IJCRR - 6(19), October, 2014
Pages: 21-23
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
COEXISTENCE OF NON-HODGKIN LYMPHOMA AND EXTRAMEDULLARY HAEMATOPOIESIS IN
A LYMPH NODE: A UNIQUE CASE DIAGNOSED BY FINE NEEDLE ASPIRATION CYTOLOGY
Author: Arindam Karmakar, Tanushree Ghosal, Gopinath Barui, Ranjana Bandyopadhyay, Subhalakshmi Mukhopadhyay
Category: Healthcare
Abstract:Aim: Non-Hepatosplenic extramedullary haematopoiesis is an uncommon finding and Extramedullary haematopoiesis (EMH) in lymph nodes is further rarity. This effort aims at highlighting an extremely rare coexistence of the two in the same lymph node. Case report: We report an old man with co-existent Non-Hodgkin lymphoma and EMH in the same lymph node diagnosed by FNAC. Discussion: It is rare to find extramedullary haematopoiesis in enlarged lymph nodes subjected to FNAC. To the best of our knowledge no case of co-existent Non-Hodgkin lymphoma and EMH has been reported previously. Conclusion: This case emphasizes the possibility of Extramedullary haematopoiesis (EMH) in an enlarged lymph node with or without other pathological processes. It also underscores the significance of proper correlation of information for the diagnosis of the ailment which in this case could be done with very simple investigation protocol.
Keywords: Coexistence, Extramedullary hematopoiesis, Lymph node, Non-hodgkin lymphoma
Full Text:
INTRODUCTION
Extramedullary haematopoiesis (EMH) occurs when bone marrow is destroyed due to some disease process like myelofibrosis or the marrow is replaced by malignant cells or storage cells. Lymph node may be the site of extramedullary haematopoiesis in case of myelofibrosis, haematolymphoid malignancy etc. but coexistence of Non-Hodgkin lymphoma and extramedullary haematopoiesis in the same lymph node is a very unusual finding. Here we report a case of a 63 year old male patient having extramedullary haematopoiesis coexisting with Non-Hodgkin lymphoma in the right supraclavicular lymph node which was diagnosed by FNAC.
Case Report
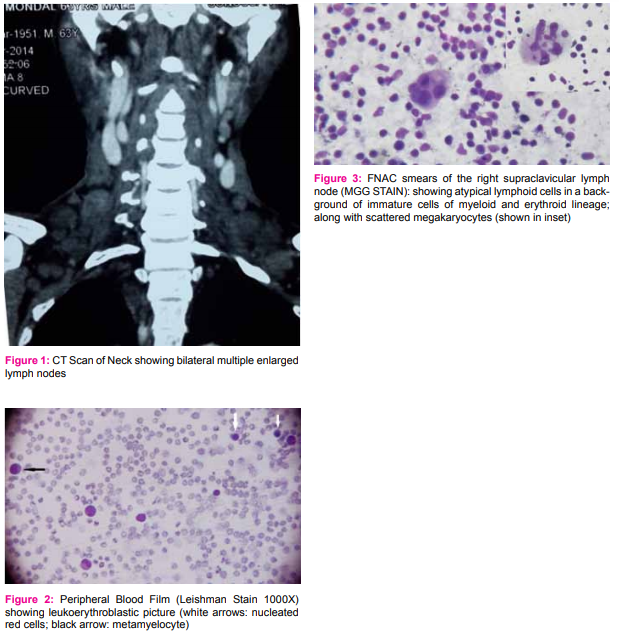
A 63year old male patient presented with multiple swellings in neck; weakness, abdominal discomfort for the last 6 months. On clinical examination severe anaemia, bilateral cervical lymphadenopathy (1-2 cm size) and mild hepatosplenomegaly were found. CT scan of neck revealed multiple enlarged lymph nodes at right lower jugular, bilateral supraclavicular, bilateral paratracheal (right>left), pretracheal, precarinal, aorto pulmonary, subcarinal and bilateral hilar regions. Routine haematological investigation revealed Hb -6.0 g%, TLC 24000/cmm , Platelets- 60000/cmm, NRBC – 16/100 WBC. Leukoerythroblastic blood picture was seen on examination of the peripheral smear. FNAC of the right supraclavicular lymph node was requested which was done using 23G needle. MGG stained smears revealed high cellularity comprising predominantly mixed population of atypical lymphoid cells. Along with lymphoid population some immature cells of myeloid and erythroid lineage were seen. Megakaryocytes, identified by the presence of large multilobated nuclei and abundant granular eosinophilic cytoplasm, were seen consistently scattered along the smears. A diagnosis of Non-Hodgkin Lymphoma along with extramedullary haematopoiesis was made based on cytomorphology.
Discussion
Extramedullary haematopoiesis occurs in various sites including liver and spleen. Occasionally it involves other organs. It is rare to find extramedullary haematopoiesis in enlarged lymph nodes subjected to FNAC. While reviewing literature we found cases depicting coexistence of leukaemic infiltration and extramedullary haematopoiesis in the same lymph node [1] but we are yet to encounter any past record of coexistence of Non-Hodgkin Lymphoma and extramedullary haematopoiesis in the same lymph node. Without the relevant haematological investigations, differential diagnosis on FNAC smears is that of myeloid sarcoma; inflammatory disorders; lymphoma and metastatic carcinoma with multinucleated giant cells. Morphological findings aided by clinical and haematological findings are sufficient enough to distinguish extramedullary haematopoiesis from others [2,3]. Although Non-Hepatosplenic Extramedullary Hematopoiesis (NHS-EMH) is often associated with myelofibrosis with myeloid metaplasia (MMM) or thalassemia, it can also accompany other disorders, including hereditary spherocytosis, sickle cell anaemia, congenital dyserythropoietic anaemia, immune thrombocytopenic purpura, chronic myeloid leukaemia, polycythaemia vera, myelodysplastic syndrome, Paget disease, osteopetrosis, and Gaucher disease and treatment with myeloid growth factors. Occasionally, an associated disease is not identified [4]. Clinically, NHS-EMH may present as an incidental finding or with a symptomatic disease or condition, including pleural effusion, ascites, neurologic deficit, cardiac tamponade, chronic renal failure, acute respiratory failure, orbital proptosis, and subglottic stenosis [4]. In a retrospective review of cases of non-hepatosplenic extramedullary haematopoiesis by Koch C.Y. et al, 27 cases were found of which most (26%) were around vertebra as well as in lymph nodes (inguinal, para-aortic, para-tracheal and cervical) , retroperitoneum, lung, pleura, genitourinary tract, skin etc. 18 cases were diagnosed as myelofibrosis with myeloid metaplasia (MMM) of which 12 were diagnosed as agnogenic myeloid metaplasia and 6 were diagnosed as post-polycythemic myeloid metaplasia. Of the 9 cases in the non-MMM group, 3 patients had congenital anaemia; 2 cases had chronic lymphocytic leukemia; 3 cases having chronic myeloid leukemia, pachydermoperiostosis and cerebrovascular malformation respectively. One case had no detectable underlying disorder. Cases involving lymph nodes were associated with agnogenic myeloid metaplasia and postpolycythaemic myeloid metaplasia [4]. Mass-forming foci of NHS-EMH, sometimes mimicking tumor were also reported [2,3,5]. Our case depicts a very rare instance having features of non-hodgkin lymphoma and extramedullary haematopoiesis in the same lymph node diagnosed by FNAC with guidance from the relevant clinical, haematological and radiological findings.
Conclusion
Non-Hepatosplenic extramedullary haematopoiesis is an uncommon finding and EMH in lymph nodes is further rarity. This case emphasizes the possibility of EMH in an enlarged lymph node with or without other pathological processes. It also underscores the significance of proper correlation of information for the diagnosis of the ailment which in this case could be done with very simple investigation protocol.
Abbreviations
EMH = Extramedullary haematopoiesis
FNAC = Fine Needle Aspiration Cytology
NHL = Non-Hodgkin lymphoma
NHS-EMH = Non-hepatosplenic extramedullary haematopoiesis
Hb=Haemoglobin
TLC = Total Leukocyte count
NRBC = Nucleated red blood cells
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature of this article has been reviewed and discussed.
References:
1. Singhal N, Tahlan A, Bansal C, Handa U, D’Cruz S. Coexistence of leukemic infiltration and extramedullary hemato-poeisis in a lymph node: A cytological diagnosis. J Cytol. 2011 Jul-Sep; 28(3):138-140.
2. Policarpio-Nicolas M, Bregman S, Ihsan M, Atkins K. Massforming extramedullary hematopoiesis diagnosed by fineneedle aspiration cytology. Diagn Cytopathol. 2006 December; 34(12):807-11.
3. Jan Y, Chen J, Chang M, Ho W. Fine-needle aspiration cytology of retroperitoneal extramedullary hematopoiesis: a case report. Kaohsiung J Med Sci. 1998 October; 14(10): 659-63.
4. Koch CA, Li CY, Mesa RA, Tefferi A. Nonhepatosplenic Extramedullary Hematopoiesis: Associated Diseases, Pathology, Clinical Course, and Treatment. Mayo Clin Proc. 2003; 78:1223-33.
5. Ahuja S, Grover G, Jha A, Sodhi K, Bansal D, Dey P. Extramedullary hematopoiesis presented as solitary renal mass: a case report with review of literature. Diagn Cytopathol. 2011 June; 39(6):435-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





