IJCRR - 6(22), November, 2014
Pages: 11-14
Date of Publication: 21-Nov-2014
Print Article
Download XML Download PDF
Autopsy Study of Brought Dead Cases in Jaipur, Rajasthan
Author: N. L. Disania, Akhilesh K. Pathak, R. K. Punia
Category: Healthcare
Abstract:Background: Most of the medico-legal cases are dealt by the government hospitals in India. Incidences of brought dead cases are higher in Sawai Man Singh Hospital, Jaipur, due to high referral rate from all areas of Rajasthan as well as from the nearby border. In all cases, who are found dead clinically on arrival examining doctor is not able to opine cause of death and hence the dead body has to be shifted for autopsy examination. Aims and Objective: There is very little information available regarding the cases of brought dead. The present study was undertaken to know the epidemiological aspects, patterns and other significant medico-legal issues regarding the brought dead cases. Method: This autopsy based retrospective study was conducted in the department of Forensic Medicine, S.M.S. Medical College, Jaipur (Rajasthan). Around 3123 autopsies were conducted during the one year period of 2012 and out of them 990
(31.70%) cases, which were brought dead to the casualty department were analyzed during this study irrespective of age, gender, religion and area of domicile. The results: In the present study, we found that the majority of the victims who were brought dead to us were Hindu males, in their 3rd and 4th decade of life that died accidentally in road traffic accident. Conclusion: Our study reveals that the cases of brought dead were included more incidences of unnatural deaths rather than the natural deaths, which are having less medico-legal significance and more suffering to relatives of the deceased as well as the investigating agencies.
Keywords: Death, Brought dead and Cause of death
Full Text:
INTRODUCTION
Brought dead or received dead (brought in dead) is a condition where the patient is found dead clinically by the examining medical person. In these cases the patient was alive before some time, but on arrival in hospital no signs of life are present. Determination of death and its various medico-legal issues are discussed by various authors. (1, 2, 3, 4) Now it is essential that the cause of death and the identity of the deceased be properly determined before lawful disposal of the dead body and it also helps to collect data regarding death. From 1 April 1969, under the Registration of Births and Deaths Act, the registration of births and deaths is now compulsory throughout India. For this purpose, whenever necessary by law, it is obligatory for a medical practitioner who last attended the deceased person, to issue a death certificate, after inspecting the body and satisfying himself of the person’s death, stating the underlying cause of death- that is the morbid condition or disease process, or abnormality leading directly or indirectly to death. (5) The incidences of brought dead cases are increasing day by day in the casualty department of S.M.S. Hospital, Jaipur because of high referral rates from the peripheral health centers and involvement of fatal natural and unnatural events. In most of the cases of brought dead, the patients are either referred from a lower health center for further management or brought by the police or relatives in the presumption of life or to confirm the death. There is very little information available regarding the cases of brought dead as only few studies has been conducted before this, and hence the present study was undertaken to know the epidemiological aspects, patterns and other significant medico-legal issues regarding the brought dead cases.
Material and Methods:
The present retrospective study was conducted in the department of Forensic Medicine, S.M.S. Hospital, Jaipur in which is a tertiary health center of Rajasthan. Here the cases are referred from almost all areas of Rajasthan as well as from the border areas of nearby state like Uttar Pradesh and Haryana. Around 3123 autopsies were conducted during the one year period of 2012 and out of them 990 (31.70%) cases, which were brought dead to the casualty department were selected for the present study. All cases who were found dead clinically on arrival in casualty irrespective of age, gender, religion and area of domicile were taken into consideration and detailed and complete post mortem examination was conducted to know the exact cause of death. Information regarding the scene of crime and history was collected from the relatives and concerning police person and the detailed autopsy report findings were taken into consideration to conclude the manner of death whether it was suicidal, accidental or homicidal in nature. Finally the data were collected and analyzed at medical college, Baroda, Gujarat and compared with data of other authors.
Results
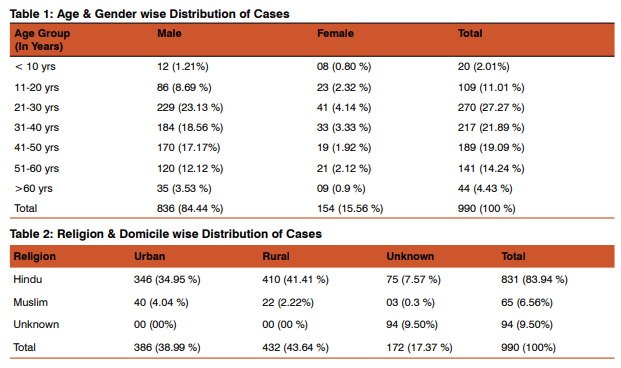
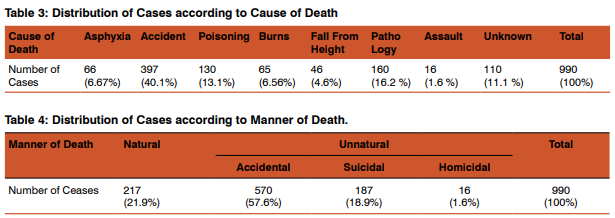
Out of total 3123 autopsies, 990 cases (31.70%), which were brought dead to the casualty department, were selected for the present study. The maximum incidences of brought dead cases were included victims in their 3rd decade (27.27%) of life followed by the victims in their 4th decade (21.89%) of life as compared to both extremes of age. The majority of the victims (68.25%) who were brought dead were belonging to the adult age group of 21-50 years. When brought dead cases were analyzed in contrast to their gender, then we found that the incidence of male victims (84.44%) was found 5.43 times higher than the female victims with a male to female ratio of 1: 0.18. Distribution by brought dead cases according to their religion and domicile shows that incidences were higher in Hindu people (83.94 %) as compared to Muslims (6.56%). There was not much difference in the incidence of the victims who were brought dead to us from urban (38.99 %) and rural (43.64 %) areas. We could not determine the religion in 9.5% cases, while the domicile of victims were not known in 17.37% cases. In the present study, analysis of brought dead cases, according to the cause of death shows that the highest number (40.1%) of the victims who were brought dead died due to accident including vehicular and railway accidents followed by pathology (16.2%) of some organs. In 11.1% cases we could not determine the cause of death after all efforts till the date of this study. The distribution of cases, according to the manner of death shows that in most of the victims who were brought dead to us, the manner of death was accidental (57.6%) in nature followed by suicidal cases (18.9%) and homicidal cases (1.6%). When the cases were analyzed in contrast to natural and unnatural means, then we found that the incidences of unnatural deaths (78.1%) were more as compared to natural deaths (21.9%).
Discussion
Death is permanent and irreversible stoppage of the all three vital systems of the body, including the circulatory, respiratory and neurological systems and in these cases a doctor is having a duty to pronounce the death and issue a certificate ascertaining the cause of death. Declaration of death is a tedious job to the doctor because he has to confirm by all means that the stoppage of vital functions is irreversible and permanent and on the other hand the doctor also has to inform the relatives about this shocking and painful news. But in the cases of brought dead the medical person who is attending the case first time in casualty department is not able to conclude the cause of death and hence the dead body is shifted to mortuary for the post-mortem examination to certify the cause of death. In the present study, we have analyzed the cases that were found dead clinically on arrival in casualty department and the results were compared with data of other researchers. The incidence of bringing dead cases in the present study was 31.7%. In our study majority of the victims (27.27%) were in their 3rd decade of life followed by the victims in their 4th decade (21.89%) of life, which is consistent with the findings of Tripude et al(6) while the Gupta et al found higher incidences in their study in 3rd-5th decade of life, which is probably due to different criteria of inclusion of the cases.(7) Most of the victims in our study were Hindu, males that are similar with the observations of other authors.(7,8) On analysis of cases according to their domicile we did not find much difference in the incidence of the victims who were brought dead to us from urban (38.99 %) and rural (43.64 %) areas. Even after all efforts, we could not find out the religion in 9.5% cases, while the domicile of victims could not be determined in 17.37% cases. In the present study majority of the victim who were received dead, died due to traumatic injury occurred in Road Traffic Accident (RTA) and railway accident, followed by pathology of any organs in the body, which is quite similar with the observations of others in their study. (6) The higher incidences in younger age groups are likely referable to the inclusion of the cases of trauma. In present study information from relatives and accompanying police records with autopsy details were used to conclude the manner of death and we found that the incidences of unnatural deaths (78.1%) were more as compared to natural deaths (21.9%), which is a common phenomenon of most of the autopsy studies.(6,8,9) In un-natural deaths majority of the victims died due to traumatic injury caused by accident in 57.6% cases, followed by suicidal deaths in 18.9% cases and homicidal deaths in 1.6% cases.
Conclusion
The pattern of cases of brought dead in present study is nearly alike to the other studies conducted at other centers. Our study revealed that most of the victims who were brought dead to us belonging to the Hindu males of the younger age group who died due to accidental trauma. The hospital administration should lead an initiative to smoothen the medico-legal issues linked to cases of received dead in casualty so the relatives who are already broken mentally do not suffer more. Finally more researches on this as well as other centers are required for better understanding the pattern of these cases and their different medico-legal issues.
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to Authors/Editors/Publishers of all those articles, journal and books from where the literature of this article has been reviewed and discussed.
References:
1. Reddy KSN and Murty OP: The Essentials of Forensic Medicine and Toxicology, 32nd Edition, K Sugnadevi, Hyderabad, 2013; 130-32.
2. Nandi A: Principles of Forensic medicine including Toxicology, 3rd Edition, New Central Book agency Pvt. Ltd., Kolkata, 2010; 221-26.
3. Vij K: Textbook of Forensic medicine and Toxicology, 5th Edition, Elsevier, 2011; 74-75.
4. Biswas G: Review of Forensic medicine and Toxicology, 2nd Edition, Jaypee brothers medical publishers, 2012; 107- 110.
5. Modi JP, Edited by Kannan K and Mathiharan K: A Textbook of Medical Jurisprudence and Toxicology, 24th Edition, Laxis Naxis Butterworth Wadhwa, Nagpur, 2012; 200-201.
6. Tripude B, Nagrale N, Murkey P, Zopate P and Patond S: medico legal profile of brought dead cases received at mortuary, J of Forensic Med, Sci and Law, 2012; Vol.21 (2): 1-8.
7. Gupta BD, Vaghela PC, Singh G and Mehta R: futility of post-mortem examination in ‘brought in dead’ cases: A retrospective study, JPAFMT, 2006; Vol.6, 9-10.
8. Chaturvedi M, Satoskar M, Khare MS and Kalgutkar AD: Sudden, unexpected and natural death in young adults of age between 18 years and 35 years: A clinic-pathological study, Ind J of Patho and Micro, 2011; Vol. 54(1): 47-50.
9. Bansal AK, Patel AP, Mittal P, Bhoot RR, Merchant SP and Patel PR: Pattern of spot death cases brought to V.S. General Hospital, Ahmedabad: A retrospective study, JIAFM, 2013; Vol.35(2): 131.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





