IJCRR - 6(19), October, 2014
Pages: 24-30
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
MENTAL TAI CHI-BASED EXERCISE PROGRAMME VS TAI-CHI FOR INDIAN MULTIPLE SCLEROSIS PATIENTS: A PILOT STUDY
Author: Darshpreet Kaur, Kirandeep Kaur, Nidhi Billore, Gunjan Kumar, Ajay Kumar Singh
Category: Healthcare
Abstract:Background: Tai Chi postures have recently been shown in a number of randomized controlled trials to improve balance and posture in a variety of patient groups. Balance and mobility are problems commonly encountered by people with Multiple Sclerosis (MS). This pilot study examines the effect of Tai-Chi \? Mental practise on balance, gait and mobility in people with MS. Objective: To determine the efficacy of both protocols in inducing balance and mobility improvements.
Methods: About 25 volunteer MS patients were screened with Movement Imagery Questionnaire\-Revised second version (MIQ-RS), Modified clinical test of sensory organisation and balance (mCTSIB) and Expanded Disability Status Scale (EDSS) before being included in this study. 16 people satisfying the inclusion criteria with Relapsing Remitting MS (RRMS) were randomly assigned to either a Tai Chi group or to Tai chi with mental practise group. The first group participated in 20 sessions of total 60 minutes duration (20 minutes mental practise followed by 40 minutes tai-Chi), for 10-12 weeks The second group participated in 20 sessions which were 40 minutes long for 10-12 weeks. Out of all the known forms of Tai-Chi forms, six wereselected an d practised during these sessions. Results: There was no significant difference between group 1and group 2 for age, gender, MS duration, MIQ score, mCTISB and EDSS. Both the groups showed significant improvement (p< 0.05)post respective therapies. The percentage improvement post intervention in both the groups was comparable. Even though Group 1 performed better than Group 2 across most tests, the difference were not significant and consistent. Conclusions: Both the treatment protocols improve the balance and mobility of the RRMS patients and Tai Chi intervention showed considerable improvement in test scores. The impact of mental practice was not statistically significant across all tests. However, patients who were allotted to this group showed better comprehension of Tai Chi forms and higher retention rate.
Keywords: Mental Practise, Tai-chi, Multiple Sclerosis, Physical rehabilitation
Full Text:
INTRODUCTION
Multiple Sclerosis is a chronic neurological autoimmune disease which is characterized by problems in balance and coordination, motor impairment, fatigue and cognitive dysfunction. 1-4 As a consequence of multiple sclerosis, complications in walking and mobility are often debilitating and carry significant social as well as economic burden. 5 Imbalance also poses serious risk of falls which are often injurious. 6 Patients of Multiple Sclerosis therefore rely heavily on rehabilitation techniques such physical and occupational therapy. Tai Chi is a low impact, slow motion mind-body exercise which originated in China as a martial art. Over the years, Tai Chi has been repeatedly shown to improve balance, strength and gait in the elderly, the frail and patients of Parkinson’s disease. A sustained Tai Chi program (12 month duration) is reported to have long term positive effects by decreasing the number of falls as well as mental and emotional stress in various test groups.7-9 A previous study suggested the efficacy of Tai-Chi in improving balance and depression in patients of Multiple Sclerosis.10However; these results were not conclusive since they were mainly deduced from self-reported improvements in response to a subjective questionnaire. Therefore, the primary aim of this study was to test the hypothesis about the beneficial effects of Tai-Chi on balance and mobility in patients of Relapsing Remitting Multiple Sclerosis (n=16) using standardized, non-biased measuring scales. Also, rehabilitation therapies are often narrowly focused on improving a selected body function. Till date, there exists little research which links the effects of cognitive rehabilitation to balance and mobility. On the other hand, previous studies have repeatedly shown that mobility in MS is not an isolated problem and is interspersed with various other factors, of which cognitive impairment is one.11-12 One particular study demonstrated a decrease in walking ability when patients were simultaneously asked to perform a mental task.13 It is not known to what extent are symptoms of cognitive dysfunction in MS (typically-impairment in visuospatial functions, information processing, executive function, decrease in attention and concentration) responsible for motility problems. 14-16 Thus, there stands a need for an integrated approach to rehabilitation. For this purpose, an alternative regime of mental practice tailored specifically for impaired domains was administered in addition to 20-minute Tai Chi practice in the second part of this experiment. The additional effect of mental practice on mobility scores was observed.
SUBJECTS AND METHODS
Patients and controls
The inclusion criteria for recruiting the patients were: 1) A definite diagnosis of MS lasting >3 months as defined by Revised McDonalds 2010 criteria and 2)No visual impairment 3) No or minimal upper limb disability 4) Ability to walk independently. The exclusion criteria were 1) Presence of coexisting medical conditions potentially affecting cognition (e.g., vitamin B12 deficiency, hypothyroidism, chronic alcoholism, and active psychiatric disorders); 2) other conditions that might affect testing (e.g., hearing impairment), and 3) patients with significant depression or other psychiatric disorders assessed by the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders were excluded from the study. 4) Patients using any kind of assistive devise.5) Subjects who had already received the planned treatment regime were excluded. All subjects were of Indian ethnicity. The study was approved by the institutional ethical committee.
Test and study procedures
About 25 volunteer MS patients were assessed through convenient sampling. After an informed consent was obtained, subjects completed a questionnaire providing information about their age, the onset of pathology. They were screened with Movement Imagery Questionnaire-Revised second version (MIQ-RS), modified clinical test of sensory organisation and balance (mCTISB) and Expanded Disability Status Scale (EDSS) before being assigned into various groups. Four subjects dropped out because they had plans to travel out of city during study duration and two subjects dropped out for unknown reasons. All subjects were tested while they wearing their regular footwear and the assessments were carried out in one session. The assessment protocol consisted of two tests of static balance and two dynamic balance as primary outcome measures and a self-administered scales on balance confidence. Movement Imagery Questionnaire—Revised second version (MIQ-RS) Imagery training is more effective in individuals who are able to engage in imagery practice. The MIQ-RS requires movements of both the upper and lower limbs, thus assessing the ability to imagine one’s gross motor movements17. It consists of fourteen tasks. It has high test-retest reliability with a visual score of 0.83 and kinesthetic score 0.73. Modified clinical test of sensory organisation and balance (mCTISB) This test assesses patient’s balance under a variety of conditions to find out the source of instability. Time for which patient was able to maintain the starting position (maximum of 30 seconds) is recorded (in seconds). It also has good test-retest reliability (r = 0.99) for young adults18.
Dynamic Gait Index
This scale measures the mobility function and the dynamic balance of an individual. The performance is rated on a 4-point scale. The total score ranges from 0 to 24.DGI has high sensitivity (87%) in identifying fallers from non-fallers with a cut-off score ≤19 in multiple sclerosis patients19. Functional Reach (FR)- Lateral and Forward This test was developed as a clinically feasible measure of limits of stability in adults. The forward reach was chosen as the test task because it is not only a common functional movement, but it also mimics the leaning movements used to measure the excursion of the centre of pressure. It has a good intrarater reliability for Forward and Lateral reach, as measured with a yardstick (ICC3,1 = .98 and .96 respectively)20. Timed up and Go (TUG)
This test is used for measuring gait speed for a shorter distance. The TUG also provides information regarding everyday physical mobility like getting up, sitting down and turning.21In testing people with MS, the TUG had an intra-class correlation coefficient (ICC) of 0.982 Activities-specific Balance Confidence This is a scale in which the subject rates his or her perceived level of confidence while performing 16 daily living activities. Scores range from 0 to 100, where 100 means high level of confidence in balance skills. The validity and reliability of the scale has been found to be good for people with multiple sclerosis22.
Intervention
Following evaluation of balance disorders and group allocation, each subject received intensive practice with a Tai- Chi exercise programme (see Appendix). Sixteen people satisfying the inclusion criteria with RRMS were randomly assigned to either a Tai Chi with mental practise group or to Tai chi group. The first group participated in 20 sessions of total 60 minutes duration (20 minutes mental practise followed by 40 minutes tai-Chi), for 10-12 weeks .The second group participated in 20, 40 minutes long training sessions for 10-12 weeks .Out of all the known forms of Tai-Chi, six were practised during these sessions. Because of the high variability of symptoms a tailored rehabilitation programme was developed based on each group’s specific protocol. During the treatment sessions we stressed the function and quality of performance of Tai-Chi forms. The difficulty of the forms was based on the subject’s performance and followed their level of recovery. Specific and uniform guidelines for the intervention were developed and discussed with the physio therapists. Each subject, irrespective of group assignment, had a total of 20 sessions spread over ten-twelve weeks, each session lasting 60 minutes.
Statistical analysis
Data analyses included all 16 subjects who matched the inclusion criterion and completed the duration of this study. Statistical analysis was performed using the software Stata IC/13. Both the groups were compared for differences in baseline measures (EDSS, MIQ, mCTISB, MS duration, age and gender). The distribution of the data sets was tested for normality using Skewness-Kurtosis and Shapiro-Wilk test. Those which did not follow normal distribution were analysed using non- parametric tests (Wilcoxon signed-ranks test ). Normally distributed parameters were investigated for significance using paired t-test. Box-plots were constructed to estimate differences in median and percentiles of baseline parameters. The gain/ change scores were recorded in both the groups post intervention. The first step was to determine if the decided treatments have any significant effect on gait and balance of the subjects. This was done by performing t-test / Wilcoxon signed-ranks test on the pre and post test scores. The level of statistical significance was uniformly set at p<0.05 for all tests. In order to test the second hypothesis about the efficacy of mental practice and to delineate it from that of Tai Chi, gain scores were tested for significant differences between Group 1 and 2 using unpaired t-test and comparison of regression lines (wherein, the post test and pre-test data were used as the dependent and independent variables respectively).
RESULTS
No significant differences were observed between Group 1(Tai Chi + Mental Practice) and Group 2 (Tai Chi only) with respect to baseline measures (EDSS, MIQ, mCTSIB, age, MS duration and gender). The recorded scores are listed in Table 1. The test scores of EDSS, MIQ and mCTISB did not follow a normal distribution pattern and were therefore analysed using nonparametric tests. However, the MIQ test scores did show minor differences in distribution with respect to the median. {Fig 1(a-e): Box plot diagrams of baseline scores}


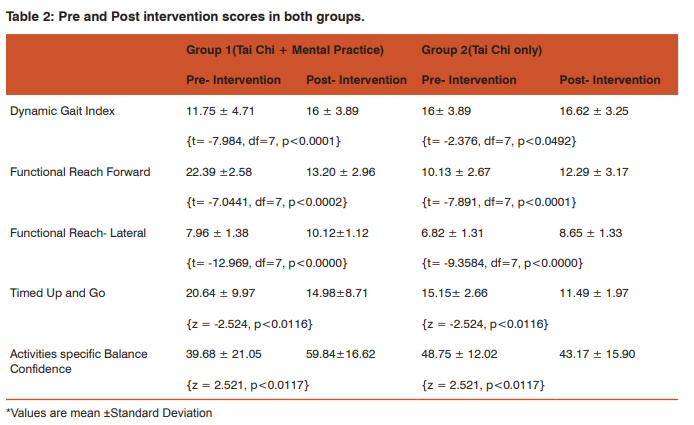

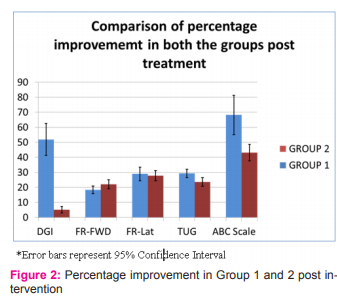
In both the groups, Tai Chi intervention showed statistically significant and positive results across all tests (Table 2). A paired t-test on the pre-intervention and post intervention scores of Dynamic Gait Index and Functional Reach revealed significant differences in both group 1 and 2 (p<0.05). The scores of the ‘Timed up and go’ and the Activities-specific Balance Confidence scale were again, not distributed normally. But Wilcoxon signed-ranks test on TUG and ABC scales again revealed clear significant differences between pre and post intervention scores ( p<0.05). Mental practice/ imagery however, did not reveal consistent and significant effect on the Gait and balance of subjects in Group 1 (Table 3). The finest impact of mental practice was seen in DGI and the subjective confidence scale which revealed clear differences in t-tests. But the results in Functional Reach and TUG were insignificant and ambiguous (Figure 2). A greater sample size would be required to assess the impact of mental practice in detail.
DISCUSSION
To the best of our knowledge, this is the first study to evaluate the effects of Tai-Chi on balance and mobility in Indian patients of Multiple Sclerosis .The objective of this study was two pronged. In the first part we wished to understand whether or not Tai Chi training can be used as a potent rehabilitation therapy for improving gait and balance in patients of Relapsing Remitting MS. The second step was to assess if a session of mental imagery can have additional effects (positive or negative) on the acquired results. There was an unambiguous improvement post intervention in all the tests and in both the groups. The percentage increase in test scores varied between 5% and 55% depending on the test in question, but usually averaged between 20-30%. These results were in synchronization with an earlier study briefing the effect of Tai-Chi on MS patients10 (Mills et al). Even though this previous study was conducted on non-objective test scales and on patients who were in the secondary progressive stage of MS, it highlighted the improvement in walking distance, steadiness and the ability to stand on one leg. Thus, this study supports the theory that Tai-Chi improves dynamic balance and mobility in patients of Multiple Sclerosis. The effect of mental practice was statistically weak but consistent across most of the tests. Although, mental practice did not have a significant impact on measures of gait and balance, it proved useful in other ways. Firstly, it played an important role in retaining the interest of patients in Tai Chi therapy. Six months after the completion of the study, the patients in mental imagery group reported performing these exercises at home at least thrice a week. On the contrary, the group which received only Tai-Chi training reported discontinuation due to difficulty in remembering postures in the absence of an expert. This group also showed a much greater improvement on confidence scales post intervention, in comparison to the group which did not receive mental training. On the other hand, patients of the Tai Chi (only) group were more hesitant and showed lesser interest as well as comprehension during the training sessions. Another interesting observation was that patients showed greater improvement in activities specific balance confidence (ABC) scale (43- 68%) in comparison to other tests. This trend can indicate that patients felt more confident regarding their gait and balance after Tai- Chi training, even if that confidence did not materialize into actual improvement to the same degree. Tai Chi is merely one amongst the many proposed therapies for MS. Yoga23,24, Aerobics, physiotherapy and certain exercises have earlier been positively correlated with improvement in balance and walking . The degree of improvement observed in Tai Chi was comparable to those recorded in others, the analyses of which can be a topic for another study. Although the sample size of 16 patients limits the study’s statistical power, its results have sufficient clinical significance for bringing this pattern of treatment into practice. In summary, the present study provides information regarding the utility of Tai-Chi, with or without mental practice, as an efficient therapeutic tool, to cater to balance and mobility issues in Multiple Sclerosis patients. However, patients who were allotted to mental practise group along with Tai-Chi group showed better comprehension of Tai Chi forms and higher retention rate.Further studies are needed on larger cohort.
ACKNOWLEDGEMENT
We thank all our participants for accepting to be a part of this study. Their willingness was an important driving force for our team to go ahead with this novel technique. We are thankful to our physiotherapists for playing a key role. We thank ECTRIMS to include this work for poster presentation at 29th Congress of the European Committee for Research and Treatment in Multiple Sclerosis (ECTRIMS) and the 18th Annual Conference of Rehabilitation in MS (RIMS) in Copenhagen, Denmark, 2– 5 October, 2013. These were not the sources of financial assistance for this study. Authors acknowledge the im- Authors acknowledge the im- Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Geoffrey L. Sheean, Nicholas M. F. Murray, John C. Rothwell, David H. Miller, Alan J. Thompson,An electrophysiological study of the mechanism of fatigue in multiple sclerosis Brain (1997), 120, 299–315.
2. Benedetti MG, Piperno R, Simoncini L, Bonato P, Tonini A, Giannini S. Gait abnormalities in minimally impaired multiple sclerosis patients., MultScler October 1999 vol. 5 no. 5 363-368.
3. Rao SM, Leo GJ, Bernardin L, UnverzagtF.Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction.Neurology. 1991 May;41(5):685-91.
4. Frzovic D, Morris ME, Vowels L.Clinical tests of standing balance: performance of persons with multiple sclerosis. ArchPhys Med Rehabil. 2000 Feb;81(2):215-21.
5. Pike J, Jones E, Rajagopalan K, Piercy J, Anderson P.Social and economic burden of walking and mobility problems in multiple sclerosis.BMC Neurol. 2012 Sep 18;12:94.
6. Matsuda PN, Shumway-Cook A, Bamer AM, Johnson SL, Amtmann D, Kraft GH.Falls in multiple sclerosis.PM R. 2011 Jul;3(7):624-32.
7. Wolfson L, Whipple R, Derby C, Judge J, King M, Amerman P, et.al.Balance and strength training in older adults: intervention gains and Tai Chi maintenance.J Am Geriatr Soc. 1996 May;44(5):498-506.
8. Lan C, Lai JS, Chen SY, Wong MK.12-month Tai Chi training in the elderly: its effect on health fitness.MedSci Sports Exerc. 1998 Mar;30(3):345-51.
9. Jin P.Efficacy of Tai Chi, brisk walking, meditation, and reading in reducing mental and emotional stress.JPsychosom Res. 1992 May;36(4):361-70.
10. Mills N, Allen J, Morgan SC. (2000). Does Tai Chi/Qi Gong help patients with multiple sclerosis? Journal of Bodywork and Movement Therapies2000; 4(1):39-48.
11. Fischer JS,FoleyFW,Aikens JE .What do we really know about cognitive dysfunction,affectivedisorders,and stress in multiple sclerosis A practitioner’s guide.JNeuroRehabl. 1994;8(3):151–164.
12. Chan A, Heck C. Mobility in multiple sclerosis: more than just a physical problem. Int J MS Care. 2000; 3: 35–40.
13. Motl RW, McAuley E, Sandroff BM.Longitudinal change in physical activity and its correlates in relapsing-remitting multiple sclerosis.PhysTher. 2013 Aug;93(8):1037-48.
14. Amato MP, Ponziani G, Pracucci G, Bracco L, Siracusa G, AmaducciL.Cognitive impairment in early-onset multiple sclerosis. Pattern, predictors, and impact on everyday life in a 4-year follow-up.Arch Neurol. 1995 Feb;52(2):168-72.
15. Bagert B, Camplair P, BourdetteD.Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management.CNS Drugs. 2002;16(7):445-55.
16. Piras MR, Magnano I, Canu ED, Achene A, Solinas G, Aiello I.Longitudinal study of cognitive dysfunction in multiple sclerosis: neuropsychological, neuroradiological, and neurophysiological findings.J Neurol Neurosurg Psychiatry. 2003 Jul;74(7):878-85.
17. Gregg M., Hall C, Butler A.The MIQ-RS: A Suitable Option for Examining Movement Imagery Ability.Evid Based Complement Alternat Med. 2010 Jun;7(2):249-57.
18. Cohen H, Blatchly CA, Gombash LL.A study of the clinical test of sensory interaction and balance.PhysTher. 1993 Jun;73(6):346-51.
19. Forsberg A, Andreasson M, NilsagårdYE.Validity of the Dynamic Gait Index in People With Multiple Sclerosis.Physical Therapy October 2013 vol. 93 no. 10 1369-1376.
20. Thompson M, Medley A.Forward and lateral sitting functional reach in younger, middle-aged, and older adults. JGeriatrPhysTher. 2007;30(2):43-8.
21. Nilsagard Y, Lundholm C , Gunnarsson LG , Dcnison E. Clinical relevance using timed walk tests and ‘timed up and go’ testing in persons with multiple sclerosis. Physiother Res Int. 2007; 12: 105–114.
22. Nilsagård Y, Carling A, Forsberg A.Activities-specific balance confidence in people with multiple sclerosis.MultScler Int. 2012;2012:613925.
23. Maria G., Susan C., Neasa H, Aidan L, Jean S.Getting the Balance Right: A randomised controlled trial of physiotherapy and Exercise Interventions for ambulatory people with multiple sclerosis.BMC Neurology 2009, 9:34
24. Mass M.,Oken B.S., Kishiyama S.,Zajdel D.,Bourdette D.,CarlsenJ.et.al.Randomized controlled trial of yoga and exercise in multiple sclerosis.Neurology. 2004 Jun 8;62(11):2058-64.
APPENDIX
The rehabilitation protocol ensured that each exercise group had a consistent intervention schedule on key training parameters which included the duration (60 minutes per session), frequency (2 times per week for 10 weeks), and training structure (i.e., a 5- to 10-minute warm-up, core activities, and a 5-minutecool-down). Participants in all three conditions were instructed not to engage in any additional home practice.
Group1: Received balance rehabilitation to improve motor, sensory and cognitive strategies.
Group2: Received balance rehabilitation to improve motor and sensory strategies. For improving motor strategies, 6 forms of Tai-Chi were selected. Training of Gait patterns was also borne in mind while designing Tai-Chi programme for both the groups. These tasks required stepping in different directions, while challenging subject’s postural stability and balance control. The somatosensory information was encouraged by large and coordinated movements in order to move the center of mass with speed, safety and balance.Emphasis was laid on improving vestibular and somatosensory information by a reduction of visual input. For this purpose certain forms of Tai-Chi were performed in different perceptual contexts. The patients were encouraged to exercise in eyes-closed condition. Group 1 also engaged in mental imagery of the desired tasks, while Group 2, underwent relaxation during that duration. For this purpose episodic memory of the patients in group 1 was targeted. Anterograde component of their memory was put into action by providing visual stimulation of the Tai-Chi form, which they will be performing on that day. Lapses in working memory were challenged by intermittently questioning about their perception of visual inputs. To insure proper execution of Tai-Chi forms patients were asked about the relevance of particular form to them and potential benefits they seem to obtain from it. Throughout 40 min Tai-Chi session it was ensured that both the groups perform symmetrical and coordinated movements such as trunk rotation and weight shifting from one foot to another foot, Controlled and coordinated displacement of the body’s center of mass over the base of support, Ankle sway toward and around the perimeter of the base of support, dynamic eye and head movements and anterior-posterior and medial-lateral stepping with rhythmical weight shifting for each form.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





