory finding show decreased breath sound to right side and normal heart sounds. Outcome: Late presentation of right sided congenital diaphragmatic hernia. Message: CDH though, rare condition in postneonatal period could be encountered in outpatient practice with children presenting with recurrent cough and growth failure.
Keywords: Congenital diaphragmatic hernia, Post- neonatal period
Full Text:
INTRODUCTION
Congenital diaphragmatic hernia is usually suspected during neonatal period, when newborn presents with respiratory distress. Very few case reports are available in literature for its late presentation in childhood. In developing countries with limited healthcare resources, this condition could be kept in differential diagnosis in post neonatal period.
CASE REPORT
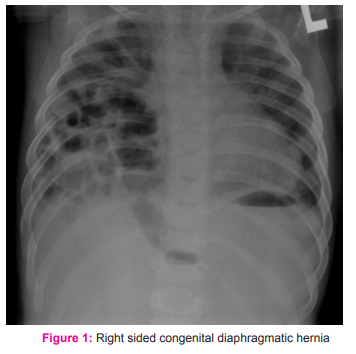
We present a case of 1 year male child presenting with recurrent cough and fever since birth. For which he had received trials of all common antibiotics and cough relieving medicine by many doctors on outpatient basis with no relief from the basic problem permanently. On examination child was in respiratory distress (Respiratory rate- 62/ min with diaphragmatic and intercostal retractions), weight 6 Kg, length 67 cm (Malnutrition according to WHO standards). Pallor was present, cyanosis absent, icterus was absent, clubbing absent and lymphadenopathy was insignificant. Temperature was 99.4 IJCRR Section: Healthcare degree F, heart reate 112/min, Blood pressure 80/54 mmHg. On auscultation there was diminished breath sound on right chest field. Cardiovascular, neurological and per abdomen examination was within normal limit. There was no suggestive history of contacts with tuberculosis. We ordered complete blood count, chest X-Ray and Mantoux test for the patient. Complete blood count was within normal limit but surprisingly in chest X- Ray we got right sided intestinal loops shadow like bag of worms and now our diagnosis was late presentation of congenital diaphragmatic hernia. Mantoux test came to be negative. After stabilizing patient condition and ruling out pulmonary hypertension in 2-D echo, we referred the patient to tertiary care center for surgical management.
DISCUSSION
Congenital diaphragmatic hernia presents with respiratory distress in neonatal period with few differential diagnosis (Anderson KD). With advances in neonatal care and resuscitation programme, congenital diaphragmatic hernia is easily diagnosed in neonatal period and managed surgically (Buttler M ). There are also sporadic case reports showing delayed presentation of CDH (craigie rj,
vandy fc, ng cp). Literature also suggests that children with right sides CDH presents with chronic symptoms in 57.4% cases, while left sided CDH mostly presents with acute symptoms, which is also the common anatomical type of CDH ( Macei Bg). In our case CDH was right sided, which is still rare in rare late presentation of CDH. Our patient’s main complain was off and on cough, which support previous finding suggesting that symptoms of respiratory system predominate the right sided CDH, while left sided CDH mainly presents with gastrointestinal symptoms (Kitano Y). Diagnosis of CDH mainly depends on clinical suspicion and chest X-Ray, although the size of herniation and amount of gastrointestinal tract herniated may cause confusion in interpretation of chest X-Ray and may confuse the picture showing differential diagnosis of pneumonia, tumor, pneumothorax and diaphragmatic eventration (Lee HM). So a quality chest x-Ray done for some other cause may diagnose a rare condition like CDH.
CONCLUSION
Congenital diaphragmatic hernia usually presents with respiratory distress in neonatal period and differential diagnosis should be considered in neonates with respiratory distress. But this condition can be missed in some neonate where respiratory distress is not so severe or proper neonatal care facility is not available. We conclude that CDH though, rare condition in postneonatal period could be encountered in outpatient practice with children presenting with recurrent cough and failure to thrive.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Anderson KD. Congenital diaphragmatic hernia. In: WelchK.J., Randolph JG, Ravitch MM, et al (eds.). Paediatric Surgery. Chicago, Year Book Medical 1986; 589-601.
2. Bag?aj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int. 2004 Sep;20(9):658-69.
3. Butler M, Stolar C, Altman P (1993) Contemporary management of congenital diaphragmatic hernia. World J Surg 17:350–355.
4. Craigie RJ, Mullassery D, Kenny SE. Laparoscopic repair of late presenting congenital diaphragmatic hernia. Hernia. 2007 Feb;11(1):79-82.
5. Kitano Y, Lally KP, Lally PA: Congenital Diaphragmatic Hernia study group: Late-presenting congenital diaphragmatic hernia. J Pediatr Surg 2005, 40(12):1839–1843.
6. Lee HM, Addavide KE, Prince NJ: Late presentation of a diaphragmatic hernia. Arch Dis Child 2011, 96(9):837.
7. Ng CP, Lo CB, Chung CH. Congenital diaphragmatic hernia masquerading as pneumonia. Emerg Med Australas. 2004 Apr;16(2):167-9.
8. Vandy FC, Landrum JE, Gerig NR, Prahlow JA. Death due to late-presenting congenital diaphragmatic hernia in a 2-year-old child. Am J Forensic Med Pathol. 2008 Mar;29(1):75-9.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





