IJCRR - 6(19), October, 2014
Pages: 54-58
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
ESTIMATION OF SERUM LIPOPROTEIN (A), LIPID PROFILE AND HBA1C IN PATIENTS WITH TYPE 2 DIABETES MELLITUS - A CASE CONTROL STUDY
Author: Sunita Pujar, Kavitha Hiremath, L.L. Pujar, Shankar Prasad, Mahanthesh Bhuthal
Category: Healthcare
Abstract:Objective: Diabetes is a major worldwide health problem, leading to markedly increased mortality and serious morbidity. It is characterised by chronic hyperglycemia resulting from a diversity of aetiologies and environmental and genetic factors acting together. Type 2 diabetes mellitus itself leads to dyslipidemia like elevated triglyceride levels and low HDL levels, which are known risk factors for coronary artery disease (CAD). Increased lipoprotein (a)[Lp(a)] concentrations are predictive of CAD. The study was designed to estimate serum lipoprotein (a) and glycosylated hemoglobin (HbA1c) in south Indian patients with type 2 diabetes mellitus and compare them with healthy controls. Material and Methods: The study included 50 patients of type 2 diabete mellitus and 50 age and sex matched controls. Fasting venous blood sample was analysed for fasting blood glucose(FBS), glycated hemoglobin (HbA1c), lipid profile and serum Lp(a). Statistical analysis was done using student t test. Results: The serum Lp(a) and HbA1c levels were significantly elevated in type 2 diabetics compared to healthy controls (p< 0.001). There was significant elevation in the levels of FBG ,total cholesterol, total triglyceride, LDL cholesterol and TC/HDLcholesterol ratio in type2 diabetics compared to the control group(p< 0.05). Conclusion: Diabetic patients have higher levels of serum Lp(a) and HbA1c compared to healthy controls. Serum Lp(a) associated with lipid abnormalities - high total cholesterol, high triglyceride ,high LDL and low HDL makes diabetics prone for CAD.
Keywords: Type 2 diabetes mellitus, Glycated hemoglobin, Lipid profile, Lipoprotein a
Full Text:
INTRODUCTION
Diabetes mellitus (DM) is world-wide in distribution. Diabetes mellitus is a chronic metabolic disorder that is often associated with unacceptably high disease burden especially in developing countries and the cardiovascular complications of DM are highly contributory to this scenario1 . In India, diabetes is not an epidemic anymore but has turned into a pandemic, according to the International Journal of Diabetes in developing countries which labelled India the diabetes capital of the world. Mainly because India now has the highest number of diabetes patients in the world. The International Diabetes Federation estimates that the number of diabetic patients in InIJCRR Section: Healthcare dia more than doubled from 19 million in 1995 to 40.90 million in 2007. It is projected to increase to 69.9 million by 2025.Currently upto 11 percent of India’s urban population and 3 percent of rural population above the age of 15 has diabetes. The most prevalent is type 2 diabetes2 . Well studied and documented CVS risk factors in DM include components of metabolic syndrome namely dyslipidemia, central obesity and hypertension3 . Other CVS risk factors that have not been widely studied in Indian population include C-reactive protein, hyeruricemia, HbA1c and lipoprotein (a). Lipoprotein (a) [Lp(a)] consists of an LDL like particle and the specific apolipoprotein (a) [apo(a)],which is covalently bound to the apo B of the LDL like particle. The structure of Lp(a)
resembles LDL and its atherogenic properties can be explained by its binding to glycosaminoglycans and inhibition of fibrinolysis. The atherogenic properties of Lp(a) are expressed over 30 mg/dl4 . Persistent hyperglycaemia causes glycosylation of the proteins especially hemoglobin5 . Haemoglobin glycation, estimated by percentage of glycated haemoglobin (HbA1c) ,was first used clinically 30 years ago to asses the degree of chronic hyperglycaemia among diabetic patients in whom values reflect weighted mean glucose levels over the preceding 3 months period; it is useful for characterizing dysglycemia in population studies because it is simpler to perform than the oral glucose tolerance test(GTT) 6 . In Diabetics an increase in HbA1c of 1 percent was associated with a 20 % to 30% increase in mortality associated with cardiovascular events7 .
MATERIALS AND METHODS
Study Participants: The present study comprises 50 patients with Non-Insulin dependent diabetes mellitus (NIDDM) reporting to Hanagal Shree Kumareshwar Hospital and Research Centre. The criteria for the diagnosis of DM was according to the criteria of the American Diabetes Association (ADA) 2007 guidelines. 8 50 subjects of similar age, sex and socioeconomic status served as controls. The controls were free from any major aliment which could affect the parameters under study (the clinical history or investigative results showed no involvement of any organ).The exclusion criteria included type 1 DM, Gestational diabetes , other specific causes for diabetes, micro- and mcro-vascular complications frank proteinuria detected by albustix, cigarette smoking and on lipid altering drugs like oral contraceptive, diuretics, beta blockers and lipid lowering drugs. Subjects with lipid altering diseases: hepatobiliary disease, hypothyroidism, chronic kidney disease and nephrotic syndrome were also excluded. Informed written consent was obtained from all the subjects enrolled for the study. Institutional ethical committee clearance was obtained for the study (Ref No:SNMC/09-10/612).The study was conducted from June 2009 to February 2010. A detailed history was taken to know duration of the disease, treatment history and any complication of the disease. All the subjects underwent clinical examination including anthropometric measurements. The anthropometric measurements comprised of waist circumference, height, body weight and body mass index (BMI) was calculated as weight in Kg/height in m2 .The waist circumference was determined by applying a tape measure to the midpoint between the inferior margin of the last rib and the crest of the ileum. Biochemical analysis-The fasting blood sample, 2 ml in fluoride bulb for sugar estimation and 5ml in plain bulb for lipid profile estimation was collected from the cubital vein with aseptic precaution. Serum was separated by centrifugation at 3000 rpm for 10 minutes.
The following parameters were studied.
1. Fasting blood glucose –Enzymatic, GOD-POD, end point colorimetric, single reagent chemistry.( Trinder P and Teitz N W by autospan kit method).
2. Serum total cholesterol – cholesterol oxidase / peroxidase method. CPT diagnostics kit.
3. Serum HDL cholesterol – phosphotungstate / magnesium precipitate method. Ident i kit.
4. Serum Triglycerides – Glycerol phosphate oxidase / peroxidase method, Ident i kit.
5. Serum VLDL cholesterol – calculated by formula Triglyceride / 5
6. Serum LDL cholesterol – calculated by formula LDL cholesterol = TC – (HDL-C+VLDL-C)
7. TC/HDL-C Ratio All the parameters read using semi auto analyser (Erba, Transasia).
8. Glycosylated Haemoglobin (HbA1c) was determined using Biorad equipment.
9. Lp (a) levels were determined using immunoturbidimetric methods. The statistical analysis was done using student‘t’ test and p value < 0.005 was considered statistically significant.
RESULTS
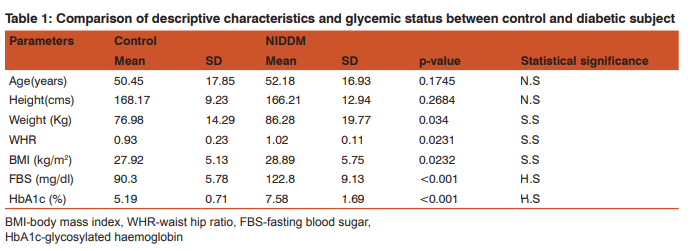
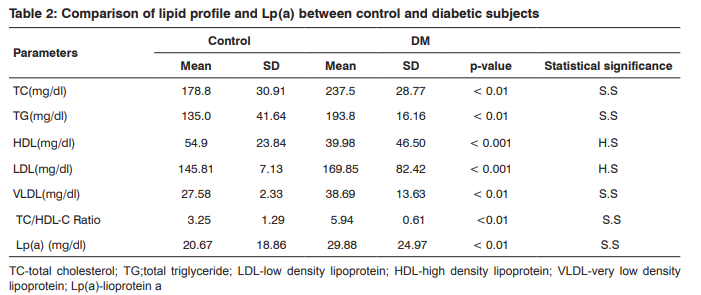
The descriptive characteristics and the glycemic status of the control and diabetics subjects are shown in table 1. There was no statistical significant difference seen in age and height of control and diabetic patients (p<0.05). The weight, WHR, BMI, levels of fasting blood glucose and HbA1c in diabetes mellitus patients were significantly elevated in comparison to healthy controls (P<0.001) (table 1). The levels of serum total cholesterol, serum triglycerides, serum LDL-C , serum VLDL-C, TC/HDL-C ratio and serum Lp(a) showed statistically significant elevation in DM subjects compared to control subjects ( P<0.001). The level of serum HDL-C was statistically significantly decreased in diabetes mellitus patients compared to healthy controls (P<0.001) .The results are shown in table no 2.
DISCUSSION
The number of people affected with type 2 DM has reached epidemic proportions worldwide. It is estimated that by 2020, there will be approximately 250 million people who will be affected worldwide 9 . Diabetes is associated with a variety of metabolic abnormalities, principal among which is hyperglycaemia and disturbances of carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action or both. The long term relatively specific effects of diabetes include development of retinopathy, nephropathy and neuropathy. The patients with diabetes are also at increased risk of cardiac, peripheral arterial and cerebrovascular disease 10. HbA1c reflects average plasma glucose over the previous 8 to 12 weeks. It can be performed at any time of the day and does not require any special preparations such as fasting .These properties have made it the preferred test for assesing the glycemic control in people with diabetes . More recently there has been substantial interest in using it as a diagnostic test for diabetes and as a screening test for persons at high risk of diabetes11. The main cause of the major feature of diabetic dyslipidemia is the increased free fatty acid release from insulin resistant fat cells.11 The increased flux of free fatty acids into the liver in the presence of adequate glycogen stores promotes triglyceride production which in turn stimulates the secretion of apolipoprotien B (apo B) and VLDL-C .This leads to enhanced hepatic VLDL-C production12.The abnormally increased TGs enrich high -density lipoproteins and low density lipoproteins leading to high levels of potentially atherogenic particles and low levels of HDL-C .13 The study showed significantly decreased level of the HDL-C in diabetic as compared to the healthy controls. The reduced HDL-C may be due to decrease in the activity of hepatic lipase resulting in decrease VLDL clearance leading to reduced HDL-C synthesis is the primary abnormality14 .The TC/HDL-C ratio is a sensitive and specific index of cardiovascular risk. The TC/HDL-C ratio is regarded as a predictor of CHD risk, especially with value ?6.0 15 Atherosclerosis is one of the common complications of DM and abnormal lipoprotein metabolism may account for the increased frequency of atherosclerotic lesions in diabetics. Elevated Lp(a) and low HDL were independent risk factors for premature coronary artery disease 16. Lp(a) interferes with the fibrinolytic function of plasminogen, thereby promoting the thrombotic events. It inhibits tissue plasminogen activator (t-PA) binding to fibrin and also suppresses the fibrin and fibrinogen fragment dependent enhancement of plasminogen activation by t-PA in some assay system 17. Lp(a) also inhibits plasminogen activation by streptokinase. It has been shown to compete for the binding of plasminogen to monocytoid cell and epithelial cells18. Tetraectin, a plasma protein ,binds reversibly to plasminogen and enhances plasminogen activation by t-PA. Lp(a) was found to bind to tetrenectin with higher affinity than Glu or Lys plasminogen 19. Systemic atherosclerosis measured as the peripheral occlusive arterial disease is strongly associated with serum Lp(a) in type 2 DM 20. The Lp(a) levels have also been suggested to play a pathogenic role in the development of complications like gangrenous foot lesions i patients of DM 21. Type 2 DM has a strong genetic component 22. The genetic basis of dyslipidemia has been well established 23. The genetic predisposition of both type 2 DM and the deranged Lp(a) levels may be a common basis of the two events occuring together. Lp(a) concentration in serum is also affected by apo(a) phenotypes. According to their electrophoretic mobilities Lp(a) has six phenotypesF,B,S1.S2,S3 and S4 as compared to apo B-100. Family studies are compatible with the fact that Lp(a) glycoprotein phenotypes are controlled bya number of autosomal alleles at a single lous. Comparison of Lp(a) levels in different phenotypes revealed a highly significant association of phenotype with concentration .Phenotype B,S1 and S2 are associated with high and phenotype S3 and S4 with low plasma concentration 24. It may be possible that increased Lp(a) concentrations in diabetics is due to the presence of apo(a) phenotypes and added to this are increased levels of insulin in patients with type 2 DM25.
CONCLUSION
In the present study the concentration of serum Lp(a), total cholesterol, serum triglyceride, LDL cholesterol and HbA1c is increased in the circulation of diabetic subjects than in controls, it may be the effect of hyperglycaemia on the the rate of synthesis , transcription and translation of apo (a). Glycosylation prolongs the half-life of proteins, this may add to higher levels of Lp(a) and HbA1c in diabetics compared to controls.
ACKNOWLEDGMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to authors /editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Ogbera AO:Burden of diabetes mellitus in Nigeria.Trop Doct 2007;37(3):153-154.
2. Smith S and Lall AM. A Study on Lipid Profile levels of Diabetics and Non-Diabetics among Naina Region of Allahaba d,India.2008;33(4):138-141.
3. AlbertiKG,Eckel RH,Grundy SM,Zimmet,Paul Z,Cleeman,James I.Donato karen harmonizing the metabolic syndrome.Ajoint interim statement of the International Diabetes Federation Task Force on epidemiology and prevention ;National Heart,Lung and Blood Institute;American Heart Association ;World Heart Federation ;International Atherosclerosis Society; and International Association for the study of Obesity.Circulation 2009;120:1640-45
4. Chattanda SP and Mgonda YM. Diadetic dyslipidemia among diabetic patients attending specialised clinics in Darer Salaam.Tanzania Med.J 2008;23(1):08-11.
5. Romics L,Karadi I,Csaszar A,Kostner G.Physiological and Clinical Importtance of Lipoprotein(a).J Exp Clin Med 1990;15:149-154.
6. Marshall SM,Barth JH.Standardisation of HbA1c measurements -a consensus statement.Diabet Med 2000;17:-6.
7. Naomi BM, Craig SW,Grad D,Noemie T,Cunningham CW,Hornell J,Pearce N, Jeffreys M. A New Zealand Linkage Study Examining the Association Between A1c Concentration and Mortality.2008;31(6):1144-49.
8. American Diabetes Association. Standards of medical Care in Diabetes. Diabetes Care.2007; 30:4-41.
9. Gitanjali G,Sudeep G,Neerja ,Mili G,Deepak A,Priyanka S. The effect of hyperglycemia on some biochemical parameters in diabetes millitus.2019;4(5):3181-3186.
10. Hanssen KF,Bangstad HJ,Brinchmann-Hansen O et al. Blood glucose control and diabetic microvascular complications:Long -term effects of near-normoglycemia. Diabet Med .1992;9:697-705.
11. Fox CS,Coady S,Sorlie PD et al. Increasing cardiovascular disease burden due to diabetes mellitus:The Framingham Heart Study. Circulation .2007;115:1544-1550
12. International Expert Committee report on the role of the A1c assay in the diagnosis of Diabetes. Diabetes care .2009;32:1327-1334
13. Alam SM, Ali S, Khalil M, Deb K, Ahmed A, Akhter K. Serum lipid profile in hypertensive and normotensive type 2 DM patients- a comparative study. Mymensingh Med J.2003;12(1):13-6.
14. Gambir JK,Kaur H,Gambir DS,Prabhu KM.Lipoprotein (a) as an independent risk factor for coronary artery disease in patients below 40 years of age. Indian Heart J . 2000;52:411-15.
15. Solfirizzi V, Panza F, Colacicco AM, Capurso C, DIntrono A, Torres F,et al. Relation of lipoprotein(a) as coronary risk factor to type 2 DM and low density lipoprotein cholesterol in patients ≥65 years of age.Am J Cardiol 2002;89:825-9.
16. Edelberg JM, Gonzalez-gronow M, Pizzo SV.Lipoprotein(a) inhibition of plasminogen activation by tissue-type plasminogen activator. Thromb Res 1990;57:155-62.
17. Karadi I, Kostner GM, Gries A, Nimpf j, Romics L, Malle E. Lipoprotein(a) and plasminogen are immunochemically related. Biochem Biophys Acta 1988;960:91-7.
18. Miles LA, Fless GM, Levin EG, Scanu AM, Plow EF. A potential basis for the thrombotic risks associated with lipoprotein(a). Nature 1989;339:301-3.
19. Kluft C, Jie AFH, Los P, de Wit E, Havekes L. Functional analogy between lipoprotein(a) and plasminogen in the binding to the kringle 4 binding protein,tetranectin. Biochem Biophys Res commun 1989;161:427-33.
20. Wollesen F, Dahlen G, Berglund L,Berne C. Peripheral atherosclerosis and serum lipoprotein(a) in diabetes. Diabetes Care1999;22:93-8.
21. Unluhizacri K, Muhtaraglu S, Kabak S,Bayram F, Kelestimur F. Serum lipoprotien(a) levels in diabetic foot lesions. Diab Res and Clin Pract 2006;71:119-23.
22. Singla S, Kaur K, Kaur G, Kaur H, Kaur J, Jaswal S. Lipoprotein(a) in type 2 diabetes mellitus: Relation to LDL:HDL ratio and glycemic control. Int J Diab Dev Ctries. Apr-June 2009;29(2):80-4.
23. Heller FR, Jamart J, Honare P. Serum lipoprotein(a) in patients with diabetes mellitus. Diabetes Care 1993;16:819- 23.
24. Uterman G,Mazel HJ,Kraft HG,Duba HC,Kemmeler HG,Seitz C.Lp(a) glycoprotein phenotypes inheritance and relation to Lp(a) concentrations in plasma.J Clin Invest 1987;80:458-65.
25. Habib SS. Serum lipoprotein (a) and high sensitivity C reactive protein levels in Saudi patients with type 2 diabetes mellitus and their relationship with glycemic control. Turkish Journal Of Medical Sciences.2013;43:33.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





