IJCRR - 6(23), December, 2014
Pages: 19-22
Date of Publication: 10-Dec-2014
Print Article
Download XML Download PDF
A STUDY ON THE PREVALENCE AND ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF METHICILLIN RESISTANT STAPHYLOCOCCUS AUREUS IN A SOUTH INDIAN TERTIARY CARE HOSPITAL
Author: A. Heraman Singh, S. Aruna
Category: Healthcare
Abstract:Context: Methicillin Resistant Staphylococcus aureus (MRSA) prevalence is increasing worldwide and it remains as a major cause of morbidity and mortality in hospitalised patients due to its versatile behaviour towards antibiotics.
Aims: This study was done to find out the prevalence and antimicrobial susceptibility pattern of MRSA isolates at our hospital setup, in order to guide policy on the appropriate use of antibiotics. Settings and Design: The study was a prospective observational study, carried out in the Department of Microbiology, GSL Medical College, Rajahmundry, Andhra Pradesh. Methods and Material: A total number of 288 strains of Staphylococcus aureus were isolated from various clinical samples received in the laboratory. Staphylococcus aureus was identified by routine standard operative procedures. Antimicrobial susceptibility testing was done by Kirby-Bauer disc diffusion method and the results were interpreted following Clinical Laboratory Standards Institute (CLSI) guidelines. Methicillin resistance was screened by using oxacillin disks [1 mcg]. Statistical analysis used: Data obtained was analysed and presented in counts and percentages. 95 % confidence interval values were also calculated. Results: Methicillin resistance was documented in 120 [41.6%] Staphylococcus aureus isolates. Most of them were isolated from pus, wound swabs, urine and respiratory samples. All MRSA isolates were resistant to penicillin and cefepime. The resistance was high to tetracycline, erythromycin, co-trimoxazole piperacillin / tazobactam, and ciprofloxacin; moderate to aminoglycosides, clindamycin, chloramphenicol and levofloxacin. All MRSA strains were susceptible to vancomycin. Overall, 63.3% [76/120] of MRSA strains were found to be resistant to more than 6 antimicrobials tested. Conclusions: Our study emphasizes the need for regular surveillance and formulation of a strict drug policy on the appropriate use of antibiotics to control MRSA infections. This would also minimise the irrational use of vancomycin and the emergence of vancomycin resistant Staphylococcus aureus [VRSA].
Keywords: MRSA, Vancomycin, Antimicrobial susceptibility pattern
Full Text:
INTRODUCTION
The isolation of methicillin resistant Staphylococcus aureus [MRSA] was reported within one year of introduction of methicillin. Since then, the prevalence of MRSA has increased steadily. In the past 10 years, numerous outbreaks of infections caused by MRSA have been reported 1 . In many hospitals, 40 – 50 % of Staphylococcus aureus isolates are now resistant to methicillin1, 2. MRSA isolates are important for their resistance to many commonly used antibiotics. They exhibit remarkable versatility in their behaviour towards antibiotics which poses a serious therapeutic problem. Thus, MRSA remains as a major cause of morbidity and mortality among hospitalised patients despite the availability of numerous effective anti-staphylococcal antibiotics. This emphasizes the need to study the prevalence and antimicrobial susceptibility pattern of MRSA isolates area-wise in order to guide policy on the appropriate use of antibiotics which would minimise the irrational use of vancomycin and so the emergence of resistance to vancomycin. The present study was carried out to find out the prevalence and antimicrobial susceptibility pattern of MRSA isolates at our hospital set up. The information would also be useful in contributing data to larger more extensive surveillance programs.
SUBJECTS AND METHODS
The present study was conducted in the Department of Microbiology, GSL Medical College and General hospital, Rajahmundry, Andhra Pradesh. A total number of 288 strains of Staphylococcus aureus were isolated from various clinical samples received in the laboratory during the period June 2011 to December 2012. Ethical clearance was obtained from the institute. Standard procedures were followed to isolate the organisms from the clinical samples. Staphylococcus aureus was identified by Gram stain morphology, colony characters on blood agar, biochemical reactions like catalase test, mannitol fermentation, slide coagulase test and tube coagulase test3 . All the Staphylococcus aureus strains were then subjected to antimicrobial susceptibility testing by Kirby-Bauer disc diffusion method and the results were interpreted following CLSI guidelines4 . Methicillin resistance was screened by using oxacillin disks [1 mcg]. Anti-staphylococcal antibiotics like penicillin G [10 units], cefepime [30mcg], ciprofloxacin [5 mcg], levofloxacin [5 mcg], erythromycin [15 mcg], tetracycline [30 mcg], chloramphenicol [30 mcg], co-trimoxazole [1.25/23.75 mcg], piperacillin/tazobactam [100/10 mcg], clindamycin [2 mcg], gentamicin [10 mcg], amikacin [30 mcg], tobramycin [10 mcg] and vancomycin [30 mcg] were tested (Himedia, Mumbai, India ). The data obtained in this study was summarized by counts and percentages. Antimicrobial Susceptibility rates were also presented in 95% confidence interval values.
RESULTS
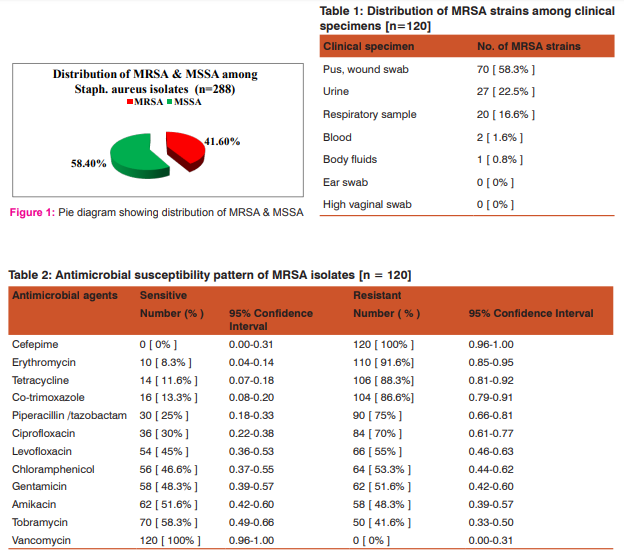
A total number of 288 strains of Staphylococcus aureus were isolated from different clinical samples obtained from inpatients of the hospital. Methicillin resistance was documented in 120 [41.6%] Staphylococcus aureus isolates (Figure 1). Majority of the MRSA strains were isolated from pus and wound samples [58.3%], followed by urine [22.5%], respiratory specimens [16.6%], blood [1.6%] and body fluids [0.8%] (Table 1). All MRSA isolates were resistant to penicillin and cefepime. Resistance was high to tetracycline, erythromycin, cotrimoxazole, piperacillin/tazobactam, and ciprofloxacin; moderate to aminoglycosides, levofloxacin, clindamycin and chloramphenicol. All MRSA strains isolated in the present study were susceptible to vancomycin (Table 2).
DISCUSSION
MRSA prevalence is increasing worldwide and has become a serious public health issue. The MRSA prevalence rate shows significant regional variance5, 6, 7. In the present study, the prevalence rate of MRSA was found to be 41.66 %. This was higher when compared to various studies reported from India, ranging from 29.1% to 34.78% 8, 9, 10 and abroad, ranging from 9 % to 26.9%5, 11, 12, 13, 14. However, it was comparable to the prevalence rates reported from Varanasi (38.44%), Chennai (45%), Amritsar (46%) and Visakhapatnam (45%) 6, 15, 16, 17. In contrast, studies from Indore (80.89%) and Pakistan (83%) reported much higher prevalence rates of MRSA7, 18. This variation in prevalence rates in different places could be due to differential clonal expansion and drug pressure in the community 6 . MRSA are often multidrug resistant and studies have indicated that there has been progressive increase in the development of resistance to several antibiotics6, 8, 9. In our study, 63.3% [76/120] of MRSA isolates were found to be resistant to more than 6 antimicrobials tested. A study from Varanasi reported that prevalence of multidrug resistant MRSA is high in India and without MRSA surveillance and strict drug policy, the threat would increase 6 . The antimicrobial susceptibility pattern of MRSA isolates varies with place and time5 . Ciprofloxacin has been considered as a potent antibiotic in the therapy of MRSA infections and therefore it is widely used on empirical basis. This resulted in a steady increase of resistance to ciprofloxacin among MRSA isolates 11. Many studies have reported high resistance rates to ciprofloxacin among MRSA isolates ranging from 75.7 % to 88.2 % 6, 8, 13, 16. In the present study it was found to be 70 %. However, this was higher when compared to other studies reported from Eritrea ( 8 % ), Mangalore ( 31.8 % ) and Kano ( 43.7 % ) 5, 9,12 . High resistance was observed in this study among MRSA isolates to antibiotics like co-trimoxazole (86.6%), tetracycline (88.3%), and erythromycin (91.6%). This was indicated in different studies reported from India and abroad 6, 9, 12, 13, 16. In contrast, low resistance was found in Eritrea to erythromycin (27%) and co-trimoxazole (23%) 5. The emergence of high resistance could be due to excessive use and over the counter availability of these antibiotics in the developing world for the treatment of staphylococcal and many other infections both in man and animals6, 11. All MRSA isolates were found to be resistant to penicillin (100%) and cefepime (100%). Interestingly, the resistance to piperacillin and tazobactam combination (75%) was high even though it was not a commonly used antibiotic at our hospital setup. Vancomycin was found to be the most effective antibiotic against MRSA isolates in our study, with a susceptibility rate of 100%. This was in line with the observations made in various studies from India and abroad 9, 12,13,16,17. However, it is quite expensive, toxic and not easily available for regular use and therefore may be reserved for treating life threatening MRSA infections6, 7, 9. In our study MRSA isolates showed moderate resistance rates to gentamicin [51.6%], amikacin [48.3%] tobramycin [41.6%], chloramphenicol [53.3%], clindamycin [53.3%] and levofloxacin [55%] compared to other antibiotics tested. These antibiotics may be tried as an alternative to vancomycin after antimicrobial susceptibility testing is done. This would prevent the emergence of vancomycin resistant Staphylococcus aureus [VRSA] 6, 7, 9 .
CONCLUSION
MRSA is a common pathogen at our hospital setup and vancomycin is still the drug of choice. The presence of high percentage of multidrug resistant MRSA is a serious matter of concern. Therefore, regular surveillance and formulation of a strict drug policy on the appropriate use of antibiotics are very much essential in the control of MRSA infections and to avoid the emergence of VRSA. Regular monitoring on quality, availability and the use of antibiotics also helps in preserving the effectiveness of antibiotics.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of funding: None Conflict of interest: None Declared
References:
1. Fauci, Brawnwald, Kasper, Hauser, Longo, Jameson et al. Harrison’s Principles of Internal Medicine; 17th edition. 2008; vol 1; 879.
2. Shiv Sekhar Chatterjee, Pallab Ray, Arun Aggarwal, Anindita das and Meera Sharma. Acommunity-based study on nasal carriage of Staphylococcus aureus. Indian J Med Res 130, December 2009, pp 742-748.
3. Collee JG, Fraser AG, Barry P Marmion, Simmons A. Mackie and McCartney Practical Medical Microbiology; 14th edition. Churchill Livingstone, London. 1996; 245- 258.
4. Clinical and Laboratory Standard Institute, 2012. Performance standards for antimicrobial susceptibility testing. Clinical and Laboratory Standards Institute, Wayne. 22nd Informational Supplement, 32 (3).
5. Durgadas Naik, Alem Teclu. A study on antimicrobial susceptibility pattern in clinical isolates of Staphylococcus aureus in Eritrea. Pan African Medical Journal, 2009 3:1.
6. Hare Krishna Tiwari, Darshan Sapkota, Malaya Ranjan Sen. High prevalence of multidrug-resistant MRSA in a tertiary care hospital of Northern India. Infection and Drug Resistance 2008: 1; 57-61.
7. Sheetal Verma, Swati Joshi, V Chitnis, Nanda Hemwani, D Chitnis. Growing problem of methicillin resistant staphylococci – Indian scenario. Indian Journal of Medical Sciences year: 2000 / Volume: 54 / Issue: 12 / page: 535-540.
8. Lahari Saikia, Reema Nath, Basabdatta choudhury, Mili sarkar. Prevalence and antimicrobial susceptibility pattern of methicillin-resistant Staphylococcus aureus in Assam. Indian Journal of critical care Medicine, 2009/ volume:13/ issue: 3/ page: 156-158.
9. Vidya Pai, Venkatakrishna I Rao, Sunil P Rao. Prevalence and Antimicrobial Susceptibility pattern of Methicillin-resistant Staphylococcus aureus [MRSA] isolates at a tertiary care hospital in Mangalore, South India. Journal of Laboratory Physicians / Jul-Dec 2010 / Vol-2 / Issue-2.
10. AA Mehta, CC Rodrigues, RR Kumar, AA Rattan, HH Sridhar, VV Mattoo, VV Ginde. A pilot programme of MRSA surveillance in India. (MRSA Surveillance Study Group). Journal of Postgraduate medicine, year: 1996 / Volume: 42 / Issue: 1 / Page: 1-3.
11. Baral R, B Khanal, A Acharya. Antimicrobial susceptibility patterns of clinical isolates of Staphylococcus aureus Health Renaissance 2011; Vol 9 (No. 2): 78-82.
12. Nwankwo Emmanuel Onwubiko, Nasiru Magaji Sadiq. Antibiotic sensitivity pattern of Staphylococcus aureus from clinical isolates in a tertiary health institution in Kano, Northwestern Nigeria. Pan African Medical Journal. 2011; 8:4.
13. Patrick Eberechi Akpaka, Shivnarine Kissoon, William Henry Swanston and Michele Monteil. Prevalence and antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus isolates from Trinidad and Tobago. Annals of Clinical Microbiology and Antimicrobials 2006, 5: 16.
14. Adebayo O Shittu, Johnson Lin. Antimicrobial susceptibility patterns and characterization of clinical isolates of Staphylococcus aureus in KwaZulu-Natal province, South Africa. BMC Infect Dis 2006; 6:125.
15. M. Shanthi, Uma Sekar. Antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus at SriRamachandra medical centre. Sri Ramachandra Journal of Medicine, June 2009, Vol. II, Issue 2.
16. Dr. Bandaru Narasinga Rao, MD, Ph.D., Dr. T. Prabhakar, M.Sc., Ph.D. Prevalence and Antimicrobial Susceptibility pattern of Methicillin Resistant Staphylococcus aureus [MRSA] in and around Visakhapatnam, Andhra Pradesh, India. Journal of Pharmaceutical and Biomedical Sciences [JPBMS].
17. Shilpa Arora, Pushpa Devi, Usha Arora, Bimla Devi. Prevalence of Methicillin-resistant Staphylococcus aureus (MRSA) in a tertiary care Hospital in Northern India. Journal of Laboratory Physicians / Jul-Dec 2010 / Vol-2 / Issue-2.
18. Mehta AP, Rodrigues, C, Sheth K, Jani, S, Hakimiyan A, Fazalbhoy N. Control of methicillin resistant Staphylococcus aureus in a tertiary care centre – A five year study. J Med Microbial 1998; 16: 31-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





