IJCRR - 6(20), October, 2014
Pages: 55-60
Print Article
Download XML Download PDF
STUDY OF VARIATIONS IN THE BRANCHING PATTERN OF BRACHIAL ARTERY
Author: Preeti Sonje, Neelesh Kanaskar, Vasanti Arole, Sapna Shevade, Preeti Awari, Vatsalaswamy
Category: Healthcare
Abstract:As the arterial variations are very common, variations in the branching pattern of Brachial artery were studied at D.Y.Patil Medical College, Pune. 50 upper limbs were studied for the variations of Brachial artery. Different types of variations were found. The high origin of Radial artery in 2% of cases, high origin of ulnar artery in 4 % of cases was found. Other type of variation was also seen. These variations are important in different diagnostic as well as surgical procedures. Embryological basis of these variations has also been discussed.
Keywords: Brachial artery, Profunda brachii artery, Radial artery, Ulnar artery
Full Text:
INTRODUCTION
Aim of this study is to study different variations in the branching pattern of brachial artery, which are clinically as well as diagnostically important. 50 upper limbs, embalmed in the formalin, were procured from the department of Anatomy of D. Y. Patil Medical college Pune. Brachial artery is a continuation of Axillary artery at the lower border of teres major muscle. It is the main artery of the upper limb which divides in the cubital fossa into its terminal branches, Radial and Ulnar arteries. Sometimes the Radial artery instead of arising in the cubital fossa, arises at higher level in the upper limb and it is called as high origin of Radial artery which was found in 2% cases unilaterally. Similarly ulnar artery may arise at higher level from the brachial artery which is called as high origin of Ulnar artery. This type of variation was seen in 4% cases, unilaterally. Axillary artery normally gives one branch from the first part i.e. Superior thoracic artery, two branches from the second part i.e. Thoracoacromial and Lateral thoracic arteries and three branches from the third part i.e. Sub scapular , Anterior circumflex humeral and Posterior circumflex humeral arteries . In the present study in 2% cases there was double Posterior circumflex humeral artery one was arising from the third part of Axillary artery and the other was arising from Brachial artery.
MATERIALS AND METHODS
50 formalin fixed upper limbs were procured from the department of Anatomy, Dr D.Y.Patil Medical College Pune. Arm and forearm were dissected by taking incision given in Cunningham’s dissecting manual. After reflection of skin, fascia was cleaned to expose brachial artery and its branches. Incisions were extended both vertically and horizontally whenever necessary. Brachial artery was exposed. It was traced downwards in the upper limb, branching pattern of brachial artery was studied and the variations in its branching pattern were noted and photographed.
RESULT
Different types of variations in the branching pattern of brachial artery were found as follows.
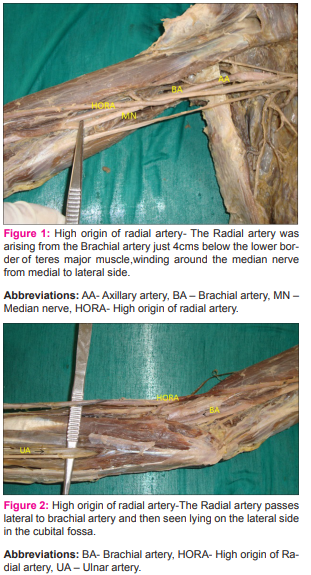
• Presence of unilateral high origin of Radial artery was found in2% of cases.
• The Radial artery was arising from the Brachial artery just 4cms below the lower border of teres major muscle,winding around the median nerve from medial to lateral side to cross superficial to the Median nerve. The artery passed lateral to brachial artery and then was seen lying on the lateral side in the cubital fossa.(fig.1) and ( fig.2)
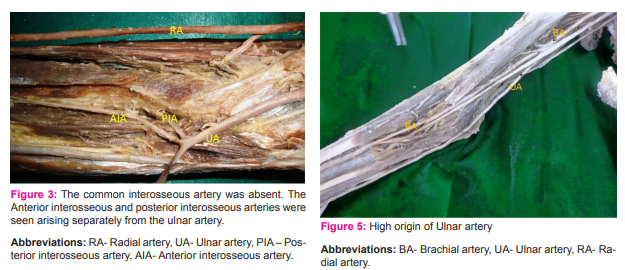
• The common interosseous artery was absent. The Anterior interosseous and posterior interosseous arteries were seen arising separately from the ulnar artery. Inferior ulnar collateral artery was seen arising from the ulnar artery. Superior ulnar collateral artery was arising from the brachial artery. Also both the structures , the median nerve and brachial artery were seen piercing the brachialis muscle.(fig3)
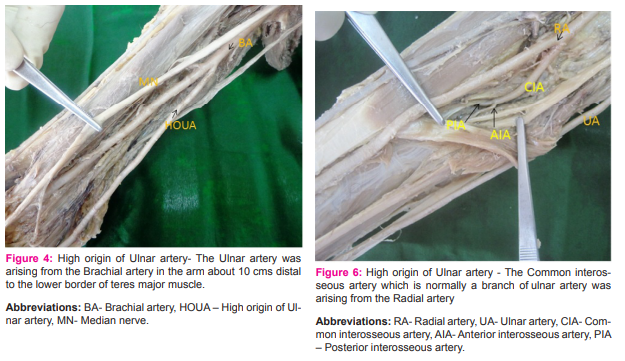
• High origin of ulnar artery was found in 4% of cases
• The Ulnar artery was arising from the Brachial artery in the arm about 10 cms distal to the lower border of teres major muscle .In both the cases the high origin of Ulnar artery was seen unilaterally. (fig.4) and (fig.5)
• The Common interosseous artery which is normally a branch of ulnar artery was seen arising from the Radial artery, while the Ulnar artery had the same course as that of normal ulnar artery in the forearm.(fig.6)
• In 2% of cases there was a common stem for the posterior circumflex humeral artery and Profunda brachii artery.
• Normally the posterior circumflex humeral artery is a branch of third part of axillary artery and the profunda brachii artery is a branch of brachial artery. In our study, there were two posterior circumflex humeral arteries. One posterior circumflex humeral artery was arising as a branch of third part of axillary artery as seen normally but it was very thin, while the other quite thick posterior circumflex humeral artery was arising from the brachial artery as a common trunk with profunda brachii artery. .(fig.7)
• The Superior ulnar collateral artery was seen arising from the Profunda brachii artery instead of arising from the brachial artery (fig.8). This variation was also unilateral.
DISCUSSION
Variations in the branching pattern of brachial artery have been reported by many workers. These variations are important from diagnostic and surgical point of views M. Rodri et al found Brachioradial artery which is defined as a radial artery with a high origin in 39 out of 192 cadavers. Presence of Brachioulnar artery in 13% of cases . This is defined as a high origin of the ulnar artery coexisting in the whole arterial pattern of the limb, with a brachial artery which branches into the radial and common interosseous trunk [1]. John Gourassas presented a case-report of a patient with a failed radial coronary angiography approach, due to the anomalous high origin of the radial artery from the brachial artery [2]. O Okaro et al reported bilateral high origin of radial artery from the Axillary artery [3]. JE Waghmare reported that radial artery was arising from 2nd part of axillary artery [4]. Konstantinos Natsis reported two cases of a uni-lateral high-origin of radial artery with different variations in each case in the course of the artery [5]. Dong Zhan described a brachioradial artery where the radial artery was seen originating from the upper one-third of the brachial artery and continuing distally asthe radial artery in the forearm[6]. Sharmila Bhanu demonstrated high origin and superficial course of Radial artery [7]. Harbans Singh reported an unusual case of bilaterally symmetrical higher bifurcation of brachial artery into radial and ulnar arteries with superficial course of radial artery in right forearm [8]. According to Swaroop. N et al a high origin of radial artery in the left upper limb with superficial course in arm and forearm was found in a male cadaver .The radial artery was originating from the medial side of the brachial artery in the proximal 1/3 rd of the arm. In the cubital fossa a communication was also seen between the radial artery and the Ulnar artery at the level of the neck of radius[9]. Gh. Noditi reported a case presented to the Diagnostic Imaging Centre with peripheral vascular disease of the upper right limb. Using MDCT angiography (64-slice MDCT system; SOMATOM Sensation, Siemens Medical Solutions, Forchheim, Germany) where the patient was found to have a superficial radial artery [10] Venkata Ramana Vollala presented a case of a high origin of the ulnar artery from the brachial artery which was observed during anatomical dissection of a right upper limb This superficial ulnar artery, after running over the bicipital aponeurosis in the cubital fossa was also having a superficial course to the flexor muscles in the forearm and terminated as the superficial palmar arch in the hand [11]. Dr. Sharadkumar Pralhad Sawant observed an unusual branch of the right brachial artery. The brachial artery terminated in the cubital fossa by dividing into radial and common interosseous arteries. The radial artery had normal course and branches. The common interosseous artery was deeper and gave anterior and posterior ulnar recurrent arteries, and then terminated by branching into anterior and posterior interosseous arteries. The unusual large branch from the right brachial artery was a variant of ulnar artery and was seen arising from the lateral side of the brachial artery [12].
Chauhan K et al demonstrated that the superior ulnar collateral artery was seen arising as common trunk with profunda brachii artery in 18 % cases [13]. Dr. Chandrika Teli demonstrated high division of brachial artery into radial and ulnar arteries in the upper third of arm. The posterior circumflex humeral artery, profunda brachii artery and superior ulnar collateral artery all arose from one common trunk in proximal part of brachial artery before its termination. Similar variation was found in the present study in one case [14]. Suat Keskin demonstrated the origin of the ulnar artery from the proximal part of brachial artery. The ulnar artery had a course through the arm and had its normal course in the forearm, forming the palmar arch. In addition, the brachial artery continued as the radial artery, which had a normal course. The common interosseous artery originated from radial artery instead of ulnar artery .This type of variation was also found in the present study in one case [15]. Embryological Explanation: Every anomaly in the peripheral vascular anatomy can be related to genesis as regression or persistence of one or other segment of the embryologic axial artery .The type of anomaly presented in this case is due to persistence of radial artery in the arm and failure of formation of communication between radial and axial arteries in cubital fossa The superficial course of radial artery in upper part of forearm can be explained on the basis of haemodynamic mechanism between deep and superficial arteries in the forearm. Normally due to deep haemodynamic predominance, superficial terminal branches of radial artery undergo developmental arrest and deep part persists as normal radial artery.The superficial radial artery in right upper limb as seen in this case appears to be due to chance variations in haemodynamic factors which leads to regression of deeper vessels and persistence of one of the superficial terminal branches of radial artery. The early limb bud receives blood via inter segmental arteries, which contribute to a primitive capillary plexus. At the tip of the limb bud there is a terminal plexus that is constantly renewed in a distal direction as the limb grows. Later one main vessel supplies the limb and the terminal plexus; it is termed the axis artery.This avascular region contains an extracellular matrix consisting largely of hyaluronic acid. Removal of this hyaluronic acid by hyaluronidase results in vascularization of the tissue since partial degradation products of hyaluronic acid are angiogenic. Thus ectodermal-mesenchymal interactions and extracellular matrix components are controlling the initial patterning of blood vessels within the limb. In the upper limb bud the axis artery is derived from the lateral branch of the seventh intersegmental artery (subclavian). It is pertinentto mention here thatthe normal vascular development including the patterning of the blood vesselsis influenced greatly by local hemodynamic factors. Altered hemodynamic environment may give rise to variant patterning of blood vessels [16]. The developmental reason for the superficial ulnar artery in the present case may be due to the ulnar artery establishing a connection with the axis artery in the arm.
CONCLUSION
Diagnostically these types of variations may disturb the evaluation of angiographic images. Knowledge of such variations has got clinical importance especially in the field of orthopedic, plastic and vascular surgeries [11]. Also knowledge of these different variations is important for the clinicians in day to day practice for measurement of blood pressure using sphygmomanometer cuff in the arm. The knowledge of such variation is important for the diagnostic, interventional and surgical procedures. It may cause misinterpretation of angiographic images. Accidental puncture of superficially placed arteries may occur while attempting venae puncture. Anomalous origin of the radial artery may cause the failure of the radial approach of the coronary angiography and in the reconstructive surgery of the upper limb. When the superficial brachial artery persists it is more vulnerable to the accidental injuries. The superficially located artery increases the risk of heavy bleeding in unexpected situations.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of allthose articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. M. Rodriguez-niedenfuhr1, T.Vazquez 2, L. Nearn 3 , B. erreira1, I. Parkin 4 And J.R. Sanudo (2001) Variations of the arterial pattern in the upper limb revisited: a morphological and statistical study, with a review of the literature. J. Anat. 199, pp. 547–566.
2. J. Gourassas (2003) Anomalous Origin of Right Radial Artery as a Cause of Radial Approach Failure of Coronary Angiography J Cardiol 44: 226-229.
3. O Okaro , B.C. Jiburum (2003) Rare high origin of radial artery : a bilateral symmetrical case. The Nigerian journal of surgical research vol.5 no 1-2 jan.-Junes; page- 70-72.
4. JE Waghmare et al (2009) A high origin of radial artery with asymmetrical vasculature of upper limbs: a case report. Nepal Med Coll J; 11(4): 284-286.
5. Konstantinos Natsis et al (2009) Study of two cases of highorigin radial artery in humans. Eur J Anat, 13 (2): 97-103
6. Dong Zhan et al (2010) High Origin of Radial Arteries: A Report of Two Rare Cases The Scientific World Journal; 10, 1999–2002.
7. Sharmila Bhanu P, Devi Sankar K Susan P (2010) High origin and superficial course of radial artery Case Report .International Journal of Anatomical Variations 3: 162–164.
8. Harbans Singh, Neena Gupta, Bargotra RN, NP. Singh (2010) Higher Bifurcation of Brachial Artery with Superficial Course of Radial Artery in Forearm. JK SCIENCE Vol. 12 No.1, January-March ; page 39-40.
9. Swaroop. N et al (2011) The High Origin of Radial Artery and its Clinical Significance. Anatomica Karnataka, Vol-5, (2) Page 32-35
10. Gh. Noditi et al (2011) Superficial Radial Artery: case report using MDCT angiography.Journal of Experimental Medical & Surgical Research. Pag. 202 – 205.
11. Venkata Ramana Vollala, Raghu Jetti Simmi Soni(2011) High Origin of An Ulnar Artery –Development and Surgical Significance .Chang Gung Med J Vol. 34 No. 6 (Suppl)page 39-42.
12. Sharadkumar Pralhad Sawant , Dr. Shaguphta T. Shaikh , Dr. Rakhi M. More (2012) .Variant Origin and Course of Ulnar Artery. International Journal of Modern Engineering Research (IJMER) available at www.ijmer.com. Vol.2, Issue.6, Nov-Dec. pp-4102-4104.
13. Chauhan K, Udainia A, Bhatt C, Patil D, Patel V and Prajapati B (2013) Morphological study of variations in branching pattern of brachial artery. Internat ional Journal of Basic and Applied Medical Sciences. (Online)Available at http:// www.cibtech.org/jms.htm Vol. 3 (2) May-August, pp.10- 15.
14. Chandrika Teli , Dr. Nilesh N. Kate , Dr. Paarthipan N (2013) High division and variation in brachial artery branching pattern. IOSR Journal of Dental and Medical Sciences available at www.iosrjournals.org. Volume 3, Issue 6 (Jan.- Feb 2013)., PP 68-70
15. Suat Keskin, Zeynep Keskin, M Akif Teber (2013) Common interosseous artery arising from the radial artery and ulnar artery origin from proximal brachial artery -case Report. Eur J Gen Med; 10 (Suppl 1):36-38.
16. Keith L.Moore, T.V.N. Persaud.The developing human – Clinically oriented embryology.Elsevier publications, 2008, 8th edition page no 371-374.

Abbreviations:
BA- Brachial artery, CT- Common trunk, PCHA- Posterior circumflex humeral artery ,PBA- Profunda brachii artery, RN – Radial nerve, SUCA – Superior ulnar collateral artery, UN – Ulnar nerve.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





