IJCRR - 6(19), October, 2014
Pages: 31-33
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
HEMODYNAMIC MIMICRY OF HYPERTROPHIC OBSTRUCTIVE CARDIO MYOPATHY : A CASE REPORT
Author: B. P. Chattopadhyay, Hamid Ali, Kapildev Mandal, Madhab Kumar Mondal, Anupam Mondal, Pranab Kumar Maity
Category: Healthcare
Abstract:A 64 year diabetic and hypertensive male suffering from ischaemic heart disease developed two episodes of syncopal attacks in quick succession followed by coffee-brown vomiting. He was in a state of shock following upper G.I. bleeding induced hypotension for which he was resuscitated with blood transfusion, volume repletion and inotropic support. Echo-doppler study during inotropic therapy showed hypercontractile LV with LVOT obstruction and gradient of 100 mm Hg across the LVOT. After the volume repletion echo-doppler study was repeated; the LVOT obstruction and the gradient across it was absent in repeat Echodoppler study. So echo-doppler study during inotropic treatment of shock in pre-existing hypertensive background (LVH) may temporarily mimic the haemodynamic findings of HOCM which disappears after stabilization of the shock state.
Keywords: HOCM (Hypertrophic Obstructive Cardio Myopathy), LVOT (Left Ventricular Outflow Tract) Obstruction Haemodynamic mimicry
Full Text:
INTRODUCTION
Hypertrophic Obstructive Cardio Myopathy(HOCM) is a common cardiac problem and the echo-doppler findings of HOCM can be mimicked by several other conditions. The differential diagnosis is very important because the line of management is different in different disease states. One such clinical condition is treatment of shock state with inotropic drugs in a patient who is having established hypertensive heart disease (LVH).
Clinical Summary
A 64 year old diabetic, hypertensive male presented with two episodes of syncopal attacks in quick succession which mandated admission in a city hospital outside our institute was known to be suffering from chronic stable angina and hypothyroidism since 1999. On 10.01.06 the patient had. On admission the patient had bouts of vomiting and the vomitus was coffee–brown in colour to start with, followed by frank haematemesis; it was accompanied by hypotension for which intravenous fluid and inotropes were started. Interrogation of past medication revealed that he was receiving aspirin, oral nitrates, Oral Hypoglycaemic Agents, ACE Inhibitors. On general examination the patient was observed to have pallor,tachycardia,B.P.80/60 mm of Hg and cold clammy extremities. On systemic examination there was tenderness in the epigastric region and there was a systolic murmur in the mitral area. Examination of the other systems including central nervous system was non-contributory.
Investigation summary
ECG revealed sinus tachycardia, LVH and 2 mm ST elevation in I,aVL,V5and V6; Trop-T was negative Capillary blood glucose was 223 mg/dl, Haemogram displayed Hb 6.6 g/dl with peripheral smear suggestive of hypochromic microcytic anaemia. UGI Endoscopy revealed 8 mm size active ulcer in the antrum with presence of altered blood in the stomach. Stool for occult blood test was positive (apart from G.I.
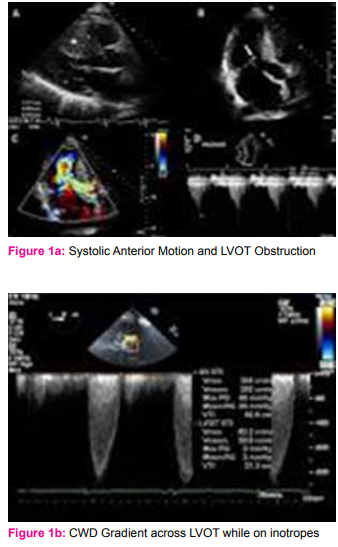
Bleeding induced true positivity, aspirin consumption may also lead to false positivity) CT Scan of brain revealed only age related cerebral atrophy. Carotid Doppler study revealed significant intimal thickening of both common carotid arteries without any significant stenosis. 24 hour Holter monitoring revealed no significant arrhythmia. Bedside Echo-doppler study (while the patient was on I/V fluid and inotropes) revealed IVS thickness 15mm,Posterior Wall thickness 12 mm. There was no typical asymmetric septal hypertrophy (septum to posterior wall ratio greater than 1.5) but there was systolic anterior motion of the anterior mitral leaflet causing dynamic LVOT Obstruction. The resting gradient of 100 mm of Hg across the LVOT(fig.1a and fig 1b) and LVH was noted.Pulse Wave Doppler revealed diastolic dysfunction .It was labeled as Hypertrophic Obstructive Cardio Myopathy outside. Inotropes were stopped and volume and blood replacement were emphasized.
Repeat Echodoppler study revealed thickness of IVS and PW to be 14.7 mm and 11.5mm respectively; there was no significant resting gradient across the LVOT. The LVOT gradient on Valsalva strain was found to be only 20 mm Hg. There was reduced diastolic compliance. There was no finding suggestive of HOCM. Another echo-doppler report (done in 1999) revealed concentric left ventricular hypertrophy and diastolic dysfunction. There was no suggestion of HOCM at that time as well.
Discussion
The purpose of the present case reporting is to draw attention to the differences in the three echo-doppler study findings. Echo on admission was done in the setting of intravenous inotropic therapy for treatment of hypotension following the G.I.Bleed. Noteworthy is the fact that the patient was hypertensive for more than 15 yrs. It has been described in the literature that the LVOT gradient mimicking HOCM can be encountered in the intensive care unit setting in the patients of hypotension following intravascular volume depletion especially while on concurrent inotropic agents 1. Often there is a history of underlying hypertension and the relatively low intravascular volume with augmented contractility result in hyperdynamic motion of the ventricle - an acquired form of dynamic LVOT obstruction2 .
Conclusion
Echodoppler suggestion of possibility of HOCM in patients of intravenous inotropic therapy for treatment of hypotension specially in the background of hypertensive heart disease should be critically reviewed after cessation of inotropic therapy and correction of shock and hypotension.High index of suspicion of such haemodynamic mimicry of HOCM helps establish actual diagnosis and management. Denial of opportunity of treating with Diuretics and many other drugs can be avoided by differentiation from HOCM.
Acknowledgements
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Dynamic left ventricular outflow tract obstruction in acute myocardial infarction with shock, Anand Chockalingam, Lokesh Tejwani et al, Circulation 2007:116e:110e-113.
2. Dobutamine mediated left ventricular outflow tract dynamic obstruction associated with hypovolaemic shock. M.Basalus, S.A.M. Said, P. Danse et al, The open Cardiovascular imaging journal,2010,Volume-2,page 14-1.7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





