IJCRR - 6(23), December, 2014
Pages: 10-13
Date of Publication: 10-Dec-2014
Print Article
Download XML Download PDF
EVALUATION OF CLINICALLY SIGNIFICANT HYPOCALCEMIA AFTER TOTAL THYROIDECTOMY: A PROSPECTIVE STUDY
Author: Ashim Sarkar, Subhasis Jana, Bijan Basak, Ganesh Chandra Gayen, Santanu Sit, Apurba Sarkar
Category: Healthcare
Abstract:Purpose: Many factors are responsible for the occurrence of hypocalcemia after total thyroidectomy (TT). This study was conducted to look at the factors usually concerned in post TT clinically significant hypocalcemia (CSH). A scoring system is being developed in combination with these factors for early diagnosis of CSH. Study Design: Institution based Prospective study. Materials and Methods: Total 50 patients with benign goiter and early carcinoma thyroid were included in this study and all were go through total thyroidectomy. Age of the patients, pre-operative thyroid hormone status, serum Ca2+ level and 25 (OH) vitamin D were studied. Post-operative iPTH level at 8 hours and calcium level at 12 hours were measured. Condition of parathyroid gland and size of the nodule were studied and preserved during operation. CSH prediction score (0 to 8) was designed based on these 8 factors. Statistical Analysis: SPSS 16 software was used. Independent samples T-test and Chi-square test was used for comparison between two groups. P value < 0.05 was used as statistically significance. Results: There were 8 males and 42females. 64% (n=32) had euthyroid multi-nodular goiters, 24%(n=12) had toxic MNG, and 12%(n=6) had an early carcinoma of thyroid. 30%(n=15) developed CSH. CSH was developed in patients with low pre-operative serum calcium (P=0.000), low 25 OH vitamin D (P=0.001) with low serum calcium (P=0.000) at 10 hours, low post-operative iPTH at 6 hours (P=0.001), after surgery and lesser number of parathyroid identification at surgery (P=0.000)and nodule size (P - 0.000). Conclusions: Clinically significant hypocalcemia (CSH) after TT depends upon multiple factors and these factors (Hypocalcemia prediction score > 3) can be taken account to predict it to discharge patients within one day after surgery.
Keywords: Total thyroidectomy, 25 OH vitamin D3, Clinically significant hypocalcemia, intact PTH.
Full Text:
INTRODUCTION
Temporary symptomatic hypocalcemia occurs in some patients after total thyroidectomy (TT). This is a limiting factor in an early discharge of the patients from hospital1 . The incidence has been reported to vary from 0.5% to 75%2 . Early treatment can be started in these patients who were likely to develop clinically significant hypocalcemia (CSH), and the others, in those the incidence of hypocalcemia is unlikely and can be discharged as a day care surgery. Post-operative serum calcium, post-operative intact PTH (iPTH), serum 25 OH vitamin D levels, pre-operative serum calcium, presence of hyperthyroidism, advanced age of the patient, parathyroid preservation, and size of goiter at surgery have all been implicated in the development of post TT hypocalcemia 2-17. It has been realized from various studies published in literature that no single factor can predict its occurrence 2-17. The study was carried out to consider all these factors and to create a multi-factorial scoring system. We hope that this will facilitate us to predict incidence of post TT clinically significant hypocalcemia and enable us to discharge the patients within one day after surgery
MATERIALS AND METHODS
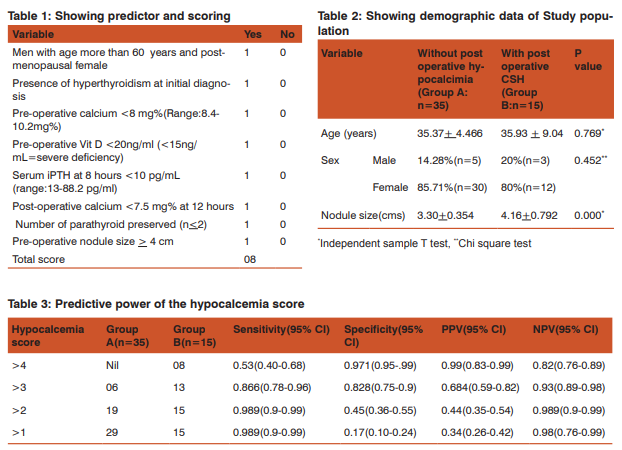
This prospective study was conducted at Burdwan Medcal College and Hospital a rural based medical college and hospital from February 2013 to January 2014. All patients undergo total thyroidectomy for benign thyroid swelling and stage one carcinoma thyroid (< T2/N0/ M0). All surgeries were performed by a surgeon, who is well trained in thyroid surgery. Patients who developed clinically significant hypocalcemia (CSH) within 12 hours of surgery were excluded from the final analysis. Demographics of the study population, status of hyperthyroidism, pre-operative levels of free serum Ca+2 and 25 (OH) vitamin D, post-operative serum parathyroid hormone (iPTH) at 6 hours and serum calcium at 10 hours, nodules size and parathyroid preservation status during operation were recorded. Hypocalcemia prediction score (0 to 8) was designed based on these factors [Table 1]. Post-operative Hypocalcemia was defined as serum calcium < 7.5 mg% occurring anytime after total thyroidectomy. Patients who have low serum calcium (< 7.5 mg %) and develope carpopedal spasm [induced within 2 minutes on eliciting the Trousseau sign (Figure 1)] after total thyroidectomy, said to have clinically significant hypocalcemia (CSH). A minimum of 0 points and maximum of 8 points were chosen to each case. Statistical Analysis: SPSS 16 software was used. Independent samples T-test and Chi-square test was used for comparison between two groups. P value <0.05 was used as statistically significance. A logistic regression analysis model was built to assess the significant predictors. RESULTS Among the 50 patients included in the final analysis; there were 8 males and 42 females (16% and 84%), 64% (n=32) were euthyroid multinodular goiters, 24% (n=12) were toxic MNG, and 12% (n=6) were early carcinoma thyroid. 30% (n=15) developed clinically significant hypocalcemia (CSH) after 24 hours of surgery. Comparison of the patients who developed CSH (group B) with those who did not develop (group A) [SPSS result]. CSH was found in patients with low pre-operative serum Ca2+ (P=0.000), low Serum Vit D (P=0.001), low post-operative iPTH (P=0.001), and low serum Ca2+ (P=0.000) at 6 and 10 hours after surgery respectively. Clinically significant hypocalcemia (CSH) also occurred with lesser number of parathyroid being preserved at surgery (P=0.000) and nodule size (P-0.000). Age of the patient (P=0.3) was not significantly different between the groups. [Table 2] shows the comparison of the demographic data between groups A vs. group B. [Table 3] depicts the predictive power of the different hypocalcemia scores, which will predict clinically significant hypocalcemia. DISCUSSION The most common problem encountered after TT is hypocalcemia, which can either be temporary or be permanent1 . Temporary hypocalcemia can be biochemical (BH) or symptomatic hypocalcemia (SH), which usually develops 24 to 48 hours after the thyroidectomy3 . Thus, patients have to be observed for this time period prior to discharge in order to prevent development of clinically significant hypocalcemia. It is particularly important in India because of the poor rural health care system. Development of post total thyroidectomy (TT) hypocalcemia is depends on various factors. One of them has been postoperative serum calcium levels4 . Pfleiderer et al2 demonstrated that serum calcium less than 7.6 mg% on day 1 after surgery had 95% specificity in predicting SH. In this study we measured the serum calcium level at 10 hours after the TT but Lombardi et al8 used serum calcium at 12 hours after surgery in their study. Lo CY et al5 used serum calcium of 7.2 mg% as cut off to define hypocalcemia. The cut off value is 7.5 mg% in this study. Postoperative as well as intra-operative serum iPTH has been used in various studies to predict post TT hypocalcemia. 3,5-7. An analysis of 9 observational studies by Noordzij et al.3 reported that the level of PTH 6 hours after TT had 96.4% sensitivity and 91.4% specificity in detecting post-operative hypocalcemia. Payne et al6 used iPTH at 6, 12, and 20 hours post-operatively and found the 12 hour value as most sensitive in prediction. Lombardi et al8 used 2, 4, 6, 24, 48 hours post-operatively and found that the 4 hour and 6 hour value had the best predictive value. As there were no specific guidelines for the collection of iPTH sample, iPTH level at 6 hours after surgery was measured in this study. The mean PTH was 13.52 pg/mL in patients who developed hypocalcemia3 . In our study, we found that the post-operative iPTH of ≤10 pg/ mL at 6 hours after surgery. Literature review has shown that intra-operative PTH was less sensitive and specific than when it was checked post-operatively3 . That’s why we used only 6 hour post-operative iPTH value. Serum vitamin D has been found to be low in Indian patients in various studies9,10. Since the serum vitamin D directly influences the calcium kinetics, especially in the post-thyroidectomy scenario, we included pre-operative vitamin D also as a predictive factor11. One study has shown that the low vitamin D levels are associated with 28-fold increase in chances of post TT clinically significant hypocalcemia12. Hyperthyroidism has been shown to have significant impact over bone turn over even after euthyroid status is restored13. Longer duration of Grave’s disease and low vitamin D were shown as factors contributing to hypocalcemia14. Pre-operative calcium levels have been used to predict hypocalcemia post-operatively11. Yamashita et al15 have reported that lower pre-operative calcium levels in patients underwent total thyroidetomy shown early development of hypocalcemia. Erbil et al14 and Dedivitis et al16 observed that elderly patients have significant risk factor for post-operative hypocalcemia. Ageing is said to be associated with decreased intestinal calcium absorption, decreased renal 1α hydroxylase, decreased dermal synthesis of vitamin D, these contribute to susceptibility to hypocalcemia after TT14. In this study, we found post-menopausal women and men > 60 years are susceptible to hypocalcemia. We also found that the age was insignificant parameter in predicting clinically significant hypocalcemia . Preservation of parathyroid gland is inversely proportional for the development of post total thyroidectomy (TT) hypocalcemia. Some authors have suggested that at least 3 parathyroids are to be saved while others opined that 2 functional glands are enough to prevent post TT hypocalcemia17. In our study, in patients with 2 or <2 parathyroid gland developed clinically significant hypocalcemia. It has been shown that the post-operative hypocalcemia is also dependant on the surgeons experience and the operative technique used17.
CONCLUSION
CSH after TT depends upon multiple factors and these factors can be taken account to predict it to discharge patients within one day after surgery. Further studies are needed to authenticate the scoring system.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of funding: None Conflict of interest: None Declared
References:
1. Pradeep PV, Ramalingam K, Jayashree B. Post total thyroidectomy hypocalcemia: A novel multif-factorial scoring system to enable its prediction to facilitate an early discharge. J Postgrad Med 2013;59:4-8.
2. Pfleiderer AG, Ahamd N, Draper MR, Vrotsou K, Smith WK. The timing of calcium measurements in helping to predict temporary and permanent hypocalcemia in patients having completion and total thyroidectomies. Ann R Coll Surg Engl 2009;91:140-6.
3. Noordzij JP, Lee SL, Bernet VJ, Payne RJ, Cohen SM, McLeod IK, et al. Early prediction of Hypocalcemia after Thyroidectomy using Parathyroid hormone: An analysis of pooled individual data from nine observational studies. J Am Coll Surg 2007;205:748-54.
4. Husein M, Hier MP, Al Abdulhadi K, Black M. Predicting calcium status post thyroidectomy with early calcium levels. Otolaryngol Head Neck Surg 2002;127:289-93.
5. Lo CY, Luk JM, Tam SC. Applicability of intra operative parathyroid hormone assay during thyroidectomy. Ann Surg 2002;236:564-9.
6. Payne RJ, Hier MP, Tamilia M. Post operative parathyroid hormone level as a predictor of post thyroidectomy hypocalcemia. J Otolaryngol 2003;32:362-7.
7. Soon PS, Magarey CJ, Campbell P, Jalaludin B. Serum intact PTH as a predictor of hypocalcemia after total thyroidectomy. ANZ J Surg 2005;132:584-6.
8. Lombardi CP, Raffaelli M, Prince P. Early prediction of post thyroidectomy hypocalcemia by a single iPTH measurement. Surgery 2004;136:1236-40.
9. Babu US, Calvo MS. Modern India and Vit D dilemma: Evidence for the need of a national food fortification program. Mol Nutr Food Res 2010;54:1134-47.
10. Khadgawat R, Brar KS, Gahlo M, Yadav CS, Malhotra R, Guptat N, et al. High prevalence of Vitamin D deficiency in Asian Indian patients with fragility hip fracture: A pilot study. J Assoc Physicians India 2010;58:539-42.
11. Erbil Y, BozborsA, Ozbey N. Predictive value of age and serum parathormone and vitamin D3 levels for post operative hypocalcemia after total thyroidectomy for non toxic multinodular goiter Arch Surg 2007;142:1182-7.
12. Erbil Y, Barbaros U, Temel B, Turkoglu U, Issever H, Bozbora A. The impact of age, vitamin D(3) level, and incidental parathyroidectomy on postoperative hypocalcemia after total or near total thyroidectomy. Am J Surg 2009;197:439- 46.
13. Biet A, Zaatar R, Strunski V. Post operative complications in total thyroidectomy for Graves’s disease: Comparison with multinodular benign goiter surgery. Ann Otolaryngol Chir Cervicofac 2009;126:190-5.
14. Erbil Y, Ozbey NC, Sari S, Unalap AR, Agcaoglu O, Ersoz F, et al. Determinants of post operative hypocalcemia in vitamin D deficient Graves’ patients after total thyroidectomy. Am J Surg 2011;201:678-84.
15. Yamashita H, Murakami T, Noguchi S. Post operative tetany in Graves, disease. Important role of vitamin D metabolites. Ann Surg 1998;229:237-45.
16. Dedivitis RA, Pfuetzenreiter EG Jr, Nardi CE, Barbara EC. Prospective study of clinical and laboratorial hypocalcemia after thyroid surgery. Braz J Otorhinolaryngol 2010;76:71- 7.
17. Thomusch O, Machens A, Sekulla C, Ukkat J, Brauckhoff M, Dralle H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: A multivariate analysis of 5846 consecutive patients. Surgery 2003;133:180-5.
18. Kotan C, Kosem M, Alquan E, Ayakta H, Sonmez R, Soylemez O. Influence of the refinements of surgical technique and surgeons experience on the rate of complications after total thyroidectomy for benign thyroid disease. Acta Chir Belg 2003;103:278-81.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





