IJCRR - 6(19), October, 2014
Pages: 14-20
Date of Publication: 10-Oct-2014
Print Article
Download XML Download PDF
CHANGING PATTERNS OF AETIOLOGY OF ACUTE SPORADIC VIRAL HEPATITIS IN INDIA - NEWER INSIGHTS FROM NORTH-EAST INDIA
Author: Anup Kumar Das, Sakir Ahmed, Subhash Medhi, Premashish Kar
Category: Healthcare
Abstract:Background: Most common aetiology of viral hepatitis globally is Hepatitis A except in developing countries where Hepatitis E predominates. Geographical variation is present between the west and the east. However, in many developing countries including India, a change in aetiology is being increasingly reported in the past two decades.
Materials & Methods: 591 patients with acute viral hepatitis were prospectively screened to ascertain their aetiology (by appropriate viral markers) in a tertiary care centre from North-East India. Results were double-checked in another tertiary institute in Delhi, including Polymerase Chain Reaction for virus detection. Clinical outcomes, mortality and other relevant findings were recorded. Results: Hepatitis A was the dominant aetiology for both acute and fulminant viral hepatitis that is in contrast to other Indian reports that implicate hepatitis E virus, suggesting our region has certain differences. Overall, 16% developed complications with a 9% mortality. Those with hepatitis B had the poorest outcome. Hepatitis C virus was not detected. 2% had mixed infection. Non-A,B,C,E cases were high. History of herbal/unknown folk medicine intake was present in a large number of patients. Conclusion: North-east India, although relatively underdeveloped, is showing a shift of hepatitis A viral sero-epidemiology. Adults are affected as equally by hepatitis E. The reasons may be multi-factorial. Non-viral acute hepatitis is common here. The consumption of unidentified non-allopathic medications may influence outcome, and requires further evaluation.
Keywords: Acute viral hepatitis, Northeast India, Changing aetiology, Herbal medication induced liver damage
Full Text:
INTRODUCTION
Outbreaks of hepatitis have been recognized for centuries, but the first description of epidemic jaundice due to hepatitis is attributed to Hippocrates [1]. Acute Viral Hepatitis (AVH) is mainly caused by hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), and hepatitis E virus (HEV). They can be identified by serological tests only. Hepatitis A is the most common cause of acute viral hepatitis (AVH) worldwide. Viral hepatitis is a major public health problem in India too, which is hyperendemic for both HAV and HEV. [2] Most reports from India implicate HEV as the major cause, ranging from 12.6-78.6% in both sporadic and epidemic hepatitis from different parts the country [3,4,5,6,7,8] However, HAV AVH is the most common cause of acute viral hepatitis globally having a worldwide distribution. [9,10] Major geographical differences in endemicity of HAV exist and are closely related to hygiene and sanitary conditions and the level of socioeconomic development. In less developed regions and in several developing countries, HAV infection is still very common in the early years of life and its seroprevalence rates approach 100%.[11] In many other Asian countries too, HAV infection remains highly endemic. Studies from Pakistan in the 1980s, 1990s and 2000s show that >50% of children acquire anti-HAV immunity by their preschool years and nearly all adolescents and adults are immune. Between the 1980s and 1990s in Nepal, nearly all adolescents were immune by age 15. In Bangladesh, >50% of 5 year olds and almost all adolescents and adults are immune.[12]
It is believed that in our country, being in a hyperendemic zone, most of the population acquires HAV infection during childhood, which is mostly asymptomatic and then achieve lifelong immunity. But with increasing age of acquisition, both symptomatic diseases and serious complications like acute liver failure (ALF) increase. In addition, it is well known that superimposed acute HAV infection can worsen the prognosis in pre-existing chronic liver disease. However, some workers in India have recently reported that more adults are now at risk of developing HAV infections in different metropolitan cities of the country [13], and India may be in a transition in respect to seroprevalence of anti-HAV IgG that is similar to European countries. [14] Therefore, there are some conflicting reports from different regions within India, suggesting a geographical difference as regards the aetiology of AVH. Both HEV and HAV are enterically transmitted with similar risk factors, but the clinical course of hepatitis E is usually more severe than hepatitis A, frequently complicated by coagulopathy and cholestasis. Hepatitis E is mostly self-limiting but may develop into fulminant hepatitis, especially in pregnant females. Comprehensive data from the Northeastern part of India on the aetiology of AVH is lacking. Therefore, this observational, prospective study was undertaken to study the aetiology of acute viral hepatitis from this region.
MATERIALS AND METHODS
The study population included patients of suspected Acute Viral Hepatitis attending the Assam Medical College Hospital, Dibrugarh, Assam, India (a tertiary care teaching hospital), in the Medicine OPD and indoor wards from September 2005 to December 2013. Institutional Ethics Committee approval was obtained before the study. A total of 591 patients (aged 14 to 55 years) were included after written informed consent. Patients with acute onset signs and symptoms consisting of jaundice ( serum bilirubin > 3 mg/dL), ALT and AST > 3 times upper normal, malaise, fatigue, fever, nausea, anorexia, abdominal pain, vomiting, high coloured urine, altered sensorium, or encephalopathy were included in the study. The development of acute liver failure during the observation period and outcome of the illness was noted. Chronic liver disease patients were excluded by clinical, biochemical and radiological investigations, as well as past medical history/records when available. Other metabolic causes/infections/collagen diseases for disturbed sensorium were ruled out by laboratory and biochemical tests. CSF examination was done when indicated for excluding viral/bacterial/tubercular meningo-encephalitis. Those on anti-tubercular drugs were excluded. Detailed history regarding family contacts, travel, blood transfusion, occupation, source of drinking water, tattooing, herbal medication intake, food habits, alcohol intake (where appropriate with duration, type and amount), residence in urban/rural area and income were obtained. Pre-referral medical prescriptions, if any, were scrutinized for hepatotoxic drugs. Serum samples were collected and tested for the major hepatotropic Viral Markers in our college. All sera were tested for antibodies to hepatotropic virus; the serological tests included IgM anti-HAV (General Biologicals Corp., Taiwan), HBsAg (General Biologicals Corp., Taiwan), IgM anti-HBc (Radim Diagnostics, Rome, Italy), anti-HCV antibody using a third-generation enzyme immunoassay (EIA) kit (Ortho Diagnostics Inc., NJ, USA) according to the manufacturer’s instructions and, IgM anti-HEV (Immunovision, USA) using third-generation EIA Kits. Serum alanine aminotransferase (ALT), and aspartate aminotransferase (AST) were determined from the serum aliquots using commercial kits (Boehringer Mannheim, Germany) as per the manufacturer’s instructions. The results were re-validated in the Virology Laboratory in the Maulana Azad Medical College, Delhi. The sera were sent in small aliquots in dry ice-packs. Positive samples were re-tested in duplicate at the PCR laboratory of the Dept of Gastroenterology, Maulana Azad Medical College, Delhi. All seronegative sera were tested for amplification of HBV DNA and HCV RNA by real time PCR. Only HBV and HCV PCR negative cases were included in Non-B & C group of cases. Anti-HCV positive sera were tested further for HCV-RNA, which was detected based on the 5’ UTR-core region and whenever positive, were labeled as HVC.
RESULTS
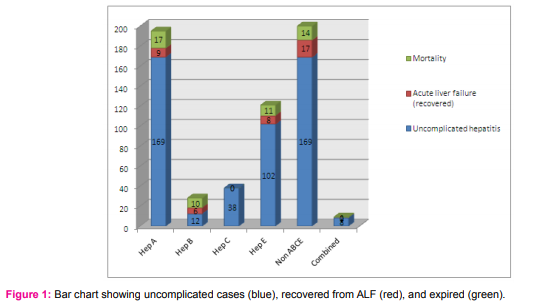
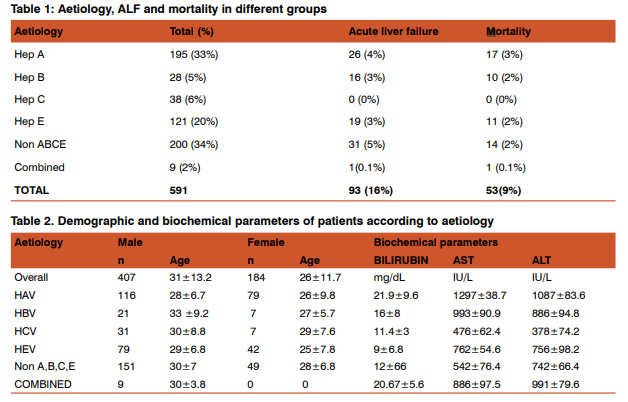
Out of 591 cases, 448 belonged to rural or semi-urban area. On an average, all patients presented to us in the second week of their illness. On enquiry, 243 (41%) used to consume unsafe drinking water. Of the study group, 69% were male (405 of 591). The average age of males in our study was ~ 31 years, and that of females ~ 5 years less. 382 (65%) patients were positive for hepatotropic viruses, while 200 (34%) had non-ABCE hepatitis (Table 1). 9 (2%) patients had combined viral infections.HAV was most common (33%) in AVH out of which 4% developed ALF. Summarizing the total outcome, 93 (16%) of 591 cases developed ALF and 9% expired. The highest mortality was in the Hepatitis A group (17 cases, 9% of total 195 Hepatitis A). But the highest proportionate mortality was seen in the Hepatitis B group (10 of 22 cases, or 36%). In the Hepatitis E group (n:121), a mortality of 9% seen. The non- ABCE hepatitis group (n:200) had 19 ALF (5% of all cases) cases with a mortality of 7% (Fig 1). Some demographic and biochemical parameters of patients in different aetiology are shown in Table 2. 50% of all patients had a history of intake of various herbal medications before coming to hospital, but could not specify the type or content of the herbal medications. Of all ALF cases, 84% had a history of ingestion of herbal medications. 60% of non-ABCE hepatitis had taken herbal medications. Paracetamol was consumed in 30% of all cases before presenting to our institute. The leading cause of AVH in Pregnancy was Hepatitis A (9 of 15) without any Hepatitis E. (Table 3).
DISCUSSION
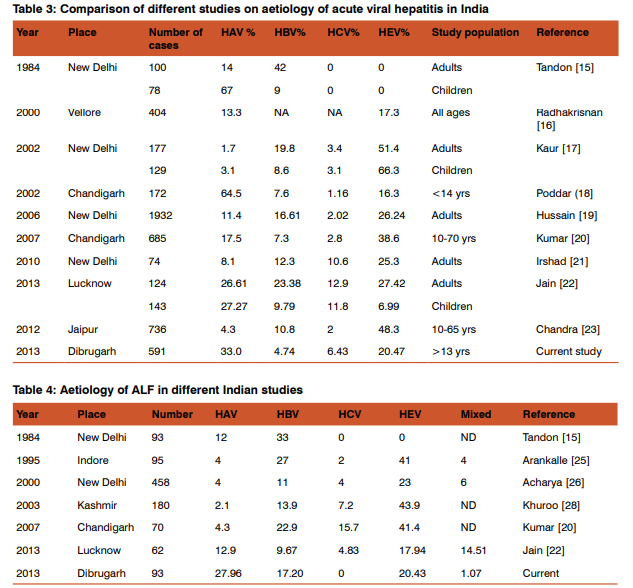
The subjects affected by AVH in our series were young, active and of productive age, thus, leading to significant loss of DALYs. They mostly belonged to rural areas. Table3 shows the comparison of various Indian studies on the aetiology of AVH [15,16,17,18,19,20,21,22,23] with our study. Except in children from Chandigarh and Lucknow, all other studies have found Hepatitis E as the commonest cause of acute viral hepatitis. In our country Hepatitis E reportedly occurs as mostly sporadic hepatitis with periodic resurgence and is responsible for 30-70% cases of acute sporadic hepatitis,[24] primarily affecting young adults between 15-40 yr of age in an endemic region [25]and is the major cause of ALF [26]. Indian seroprevalence studies also reveal that 90%- 100% of the population acquires anti-HAV antibody and becomes immune by adolescence [2] and hence HEV is found to be the most common cause of acute sporadic hepatitis. [27] Nevertheless, our study highlights Hepatitis A as the commonest cause for both AVH and ALF. Notably, significantly more ALF occurred in the non-viral group. A third of the all ALF cases were due to Hepatitis A (Table 1), but the highest proportion of deaths due to ALF occurred in HBV group compared to HAV or HEV. It appears that HBV is not a common cause for ALF in our region (Table 4), compared to other Indian studies [15,20,22,25,26,28]. The rest of India shows Hepatitis E as the leading cause of ALF in most studies. However, the proportion of cases of fulminant hepatitis A who survived was greater compared to the proportions of survival for Hepatitis B or Hepatitis E. This series shows that acute hepatitis B has a poor outcome in our setting, and acute Hepatitis C is rare in ALF in our region. We found that ALF in both viral AVH and non-ABCE group had an almost similar mortality. HAV expectedly showed a slightly higher mortality compared to HEV as it is established that in adults AVH due to HAV produces a more severe disease. There is a paradox in the rise of liver enzymes seen in various groups (Table 2). The lowest average levels of liver enzymes were for Hepatitis B, while the highest was for hepatitis A and can be explained by more hepatocyte injury in the HBV group. Hepatitis C group showed the minimum rise of bilirubin with Hepatitis A showing the maximum rise. The rise of liver enzymes may correlate inversely with mortality, but this remains to be validated. There is no difference in the clinical course of patients with non-ABCE hepatitis compared to those positive for the major hepatotropic virus. In India, non-viral AVH is not uncommon [29] and our findings confirm this. In our series, overall mortality in ALF in the viral group was higher than in non-ABCE group. We had 34% cases without any positive viral serology. In a study involving 165 south-east Asian adult patients with AVH (from India, Nepal, Pakistan), a specific etiologic diagnosis was made in 122 (74%) patients where acute hepatitis E occurred in 40%, HAV in 18.7%, HBV in 11.5%, HCV 1.2%, and combined infection in 4.2%. No viral aetiology could be confirmed in the rest 43 (26%) cases. [30] Another Indian report found that in children <12 years of age with ALF, it was possible to determine the aetiology in 35 of 45 patients (77.7%) only, [31] thus making it clear that non-ABCE AVH in all age group is a problem of this region. An earlier report from Japan implicated silent HBV mutants as a major aetiological factor in 90% of non-ABCE cases.[32] But the pathogenic role of occult viral infection in non-ABCE ALF remains controversial. [33] In our series, we did not look for any mutation in PCR studies. Similarly, in cases co-infected with more than one virus no clinical difference is reported when compared to AVH due to a single virus [17] but others opine that mixed HAV and HEV infection usually lead to severe complications in developing countries like India.[34] We had 2% of cases positive for combined viral infection. In AVH, mixed infection of HEV-HAV (5.31%) or HEV-HBV (0.91%) have been occasionally described from India (8) but in children, co-infection may occur in up to 88% of AVH or ALF. [35] In cases with pregnancy, out of 15 cases, the majority (9 cases) was also due to hepatitis A. This, again, is in conflict with available literature reporting Hepatitis E as the commonest cause in pregnancy. Hence, our findings show little dissimilarity from those of other Indian states. The comparison with other studies from India clearly shows how the aetiological profile is different in this part of the country, where HAV is common, in spite of being situated in a relatively underdeveloped part of India where high anti-HAV seroprevalence is expected. The first report of a possible endemic shift of viral hepatitis from the dominance of HEV to HAV in India was reported by Jain P et al from Lucknow. [22] Recently, it was reported from Delhi that out of 500 AVH cases, 80 (16%) were positive for HAV-IgM, signifying acute infection [36]. The authors concluded that since HAV exploits all known mechanisms of genetic variation to survive, including mutation and genetic recombination, larger study from different geographical locations is needed to achieve a logical conclusion about the existence of possible HAV mutations in the Indian population. In a study investigating the molecular epidemiology of hepatitis A virus (HAV) strains over a period of 10 years in western India, co-circulation of and co-infection with subgenotypes IIIA and IB, with predominance of IIIA and genetic heterogeneity of HAV strains were reported by Chitambar et al [37] The hepatotropic viruses are reported to show a cyclic pattern of dominance in endemicity. Thus, North-East India maybe at a junction that is asynchronous with the rest of the country. However, other regions may be following this pattern of HAV overtaking HEV. The serotypes of Hepatitis viruses here may be different. We could not identify any published literature on serotypes from this region. One rationale of HAV predominance may also lie in the unique virus-immune reactions leading to hemolysis or deranged cellular immunity that cause altered susceptibility of the host to infection or the level of viraemia in them [38] Another probable explanation of HAV being the major aetiology in our study is that we may have under-detected Hepatitis E. Chandra et al [23] 0068 ave noted that cases that are ELISA negative for anti HEV antibody may be positive for HEV viraemia by PCR. This can be due to variation that occurs with manufacturer’s lot, and antibodies to different epitopes may differ in persistence. Recently some authors have reported that multiple factors may affect the results of anti-HAV IgM assays, in addition to clinical assessment of the patients and decision to order appropriate tests [39] In AVH in pregnancy group our series does not have sufficient number of patients to come to any conclusion. North East India is a mix of various ethnicities, tribes, cultures, and hence genetic susceptibility. This is matched by the wide variety of infectious organisms found in this region. HEV is comparatively newly reported in the Northeast region with low endemicity. Intake of unknown herbal medications was very common in our series, probably due to cultural beliefs prevalent in this region. ‘Herbs’ are now included in the definition of drug induced liver injury (DILI) and in Asian countries, there are few information regarding the epidemiology and clinical course of DILI, including it’s social burden, morbidity and mortality of patients with such condition. [40] Herb-induced liver injury (HILI) is a less documented condition. In our series, half of all AVH cases took herbal medications and most importantly, it was higher in non-ABCE cases signifying possible hepatotoxic effects of the folk-medications used. Such history of herbal medications was highly significant in the ALF group. However, whether it exacerbates liver damage of AVH or ALF needs to be explored thoroughly. We attribute this to ignorance and socio-cultural beliefs as many of our cases hailed from rural areas. This is a unique finding because no other study has reported an association of herbal/folk medications with AVH or ALF from India till date.
CONCLUSION
This study shows some distinct characteristics of aetiology of AVH in North East India, with a predominance of Hepatitis A over Hepatitis E, that has public health implications. Thus, future research by serotyping and gene sequencing is required in this region to gain more insights into the differences of viral aetiology as compared to the rest of India. The high proportionate mortality in acute hepatitis B is notable. Unknown herbal medications and non-ABCE AVH and ALF are very common in this region, unlike from other parts of India, reflecting the influence of geographical, environmental and socio-cultural differences.
Acknowledgement
The authors are thankful for the immense help received from the scholars whose articles are cited and included in the manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Krugman S. The Gordon Wilson Lecture. The ABC’s of viral hepatitis. Trans Am Clin Climatol Assoc 1992; 103: 145- 156.
2. Acharya SK, Madan K, Dattagupta S, Panda SK.Viral hepatitis in India.Natl Med J India. 2006 Jul-Aug;19(4):203-17.
3. Kumar S, Ratho RK, Chawla YK, Chakraborti A. The incidence of sporadic viral hepatitis in North India: a preliminary study. Hepatobiliary Pancreat Dis Int. 2007;6:596–9.
4. Chadha MS, Walimbe AM, Chobe LP, Arankalle VA. Comparison of aetiology of sporadic acute and fulminant viral hepatitis in hospitalized patients in Pune, India during 1978- 81 and 1994-97. Indian J Gastroenterol. 2003;22:11–5.
5. Das K, Agarwal A, Andrew R, Frösner GG, Kar P. Role of hepatitis E and other hepatotropic virus in aetiology of sporadic acute viral hepatitis: a hospital based study from urban Delhi. Eur J Epidemiol.2000;16:937–40.
6. Jain A, Kar P, Madan K, Das UP, Budhiraja S, Gopalkrishna V, et al. Hepatitis C virus infection in sporadic fulminant viral hepatitis in North India: cause or co-factor. Eur J Gastroenterol Hepatol.1999;11:1231–7.
7. Bansal J, He J, Yarbough PO, Sen S, Constantine NT, Sen D. Hepatitis E virus infection in eastern India. Am J Trop Med Hyg. 1998;59:258–60.
8. Sarguna P, Rao A, Sudha Ramana KN. Outbreak of acute viral hepatitis due to hepatitis E virus in Hyderabad. Indian J Med Microbiol. 2007;25:378–82.
9. Kamath SR, Sathiyasekaran M, Raja TE, Sudha L. Profile of viral hepatitis A in Chennai. Indian Pediatr. Jul 2009;46(7):642-3.
10. Fischer GE, Thompson N, Chaves SS, Bower W, Goldstein S, Armstrong G, et al. The epidemiology of hepatitis A virus infections in four Pacific Island nations, 1995-2008. Trans R Soc Trop Med Hyg. Sep 2009;103(9):906-10.
11. Franco E, Meleleo C, Serino L, Sorbara D, Zaratti L.Hepatitis A: Epidemiology and prevention in developing countries. World J Hepatol. 2012 Mar 27;4(3):68-73.
12. WHO. The Global Prevalence of Hepatitis A Virus Infection and Susceptibility: A Systematic Review. Available from: whqlibdoc.who.int/hq/2010/WHO_IVB_10.01_eng.pdf.
13. Hussain Z, Das BC, Husain SA, Murthy NS, Kar P. Increasing trend of acute hepatitis A in north India: need for identification of high-risk population for vaccination. J Gastroenterol Hepatol. 2006 Apr;21(4):689-93.
14. Das K, Jain A, Gupta S, Kapoor S, Gupta RK, Chakravorty A, Kar P. The changing epidemiological pattern of hepatitis A in an urban population of India: emergence of a trend similar to the European countries. Eur J Epidemiol. 2000 Jun;16(6):507-10
15. Tandon BN, Gandhi BM, Joshi YK. Etiological spectrum of viral hepatitis and prevalence of markers of hepatitis A and B virus infection in north India. Bull World Health Organ 1984;62:67-73.
16. Radhakrishnan S, Raghuraman S, Abraham P, Kurian G, Chandy G, Sridharan G. Prevalence of Enterically transmitted hepatitis viruses in pateints attending a tertiary case hospital in South India. Indian J Pathol Microbiol. 43(4): 433-6; 2000.
17. Kaur R, Gur R, Berry N, Kar P. Aetiology of endemic viral hepatitis in urban North India. Southeast Asian J Trop Med Public Health 2002;33:845-8.
18. Poddar U, Thapa BR, Prasad A, Singh K. Changing spectrum of sporadic acute viral hepatitis in Indian children. J Trop Pediatr 2002;48:210-3.
19. Hussain Z, Das BC, Husain SA, Murthy NS, Kar P. Increasing trend of acute hepatitis A in north India: Need for identification of high-risk population for vaccination. J Gastroenterol Hepatol 2006;21:689-93
20. Kumar S, Rathod RK, Chawla YK, Chakraborti A. The incidence of sporadic viral hepatitis in North India: A preliminary study. Hepatobiliary Pancreat Dis Int 2007;6:596-9
21. Irshad M, Singh S, Ansari MA, Joshi YK. Viral hepatitis in India: A Report from Delhi. Glob J Health Sci 2010;2:96- 103.
22. Jain P, Prakash S, Gupta S, Singh K P, Shrivastava S, Singh D D, Singh J, Jain A. Prevalence of hepatitis A virus, hepatitis B virus, hepatitis C virus, hepatitis D virus and hepatitis E virus as causes of acute viral hepatitis in North India: A hospital based study. Indian J Med Microbiol 2013;31:261- 5
23. Chandra NS, Sharma A, Rai RR, Malhotra B. Contribution of hepatitis E virus in acute sporadic hepatitis in north western India. Indian J Med Res. 2012 September; 136(3): 477–482.
24. Panda SK, Thakral D, Rehman S. Hepatitis E virus. Rev Med Virol. 2007;17:151–80.
25. Arankalle VA, Tsarev SA, Chadha MS, Alling DW, Emerson SU, Banerjee K, et al. Age-specific prevalence of antibodies to hepatitis A and E viruses in Pune, India, 1982 and 1992. J Infect Dis.1995;171:447–50.
26. Acharya SK, Panda SK, Saxena A, Gupta SD. Acute hepatic failure in India: a perspective from the East. J Gastroenterol Hepatol. 2000;15:473–9.
27. Abraham P. Viral hepatitis in India. Clin Lab Med. 2012 Jun;32(2):159-74.
28. Khuroo MS, Kamili S. Aetiology and prognostic factors in acute liver failure in India. J Viral Hepatol. 2003;May10(3): 224-31.
29. Hussain Z, Das BC, Husain SA, Asim M, Chattopadhyay S, Malik A, Poovorawan Y,Theamboonlers A, Kar P. Hepatitis A viral genotypes and clinical relevance: Clinical and molecular characterization of hepatitis A virus isolates from northernIndia. Hepatol Res. 2005 May;32(1):16-24.
30. Abro AH, Abdou AM, Saleh AA, Ustadi AM, Hussaini HS. Hepatitis E: a common cause of acute viral hepatitis. J Pak Med Assoc. 2009 Feb;59(2):92-4.
31. Samanta T, Ganguly SAetiology, clinical profile and prognostic indicators for children withacute liver failure admitted in a teaching hospital in Kolkata. Trop Gastroenterol. 2007 JulSep;28(3):135-9.
32. Uchida T, Shimojima M, Gotoh K, Shikata T, Tanaka E, Kiyosawa K.”Silent” hepatitis B virus mutants are responsible for non-A, non-B, non-C, non-D, non-Ehepatitis. Microbiol Immunol. 1994;38(4):281-5.
33. Ferraz ML, Silva AE, Macdonald GA, Tsarev SA, Di Biscelgie AM, Lucey MR. Fulminant hepatitis in patients undergoing liver transplantation: evidence for a non-A, non-B,nonC, non-D, and non-E syndrome. Liver Transpl Surg. 1996 Jan;2(1):60-6.
34. Arora NK, Nanda SK, Gulati S, Ansari IH, Chawla MK, Gupta SD, Panda SK. Acute viral hepatitis types E, A, and B singly and in combination inacute liver failure in children in north India. J Med Virol. 1996 Mar;48(3):215-21.
35. Kumar A, Yachha SK, Poddar U, Singh U, Aggarwal R. Does co-infection with multiple viruses adversely influence the course and outcome of sporadic acute viral hepatitis in children J Gastroenterol Hepatol. 2006 Oct;21(10):1533-7.
36. Hussain Z, Husain SA, Pasha ST, Anand R, Chand A, Polipalli SK, Rehman S, Kar P. Does mutation of hepatitis A virus exist in North India? Dig Dis Sci. 2008 Feb;53(2):506-10. Epub 2007 Jun 28.
37. Chitambar S, Joshi M, Lole K, Walimbe A, Vaidya S. Cocirculation of and coinfections with hepatitis A virus subgenotypes IIIA and IB in patients from Pune, western India. Hepatol Res. 2007 Feb;37(2):85-93.
38. Hussain Z, Das BC, Husain SA, Polipalli SK, Ahmed T, Begum N, Medhi S, Verghese A, Raish M,Theamboonlers A, Poovorawan Y, Kar P. Virological course of hepatitis A virus as determined by real time RT-PCR: Correlation with biochemical, immunological and genotypic profiles. World J Gastroenterol. 2006 Aug 7;12(29):4683-8.
39. Alatoom A, Ansari MQ, Cuthbert J. Multiple factors contribute to positive results for hepatitis A virus immunoglobulin M antibody Arch Pathol Lab Med. 2013 Jan;137(1):90-5.
40. Ki Tae Suk, Dong Joon Kim Drug-induced liver injury: present and future Clin Mol Hepatol. 2012 September; 18(3): 249–257.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





