IJCRR - 6(23), December, 2014
Pages: 44-48
Date of Publication: 10-Dec-2014
Print Article
Download XML Download PDF
FREQUENCY OF PLACENTA PREVIA IN MULTIGRAVIDA AT TERTIARY CARE HOSPITAL
Author: Shahida Shaikh
Category: Healthcare
Abstract:Background: Placenta previa is a localization of placenta in the lower uterine segment, near or over the internal os. Multigravida is one of the risk factors of placenta previa. The aim of study is to look for current frequency of placenta previa in multigravida, so that further improvement in diagnosis and treatment modalities can be made in order to decrease the morbidity and mortality related to it in this group. Objective: To determine the frequency of various grades of placenta previa in multigravida at a tertiary care centerMethodology: This is a cross sectional study conducted from 28th December 2012 to 27th June 2013 at the department of Gynecology and Obstetrics, Sheikh Zaid Women, Chandka Medical College Hospital, Larkana Sindh Pakistan. A total of 208 patients enrolled in the study with non -probability purposive sampling technique. All pregnant women with singleton pregnancy of 25-35 years of age in their second or more pregnancy with gestational age ? 34 weeks were included. Exclusion criteria observed for patients with multifetal pregnancy, previous history of cesarean section, dilatation and curettage, cervical cone biopsy, myomectomy or any pelvic surgery. All pregnant women had trans-abdominal ultrasound. The presence or absence of placenta previa was reported by an experienced sonologist. The data was analyzed using SPSS version 12. Results: Among the total recruited patients, mean age of these multigravidas was 30.1\?5.6 years. The mean parity of our population was 4.02\?1.2. The gestational age noted was 38\?1.4 weeks as mean. Median Body mass index (BMI) of registered participants was 28.40\?5.9. The frequency of placenta previa was 13 (6.3%) and type IV was the most common type.
Conclusion: It is concluded from this study that the frequency of placenta previa in patients of multigravida was 6.3% and apartfrom other risk factors, multigravidity is an independent risk factor for placenta previa.
Keywords: Placenta previa, Multigravida, Age, Body mass index
Full Text:
INTRODUCTION
Placenta previa is in fact localization of placenta in the lower uterine segment, over or near the internal os, which is not a normal site of placental attachment.1 It undertakes clinical significance due to its adherent risk of maternal and perinatal morbidity and mortality. The frequency of placenta previa is reported as 3-5 per 1000 pregnancies and it is globally and statistically mounting due to swelling risk factors.2 In Pakistan prevalence is 3.5%,whereas this figure surges to 65% in mothers having history of previous caesarean section.3 The predisposition for occurrence of placenta previa is observed more in past era chiefly because of higher caesarean section rate and unconventionally late maternal age at conception4 .Even though origination of placenta previa stagnantly remains ambiguous, but multiple threatening elements can reveal its happening embracing Caesarean Section, high parity, increasing age and previous abortions.5 Life style of women also plays its role, likewise if mother is having history of smoking and cocaine during pregnancy ,these too have been seen escalating the possibility of placenta previa.6 Observation is that, there occurs a defect in endometrial lining causing its atrophy due to previous scarring or inflammation in the endometrium, ensuing in unusually low implantation of the placenta at the level of internal uterine os with ample blood supply.7 There are 4 grades of placenta previa. All the grades of placenta previa can cause painless vaginal bleeding during second or third trimester at any time, that further may result in postpartum hemorrhage, air embolism and ascending infection compromising maternal status and maternal mortality, fetal growth retardation, congenital malformation, fetal anemia, malpresentation and un expected fetal death.8,9 Multiparty has been considered as an important risk factor for placenta previa. These women are prone to have sixteen times more chances of placenta previa as compared to nullipara.10, Maternal and fetal mortality can be reduced by identifying the high risk patients and educating them for care about next pregnancy.11 For the diagnosis of placenta previa, although trans vaginal ultrasound is gold standard but trans-abdominal is also having75% accuracy in identification.12 The overall prevalence of placenta previa in setup like ours is 3.5%. 11 Though lots of studies have been done on placenta previa, but studies specifically on placenta previa in multigravida are scarce in Pakistan, as well as internationally. Aim of our study is to look for current frequency of placenta previa in multigravida in order to have further improvement in the diagnosis and treatment modalities, hence to decrease the morbidity and mortality related to it.
SUBJECTS AND METHOD
This cross sectional study was conducted at the department of Gynecology and Obstetrics, Sheikh Zaid Women Hospital Chandka Medical College , Larkana Sindh province of Pakistan during the period from 28th December 2012 to 27th June 2013 after taking formal approval from institutional ethical committee.The sample size obtained with non -probability purposive technique calculated by using World Health Organization sample size determination software with 95% confidence interval, 2.5% level of precision considering the prevalence of placenta previa as 3.5%.11 Accordingly we enrolled 208 patients in this study, after fulfilling following selection criteria as follows
INCLUSION CRITERIA
• All pregnant women of 25-35 years of age in their second or more pregnancy.
• Gestational age ≥ 34 weeks.(ultrasound based)
EXCLUSION CRITERIA
• Previous history of cesarean section (CS).
• Past history of dilatation and curettage (D and C).
• History of cervical cone biopsy.
• History of myomectomy or other any pelvic surgery.
• Multifetal pregnancy
The data was collected after explaining the study protocol and informed written consent. This was an observational study so no women denied. Confidentiality regarding patients’ medical and nonmedical details was maintained. All possible effect modifying variable as parity, maternal age, gestation age, and body mass index (BMI) was noted. All pregnant women underwent trans-abdominal ultrasound. Trans-vaginal ultrasound experts are available at our institute but patients usually refuse due to social constraints so we did not offer them. The presence or absence of placenta previa was reported by an experienced sonologist with 8 years’ experience in relevant field. All the collected data was transferred to predesigned Performa and analysis of data done through SPSS version 12.
RESULTS
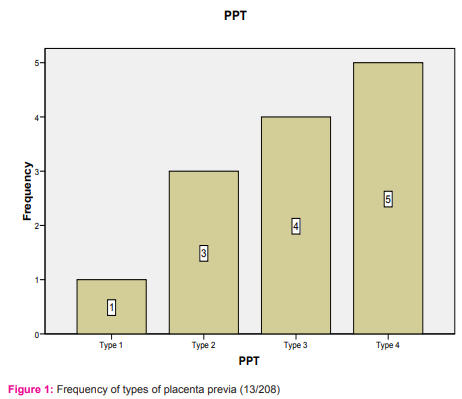
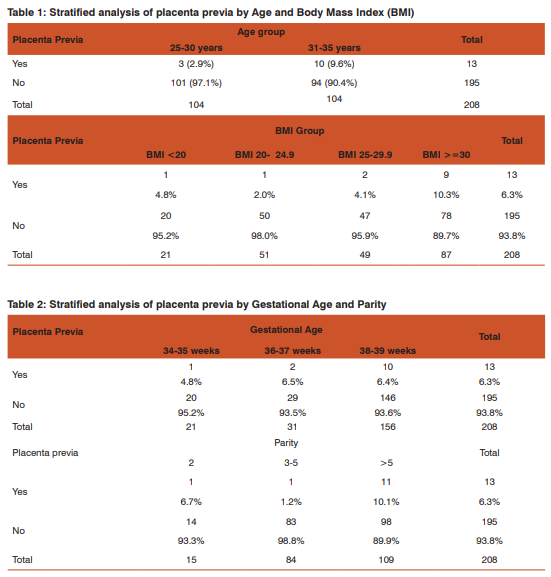
A total of 208 patients were enrolled in this study during six months period. The age assortment of women considered was from 25 to 35 years. Equal number of patients was found to be in group of 25-30 years 104 women (50%) and same figure of 104 in 31-35 year as well. Therefore their mean age was 30.1±5.6 years. We had included patients more than 34 weeks, so there were majority of patients (156/208) at 38 -39 weeks of gestation with mean gestational age was 38±1.4 weeks. The important figure of exploration was parity Thus 52% patient had parity beyond 5 and mean parity was 4.02±1.2 ranging from 1 to 5. The number of multigravida women who had placenta previa was 13 and that made 6.3% of frequency at our setup. The type IV placenta previa was the most common type; further distribution shown in figure 1 Stratified analysis of placenta previa based on age, body mass index, is summarized in table I Among 156 patients having gestational age 38-39 weeks, 10 (6.4%) had placenta previa as compared to 1 (4.8%) woman in the group of patients with gestational age 34- 35 weeks. Of 109 patients of parity >5, we had 11 women with (10.1%) making 84% of total (11/13) patients with placenta previa compared to 1 woman (6.7%) in group of primiparity. Break up is also shown in table II.
DISCUSSION
Hemorrhage in pregnancy is still the commonest cause of maternal deaths in the parts of world with low incomes.13Placeta previa in symptomatic women may cause some times furious bleeding risking both mother and baby. Advancing maternal age is a recognized hazardous issue for abnormally situated placenta. It has been established that women at or beyond 35 years of age are vulnerable population to have placenta previa.14 The pathophysiology, how advanced maternal age impedes normal placental expansion is not well agreed. The potential description is, that the proportion of sclerotic changes on intramyometrial arteries escalates with increasing age, thus plummeting blood supply to placenta.15 In our study also, we have observed that higher maternal age is a risk factor of placenta previa (PP). We found that in women of 31-35 years of age, the frequency of placenta previa was 9.6% compared to 25-30 years of age, where the frequency of placenta previa was 2.9%. This difference has likewise been noticed by study involving two centers of Sindh province and others as well.16, 17 We found in our results, the frequency of placenta previa in patients with body mass index (BMI) >30 was 10.3% in comparison to 4.8% patients with body mass index 5 the frequency of placenta previa(PP) was 10.1% compared to 6.7% in primiparous. It makes 84% of total (11/13) women having placenta previa (PP). The difference of proportion of said condition between two groups is quite significant. These observations are also instituted in studies conducted in national and international levels as well, where reportedly 60% of their patients of placenta previa were multiparous.4, 22 Another author has similar findings in her study sharing same social scenario of highest turnover of those women who never practice contraception and end up in complicated pregnancy with placenta previa.2 In one other study, 23 it was concluded that the women having less parity halves the chances of Placenta Previa than those with or higher than 3 and identical with findings of our study.
CONCLUSION
The finding of this study highlights that apart from other complications in multiparous women, placenta previa also poses a great threat to mother as an independent risk. Antenatal diagnosis of Placenta previa may help in planning mode of delivery and saving fetomaternal lives. Being part of low resource setting, we must emphasize on capacity building to have emergency obstetric services available to mothers everywhere.
ACKNOWLEDGEMENT
Author acknowledges the enormous help received from the scholars whose articles have been cited and incorporated in references. Author is also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of funding: None Conflict of interest: None declared
References:
1. Raheel R, Tabassum R, Bhutto A, Riaz H, Hanif R. Fetal outcome in the cases of placenta previa – A retrospective study. Medical Channel 2010; 16(2):256-59.
2. Khursheed F, Shaikh F, Das CM, Shaikh RB. Placenta previa: an analysis of risk factors. Medical Channel 2010; 16(3):417-9.
3. Tabassum R, Raheel R, Bhutto A, Riaz H, Hanif F. The risk factor associated with placenta previa in patients presented to civil hospital Karachi- a case report control study. Medical Channel 2010; 16(2):276-9.
4. Shoukat A, Zafar F, Asghar S, Nighat, Ayoub A, Ambreen N, et al. Frequency of placenta previa with previous Csection:[internet].2011.Available from: http:/pjmhsonline. com/frequency_of_placenta_previa_wit.htm.
5. Hung TH, Hsieh CC, Hsu JJ, Chiu TH, Lo LM, Hsieh TT. Risk factors for placenta previa in an Asian population. International Journal of Gynecology and Obstetrics 2007; 97,26–30
6. Handler AS, Mason ED, Rosenberg DL, Davis FG. The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol1994; 170:884-9.
7. Oya A, Nakai A, Miyake H, Kawabata I, Takeshita T. Risk factors for peripartum blood transfusion in women with placenta previa: a retrospective analysis. J Nippon Med Sch. 2008; 75 (3):146-51.
8. Kean L. antepartum haemorrhage. In: Luesley DM, Baker PN.Editors Obstetrics and Gynecology. Evidence-based Text Book for MRCOG. London: Arnold Publishers; 2004: 302- 16.
9. Narti OB, Konje JC. Bleeding in late pregnancy. In: James DK Steer, Weiner CP, Gonik B, Crowther C, Robson SC, editors. High risk of pregnancy, management option. London; Elsevier. 2011:1037-52.
10. Malik AM, Siddique S, Shah IA. Placeta previa: a study to determine responsible factors. Professional Med J. 2007; 14 (3):407-10.
11. Nasreen F. Incidence causes an outcome of placenta previa. J Postgrad Med Inst. 2003; 17(1):99-104.
12. Oppenheimer L, Society of Obstetricians and Gynaecologists of Canada. Diagnosis and management of placenta previa. J Obstet Gynaecol Can 2007; 29:261.
13. Obstetrics hemorrhage. In: Cunningham FG, Leveno KJ, Bloom SL, Hauth JP, Rouse DJ, Spong Cy, editors. Williams Obstetrics. 23rd Ed. New York: The McGraw-Hill Companies 2010: 757-803.
14. Ananth CV, Wilcox AJ, Savitz DA, Bowes WA Jr, Luther ER .Effect of maternal age and parity on the risk of uteroplacental bleeding disorders in pregnancy.ObstetGynecol 1996; 511-6.
15. Zhang J, Savitz DA. Maternal age and placenta previa: a population-based, case-control study. Am J ObstetGynecol 1993;168:641-5
16. Memon S, Kumari K, Yasmin H, Bhutta S. Is it possible to reduce rates of placenta previa. Journal of the Pakistan Medical Association 2010; 60(7): 566-9.
17. Cleary-Goldman J, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock CH, et al. Impact of Maternal Age on Obstetric Outcome. Obstet Gynecol 2005; 105:983-90.
18. Tosson, Madiha M, Tarek K. AL-Hussaini.The impact of maternal obesity on pregnancy outcome at Assiut University hospital. Ass. Univ. Bull. Environ Res 2005; 8(2) :1-11
19. Choden P, Bhutia,Lertbunnaphong T, Wongwananuruk T, Boriboonhirunsarn D. Prevalence of Pregnancy with Placenta Previa in Siriraj Hospital. Siriraj Med J 2011; 63(6):191-5.
20. Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and meta-analysis of observational studies. J Maternal Fetal Neonatal Med 2003; 13:175.
21. Ojha N. Obstetric factors and pregnancy outcome in placenta previa. Journal of Institute of Medicine 2012; 34: 38-41.
22. Mgaya et al. Grand multiparity: is it still a risk in pregnancy? BMC Pregnancy and Childbirth 2013; 13:241.
23. Tuzoviæ L, Djelmiš J Ilijiæ M. Obstetric Risk Factors Associated with Placenta Previa Development: Case-Control Study Croat Med J 2003;44:728-733
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





